
Abstract
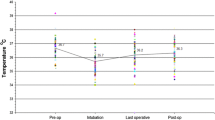
PURPOSE: Perioperative hypothermia has been shown to be an important determinant of outcome after open colorectal resections. The degree of hypothermia occurring with laparoscopic-assisted colorectal surgery is, however, unknown, and the effectiveness of standard warming measures is untested. This study was designed to assess hypothermia in open and laparoscopic-assisted colonic resections using a standardized warming protocol. METHODS: A prospective, nonrandomized study was performed with temperature measurements recorded every ten minutes. Statistical analysis was based on repeated measures analysis of variance models with significance set at the conventional 95 percent (two tailed). RESULTS: A total of 107 patients were entered into the trial; 68 had open and 39 had laparoscopic colectomies. The groups were well matched for age, weight, and duration of surgery, with a median operating time of 180 minutes in each group. The average drop in temperature from commencement of surgery to lowest point was 0.68°C (standard deviation, 0.08) in the open group, compared with 0.53°C (standard deviation, 0.06) in the laparoscopic group (P=0.126). CONCLUSIONS: Laparoscopic-assisted colorectal surgery is not associated with a higher incidence of perioperative hypothermia than open colorectal surgery using a standard warming regimen for both groups. On the basis of these results, standard temperature conservation is adequate, even for long complex laparoscopic procedures.
Similar content being viewed by others


References
Kurz A, Sessler DI, Lenhardt R. Perioperative normothermia to reduce the incidence of surgical wound infection and shorten hospitalisation. New Engl J Med 1996;334:1209–15.
Frank SM, Beattie C, Christopherson R,et al. Unintentional hypothermia is associated with postoperative myocardial ischaemia. Anesthesiology 1993;78:468–76.
Frank SM, Higgins MS, Breslow MJ,et al. The catecholamine, cortisol and hemodynamic responses to mild perioperative hypothermia. Anesthesiology 1995;82:83–93.
Rodriguez JL, Weissman C, Damansk MC,et al. Physiologic requirements during rewarming. Crit Care Med 1983;11:490–7.
Matsukawa T, Sessler DI, Sessler AM,et al. Heat flow and distribution during induction of general anaesthesia. Anesthesiology 1995;82:662–73.
Joachimsson PO, Hedstrand U, Tabow F, Hansson B. Prevention of intraoperative hypothermia during abdominal surgery. Acta Anaesthesiol Scand 1987;31:330–7.
Ott DE. Laparoscopic hypothermia. J Laparoendosc Surg 1991;1:127–31.
Ott DE. Correction of laparoscopic insufflation hypothermia. J Laparoendosc Surg 1991;1:183–6.
Figuardo E, Canosa L. Can hypothermia be evidenced during laparoscopic cholecystectomy? Surg Laparosc Endosc 1997;7:373–83.
Stitz RW, Lumley JW. Laparoscopic resection for colorectal cancer an Australian perspective. Semin Laparosc Surg 1995;2:235–41.
Nolph K. Management of the patient with renal failure. In: Brenner B, Rector F, eds. The kidney. Philadelphia: WB Saunders, 1988:1858.
Russell SH, Freeman JW. Comparison of bladder, oesophageal and pulmonary artery temperatures in major abdominal surgery. Anaesthesia 1996;51:338–40.
Lilly JK, Boland JP, Zekan S. Urinary temperature monitoring: a new index of body core temperature. Crit Care Med 1980;8:742–44.
Erikson RS, Kirklin SK. Comparison of ear-based, bladder, oral and axillary methods for core temperature measurement. Crit Care Med 1993;21:1528–34.
Sessler DI. Perianaesthetic thermoregulation and heat balance in humans. FASEB J 1993;7:638–44.
Leslie K, Sessler DI, Bjorksten AR,et al. Propofol causes a dose dependent decrease in the thermoregulatory threshold for vasoconstriction but has little effect on sweating. Anaesthesiology 1994;81:353–60.
Joris J, Ozaki M, Sessler DI,et al. Epidural anaesthesia impairs both central and peripheral thermoregulatory control during general anaesthesia. Anaesthesiology 1994;80:268–77.
Baxter JN, O'Dwyer PJ. Pathophysiology of laparoscopy. Br J Surg 1995;82:1–2.
Author information
Authors and Affiliations
Additional information
This study was conducted at the Royal Brisbane Hospital and Wesley Medical Centre in Brisbane, Australia.
About this article
Cite this article
Stewart, B.T., Stitz, R.W., Tuch, M.M. et al. Hypothermia in open and laparoscopic colorectal surgery. Dis Colon Rectum 42, 1292–1295 (1999). https://doi.org/10.1007/BF02234217
Issue Date:
DOI: https://doi.org/10.1007/BF02234217