
Abstract
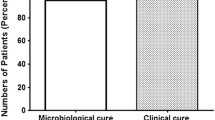
Serum, urine and renal levels of fleroxacin were evaluated in normal andEscherichia coli-infected kidneys from 1 to 48 hours after either a single or 14 (every 12 hours) injections of 50 mg/kg. All treatments were started 24 hours after the induction of infection. Fleroxacin did not accumulate in normal or infected renal tissue, with serum and tissue concentrations of fleroxacin lower than the limit of detection 24 hours after the cessation of therapy. Following a single injection, the area under the concentration curves of fleroxacin in the serum, cortex and medulla of infected animals were significantly higher than those in normal rats (P<0.05) and peak concentrations of fleroxacin in the cortex and the medulla were greater than 800 times the MIC of theE. coli strain, and remained above the MIC for 12 hours after the cessation of therapy. Fleroxacin given twice a day at a dose of 25 mg/kg or as a single daily dose of 50 mg/kg for 14 days sterilized 100% of the infected kidneys and urines for up to 6 months following the cessation of therapy. These 2 regimens were more effective than alternative therapy with tobramycin (10 mg/kg every 12 hours for 3 days) combined with trimethoprim (10 mg/kg every 12 hours for 14 days). However, fleroxacin, at 50 mg/kg every 48 hours, was no more effective than the combination of tobramycin and trimethoprim. These results demonstrate that the intrarenal distribution of fleroxacin is altered in the presence of pyelonephritis. The long tissue half-life combined with a high therapeutic ratio permits single daily fleroxacin dosing in patients with severe pyelonephritis.
Similar content being viewed by others


References
Paton JH, Reeves DS. Fluoroquinolone antibiotics. Microbiology, pharmacokinetics and clinical use. Drugs 1988; 36:193–228.
Wolfson JS, Hooper DC. Fluoroquinolones antimicrobial agents. Clin Microbiol Rev 1989;2:378–424.
Aoyama H, Inoue M, Mitsuhashi S. In-vitro and in-vivo antibacterial activity of fleroxacin, a new fluorinated quinolone. J Antimicrob Chemother 1988;22:99–114.
Hirai K, Aoyama H, Hosaka M, Oomori Y, Niwata Y, Suzue S, et al. In vitro and in vivo antibacterial activity of AM-833, a new quinolone derivative. Antimicrob Agents Chemother 1986;29:1059–1066.
Nakashima M, Kanamaru M, Uematsu T, Takiguchi A, Mizuno A, Itaya T, et al. Clinical pharmacokinetics and tolerance of fleroxacin in healthy male volunteers. J Antimicrob Chemother 1988;22:133–144.
Stuck AE, Kim DK, Frey FJ. Fleroxacin clinical pharmacokinetics. Clin Pharmacokinet 1992;22:116–131.
Weidekamm E, Portmann R, Suter K, Partos C, Dell D, Lucker PW. Single- and multiple-dose pharmacokinetics of fleroxacin, a trifluorinated quinolone, in humans. Antimicrob Agents Chemother 1987;31:1909–1914.
Wise R, Kirkpatrick B, Ashby J, Griggs DJ. Pharmacokinetics and tissue penetration of Ro 23-6240, a new trifluoroquinolone. Antimicrob Agents Chemother 1987; 31:160–163.
Kusajima H, Ishikawa N, Machida M, Uchida H, Irikura T. Pharmacokinetics of a new quinolone, AM-833, in mice, rats, rabbits, dogs and monkeys. Antimicrob Agents Chemother 1986;30:304–309.
Balfour JA, Todd PA, Peters DH. Fleroxacin. A review of its pharmacology and therapeutic efficacy in various infections. Drugs 1995;49:794–850.
Bergeron MG, Beauchamp D, Poirier A, Bastille A. Continuous vs intermittent (pulse) administration of antimicrobial agents: tissue penetration and in vivo efficacy. Rev Infect Dis 1981;3:84–97.
Trottier S, Bergeron MG: Intrarenal concentrations of ampicillin in acute pyelonephritis. Antimicrob Agents Chemother 1981;19:761–765.
Bergeron MG, Trottier S, Lessard C, Beauchamp D, Gagnon PM. Disturbed intrarenal distribution of gentamicin in experimental pyelonephritis due toEscherichia coli. J Infect Dis 1982;146:436–439.
Beauchamp D, Poirier A, Bergeron MG. Increased nephrotoxicity of gentamicin in pyelonephritic rats. Kidney Int 1985;28:106–113.
Beauchamp D, Bouchard A, Thériault G, Pellerin M, Bergeron MG. Effect ofE. coli pyelonephritis on the intrarenal accumulation kinetics of gentamicin and netilmicin in rats. Clin Invest Med 1990;13:145–151.
Jullien M, Thériault G, Bergeron MG, Beauchamp D. Effect ofE. faecalis pyelonephritis on the intracortical accumulation kinetics of gentamicin in rats. Can J Infect Dis 1990;1:117–120.
Bergeron MG. Treatment of pyelonephritis in adults. Med Clin North Am 1995;79:619–649.
Beauchamp D, Bergeron MG. Pharmacological principles of pyelonephritis treatment—distribution, efficiency and renal toxicity of antibiotics. Medecine/Sciences 1997; 13:942–951.
Ritzerfeld W. Comparative studies of fleroxacin and ofloxacin in experimental pyelonephritis. J Antimicrob Chemother 1988;22:119–122.
Morck DW, Olson ME, McKay SG, Lam K, Prosser B, Cleeland R, Costerton JW. Therapeutic efficacy of fleroxacin for eliminating catheter-associated urinary tract infection in a rabbit model. Am J Med 1993;94:S23-S30.
Lecomte F, Thauvin-Eliopoulos C, Le-Boete I, Grise G, Lemeland JF. Treatment of experimentalEscherichia coli pyelonephritis in rats by ciprofloxacin in comparison with tobramycin. Scand J Infect Dis 1990;22:75–78.
Kaye D. The effect of water diuresis on spread of bacteria through the urinary tract. J Infect Dis 1971;124:297–305.
Norman M. APL computer program for the analytical and numerical integration of hormonal disappearance data. Can J Physiol Pharmacol 1972;50:845–852.
Bergeron MG, Bastille A, Lessard C, Gagnon PM. Significance of intrarenal concentrations of gentamicin for the outcome of experimental pyelonephritis in rats. J Infect Dis 1982;146:91–96.
Bergeron MG, Bergeron Y. Influence of endotoxin on the intrarenal distribution of gentamicin, netilmicin, tobramycin, amikacin and cephalothin. Antimicrob Agents Chemother 1986;29:7–12.
Trottier S, Bergeron MG, Lessard C. Intrarenal distribution of trimethoprim and sulfamethoxazole. Antimicrob Agents Chemother 1980;17:383–388.
Bergeron MG, Marois Y. Benefit from high intrarenal levels of gentamicin in the treatment ofE. coli pyelonephritis. Kidney Int 1986;30:481–487.
Weidekamm E, Portmann R. Penetration of fleroxacin into body tissue and fluids. Am J Med 1993;94:75S-80S.
Naber KG, Sigl G. Fleroxacin versus ofloxacin in patients with complicated urinary tract infection: a controlled clinical study. Am J Med 1993;94:S114-S117.
Cox CE. Comparison of intravenous fleroxacin with ceftazidime for treatment of complicated urinary tract infections. Am J Med 1993;94:S118-S125.
Taufer M, Pummer K, Primus G. Fleroxacin vs norfloxacin in therapy for complicated urinary tract infections: a randomized, multidose, double-blind study. Rev Infect Dis 1989;11:S1353.
Childs SJ. Fleroxacin versus norfloxacin for oral treatment of serious urinary tract infections. Am J Med 1993;94: S105-S107.
Plummer K. Fleroxacin versus norfloxacin in the treatment of urinary tract infections: a multicenter, double-blind, prospective, randomized, comparative study. Am J Med 1993;94:S108-S113.
Iravani A. Multicenter study of single-dose and multiple-dose fleroxacin versus ciprofloxacin in the treatment of uncomplicated urinary tract infections. Am J Med 1993; 94:S89-S96.
Whitby M, Brown P, Silagy C, Rana C. Comparison of fleroxacin and amoxicillin in the treatment of uncomplicated urinary tract infections in women. Am J Med 1993; 94:S97-S100.
Auclair P, Tardif D, Beauchamp D, Gourde P, Bergeron MG. Prolonged endotoxemia enhances the renal injuries induced by gentamicin in rats. Antimicrob Agents Chemother 1990;34:889–895.
Author information
Authors and Affiliations
About this article
Cite this article
Leclerc, F., Morin, N.J., Bergeron, M.G. et al. Relationship between intrarenal distribution and efficacy of fleroxacin in the treatment ofEscherichia coli pyelonephritis in rats. J Infect Chemother 4, 188–194 (1998). https://doi.org/10.1007/BF02490165
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02490165