
Abstract
Background: More than half of the cases of breast cancer treated in the United States occur in women over age 65. This study investigates age-related differences in breast cancer therapy.
Methods: A retrospective review of all women with primary operable invasive breast cancer treated at the University of Michigan Breast Care Center over a 30-month period showed a total of 77 older patients aged ⩾65 years (median, 71; oldest patient, 92) for whom full information was available regarding comorbidity, tumor stage and histology, and details of surgery, radiation, and chemohormonal therapy and complications. Fifty-one similar younger patients aged 55–64 years (median, 59) were identified for comparison. Patients were classified as either having received standard treatment or nonstandard treatment. Standard therapy was prospectively defined as follows: local/regional—lumpectomy and axillary lymph node dissection plus radiation therapy or modified radical mastectomy; systemic—chemotherapy and/or tamoxifen for stage II disease. A comorbidity score calculated for each patient assigned one point each for nursing home residence, nonambulatory status, recent surgery, and each medical problem requiring drug therapy.
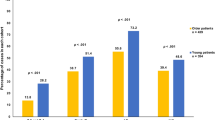
Results: When overall treatment (local/regional plus systemic) was assessed, proportionately fewer older patients (55 of 77 versus 47 of 51;p<0.01) received standard treatment. Fewer older than younger patients (62 of 77 versus 50 of 51;p<0.01) received surgical therapy that included an axillary dissection. A smaller proportion of older patients received radiation therapy following lumpectomy and axillary lymph node dissection (26 of 29 versus 19 of 19; N.S.). Overall, only 59 of 77 older patients versus 50 of 51 younger patients (p<0.001) received standard local/regional care. Similar proportions of younger and older patients (19 of 22 and 24 of 30, respectively) received standard systemic therapy for stage II breast cancer, but older patients were less likely to receive chemotherapy than younger patients (7% versus 50%;p<0.001). Treatment-related complications were not age-related but were more frequent in patients receiving standard treatment than in patients receiving nonstandard treatment (45 of 102 versus two of 26;p<0.001). Comorbidity score correlated with the use of nonstandard therapy but not with age. The scores for both older and younger patients receiving overall standard treatment were 0.8 versus 1.5 and 1.4, respectively, in patients receiving nonstandard treatment. Interestingly, explanations for decisions to deviate from standard treatment guidelines were often not identified. Comorbidity was explicitly noted in only one of four younger patients who received nonstandard treatment therapy. In 22 older patients who received nonstandard treatment, comorbidity was cited in eight cases, patient age was cited in six cases, and patient choice was cited in four cases. Follow-up (median, 34 months) did not show that disease-free or overall survival differences were related to age or to treatment (standard versus nonstandard).
Conclusions: These data demonstrate age-related variations in breast cancer treatment in a multidisciplinary breast care unit. Lower complication rates and equivalent short-term outcomes in women who received nonstandard therapy suggest good clinical judgment may have played a role in these differences. Although age-related patient preferences and comorbidity are relevant, the age-related attitudes of caregivers must also be taken into account to fully explain these variations.
Similar content being viewed by others

References
Boring CC, Squires TS, Tong T. Cancer statistics, 1991.Ca Cancer J Clin 1991;41:19–36.
Stewart JA, Foster RS. Breast cancer and aging.Semen Oncol 1989;16:41–50.
Vinokur AD, Threatt BA, Caplan RD, Zimmerman BL. Physical and psychosocial functioning and adjustment to breast cancer. Long-term follow-up of a screening population.Cancer 1989;63:394–405.
Vinokur AD, Threatt BA, Vinokur-Kaplan D, Satariano WA. The process of recovery from breast cancer for younger and older patients. Changes during the first year.Cancer 1990;65:1242–54.
Vinokur AD, Vinokur-Kaplan D. “In sickness and in health.” Patterns of social support and undermining in older married couples.J Aging Health 1990;2:215–41.
Davis SJ, Karrer FW, Moor BJ, Rose SG, Eakins G. Characteristics of breast cancer in women over 80 years of age.Am J Surg 1985;150:655–8.
Robins RE, Lee D. Carcinoma of the breast in women 80 years of age and older: still a lethal disease.Am J Surg 1985;149:606–9.
Hunt KE, Fry DE, Bland KI. Breast carcinoma in the elderly patient: an assessment of operative risk, morbidity and mortality.Am J Surg 1980;140:339–42.
Herbsman H, Feldman J, Seldera J, Gardner B, Alfonso A. Survival following breast cancer surgery in the elderly.Cancer 1981;47:2358–63.
Kantrowitz DA, Poulter CA, Sischy B, et al. Treatment of breast cancer among elderly women with segmental mastectomy plus postoperative radiotherapy.Int J Radiat Oncol Biol Phys 1988;15:263–70.
Toonkel LM, Fix I, Jacobson LH, Bamberg N. Management of elderly patients with primary breast cancer.Int J Radiat Oncol Biol Phys 1988;14:677–81.
Handel N, Silverstein MJ, Waisman E, Waisman J. Reasons why mastectomy patients do not have breast reconstruction.Plast Reconstr Surg 1990;86:1118–22.
Begg CB, Carbone PP. Clinical trials and drug toxicity in the elderly. The experience of The Eastern Cooperative Oncology Group.Cancer 1983;52:1986–92.
Walsh SJ, Begg CB, Carbone PP. Cancer chemotherapy in the elderly.Semin Oncol 1989;16:66–75.
Castiglione M, Gelber RD, Goldhirsch A. Adjuvant systemic therapy for breast cancer in the elderly: competing causes of mortality.J Clin Oncol 1990;8:519–26.
Allen C, Cox EB, Manton KG, Cohen HJ. Breast cancer in the elderly. Current patterns of care.J Am Geriatr Soc 1986;34:637–42.
Schain WS. Reasons why mastectomy patients do not have breast reconstruction (discussion).Plast Reconstr Surg 1990;86:1123–5.
Chu J, Diehr P, Feigel P, et al. The effect of age on the care of women with breast cancer in community hospitals.J Gerontol 1987;42:185–90.
Silliman RA, Guadagnoli E, Weitberg AB, et al. Age as a predictor of diagnostic and initial treatment intensity in newly diagnosed breast cancer patients.J Gerontol 1989;44:M46–50.
Samet J, Hunt WC, Key C, Humble CG, Goodwin JS. Choice of cancer therapy varies with age of patient.JAMA 1986;255:3385–90.
Becker TM, Goodwin JS, Hunt WC, Key CR, Samet JM. Survival after cancer surgery of elderly patients in New Mexico.J Am Geriatr Soc 1989;37:155–9.
Greenfield S, Blanco DM, Elashoff RM, Ganz PA. Patterns of care related to age of breast cancer patients.JAMA 1987;257:2766–70.
Schleifer SJ, Bhardwaj S, Lebovits A, Tanaka JS, Messe M, Strain JJ. Predictors of physician nonadherence to chemotherapy regimens.Cancer 1991;67:945–51.
Bergman L, Dekker G, van Leeuwen FE, Huisman SJ, van Dam FSAM, Van Dongen JA. The effect of age on treatment choice and survival in elderly breast cancer patients.Cancer 1991;67:2227–34.
Swanson GM, Satariano ER, Satariano WA, Osuch JR. Trends in conserving treatment of invasive carcinoma of the breast in females.Surg Gynecol Obstet 1990;171:465–71.
Beahrs OH, Henson DE, Hutter RVP, Myers MH.Manual for staging of cancer. 3rd ed. Philadelphia: Lippincott, 1988:145–50.
August DA, Carpenter LC, Harness JK, et al. The benefits of a multidisciplinary approach to breast care.J Surg Oncol 53:161–7, 1993.
Yancik Y, Ries LG. Cancer in the aged. An epidemiologic perspective on treatment issues.Cancer 1991;68:2502–10.
Peters H. Breast cancer: lay notions and coping strategies. Master's thesis, University of North Carolina, Chapel Hill, 1976.
Westbrook MT, Viney LL. Age and sex differences in patients' reactions to illness.J Health Soc Behav 1983;24:313–24.
Kohn M, Menon G. Life prolongation: views of elderly outpatients and health care professionals.J Am Geriatr Soc 1988;36:840–4.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
August, D.A., Rea, T. & Sondak, V.K. Age-related differences in breast cancer treatment. Annals of Surgical Oncology 1, 45–52 (1994). https://doi.org/10.1007/BF02303540
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02303540