
Abstract
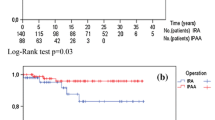
PURPOSE: This study was designed to estimate the efficiency of the various methods used to treat familial adenomatous polyposis coli. METHODS: Three hundred ninety patients (219 males) underwent surgery for familial adenomatous polyposis coli; postoperative follow-up was from 1 to 30 years. RESULTS: Coloproctectomy with preservation of the anal sphincter and coloproctectomy with ileoanal pull-through procedures resulted in development of anal canal cancer in 3 (4.1 percent) of 74 patients. Follow-up revealed development of cancer in the large bowel in 26 (10.7 percent) of 242 patients, in whom colectomy with preservation of various colonic segments was performed. CONCLUSIONS: The occurrence rate of cancer is not significantly related to patients' gender, age, length of preserved colonic segment, presence of cancer in the removed colonic segment, or postoperative follow-up period; however, presence of polyps in the colonic segments preserved during surgery significantly increased the risk of development of cancer at a later time.
Similar content being viewed by others

References
Harvey JC, Quan SH, Stearns MW. Management of familial polyposis with preservation of the rectum. Surgery 1978;84:476–82.
Moertel CG, Hill JR, Adson MA. Management of multiple polyposis of the large bowel. Cancer 1971;28:160–4.
Schroder H, Dorow C. Familial intestinal polyposis—clinical pictures and results of treatment. Coloproctology 1991;13:14–20.
Bussey HJ. Familial polyposis coli: family studies, hystopathology, differential diagnosis and results of treatment. Baltimore: John Hopkins University Press, 1975.
Bess MA, Adson MA, Elveback LR, Moertel CG. Rectal cancer following colectomy for polyposis. Arch Surg 1980;115:460–7.
Cohen Z, McLeod RS, Stern H, Grant D, Nordgren S. The pelvic pouch and ileoanal anastomosis procedure: surgical technique and initial results. Am J Surg 1985;150:601–7.
Emblem R, Bergan A, Larsen S. Straight ileoanal anastomosis with preserved anal mucosa for ulcerative colitis and familial polyposis. Scand J Gastroenterol 1988;23:913–9.
Heimann TM, Gelernt I, Salky B, Bauer J, Greenstein A, Beck AR. Familial polyposis coli: results of mucosal proctectomy with ileoanal anastomosis. Dis Colon Rectum 1987;30:424–7.
Oresland T, Fasth S, Nordgren S, Hulten L. The clinical and functional outcome after restorative proctocolectomy: a prospective study in 100 patients. Int J Colorectal Dis 1989;4:50–6.
Utsunomiya J, Iwama T, Imajo M,et al. Total colectomy mucosal proctectomy and ileoanal anastomosis. Dis Colon Retum 1980;23:459–66.
Dogle NV, Yurkovich AJ. The disease and loss of the ability for work. Moscow: Meditzina, 1984:67.
Sarre RG, Jagelman DG, Beck GJ,et al. Colectomy with ileorectal anastomosis for familial adenomatous polyposis: the risk of rectal cancer. Surgery 1987;101:20–6.
DeCosse JJ, Adams MB, Condon RE. Familial polyposis. Cancer 1977;39:267–73.
Gingold BS, Jagelman D, Turnbull RB. Surgical management of familial polyposis and Gardner's syndrome. Am J Surg 1979;137:54–6.
Bulow S. The risk of developing rectal cancer after colectomy and ileorectal anastomosis in Danish patients with polyposis coli. Dis Colon Rectum 1984;27:726–9.
Feinberg SM, Jagelman DG, Sarre RG,et al. Spontaneous resolution of rectal polyps in patients with familial polyposis following abdominal colectomy and ileorectal anastomosis. Dis Colon Rectum 1988;31:169–75.
Schaupp WC, Volpe PA. Management of diffuse colonic polyposis. Am J Surg 1972;124:218–22.
Author information
Authors and Affiliations
About this article
Cite this article
Nikitin, A.M., Obukhov, V.K., Chubarov, Y.Y. et al. Results of a thirty-year study of familial adenomatous polyposis coli. Dis Colon Rectum 40, 679–684 (1997). https://doi.org/10.1007/BF02140897
Issue Date:
DOI: https://doi.org/10.1007/BF02140897