
Abstract
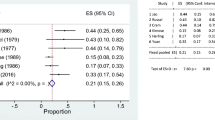
PURPOSE: Surgery for colorectal radiation injury is technically difficult and often followed by complications. This study evaluates factors affecting outcome. METHODS: A retrospective 30-year review was carried out. Preoperative characteristics and operative variables were correlated with morbidity, mortality, and success in providing symptomatic relief. RESULTS: A total of 60 cases and 75 colon and rectal lesions were analyzed. After surgery, the morbidity rate was 65 percent, and the mortality was 6.7 percent. A successful outcome in providing symptomatic relief was achieved in 71.7 percent of cases. When comparing success after operations for the different lesions (stricture, 78.1 percent; hemorrhage, 64.3 percent; perforation, 100 percent; and fistula, 54.5 percent), the presence of a fistula was associated with symptomatic relief significantly less often than the remainder (P=0.03).The type of operation had no effect on success rate: 72 percent for diversion, 66.7 percent for resection, and 83.3 percent for bypass. Morbidity and mortality rates were not significantly influenced by site of lesions, type of lesions, or choice of surgical operation. A permanent stoma was necessary in 70 percent of patients. CONCLUSIONS: The morbidity for surgical treatment of large bowel radiation injury is substantial, and largely unrelated to the type and location of the radiation lesion, as well as the type of operation. Success rates are reasonably high, but worst after fistula repair. The selection of therapy (medical, endoscopic, surgical) for radiation-induced colorectal lesions must take into account numerous factors and be highly individualized.
Similar content being viewed by others

References
Aldridge AH. Intestinal injuries resulting from irradiation treatment of uterine carcinoma. Am J Obstet Gynecol 1942;44:833–54.
Requarth W, Roberts S. Intestinal injuries following irradiation of pelvic viscera for malignancy. Arch Surg 1956;73:682–8.
Schmitt EH III, Symmonds RE. Surgical treatment of radiation induced injuries of the intestine. Surg Gynecol Obstet 1981;153:896–900.
Cochrane JP, Yarnold JR, Slack WW. The surgical treatment of radiation injuries after radiotherapy for uterine carcinoma. Br J Surg 1981;68:25–8.
Perez CA, Breaux S, Bedwinek JM,et al. Radiation therapy alone in the treatment of carcinoma of the uterine cervix: analysis of complications. Cancer 1984;54:235–46.
Harling H, Balsev I. Surgical treatment of radiation injury to the rectosigmoid. Acta Chir Scand 1986;152:691–3.
Shellito PC. Radiation injuries to the rectum. In: Condon RE, Zuidema GS, eds. Surgery of the alimentary tract. Vol. 4. Philadelphia: WB Saunders, 1991:367–80.
Villasanta U. Complications of radiotherapy for carcinoma of the uterine cervix. Am J Obstet Gynecol 1972;114:717–26.
Anseline PF, Lavery IC, Fazio VW, Jagelman DG, Weakley FL. Radiation injury of the rectum: evaluation of surgical treatment. Ann Surg 1981;194:716–24.
Galland RB, Spencer J. Surgical management of radiation enteritis. Surgery 1986;99:133–8.
Novak JM, Collins JT, Donowitz M. Effects of radiation on the human gastrointestinal tract. J Clin Gastroenterol 1976;1:9–39.
Kinsella TJ, Bloomer WD. Tolerance of the intestine to radiation therapy. Surg Gynecol Obstet 1980;151:273–84.
DeCosse JJ, Rhodes RS, Wentz WB, Reagan JW, Dworken HJ, Holden WD. The natural history and management of radiation induced injury of the gastrointestinal tract. Ann Surg 1969;170:369–84.
Deitel M, Vasic V. Major intestinal complications of radiotherapy. Am J Gastroenterol 1979;72:65–70.
Deveney CW, Lewis FR, Schrock TR. Surgical management of radiation injury of the small and large intestine. Dis Colon Rectum 1976;19:25–9.
Berken CA. Nd:YAG laser therapy for gastrointestinal bleeding due to radiation colitis. Am J Gastroenterol 1985;80:730–1.
Ahlquist DA, Gostout CJ, Viggiano TR, Pemberton JH. Laser therapy for severe radiation induced rectal bleeding. Mayo Clin Proc 1986;61:927–31.
Triadafilopoulous G, Sarkisian M. Dilatation of radiation induced sigmoid stricture using sequential Savary-Guilliard dilators. Dis Colon Rectum 1990;33:1065–7.
Cooke SA, de Moor NG. The surgical treatment of the radiation damaged rectum. Br J Surg 1981;68:488–92.
Jao SW, Beart RW, Gunderson LL. Surgical treatment of radiation injuries of the colon and rectum. Am J Surg 1986;151:272–7.
Nowacki, MP, Szawlowski AW, Borkowski A. Parks' coloanal sleeve anastomosis for treatment of postirradiation rectovaginal fistula. Dis Colon Rectum 1986;29:817–20.
Hatcher PA, Thomson HJ, Ludgate SN, Small WP, Smith AN. Surgical aspects of intestinal injury due to pelvic radiotherapy. Ann Surg 1985;99:133–8.
Galland RB, Spencer J. Surgical management of radiation enteritis. Surgery 1986;99:133–8.
Gazet JC. Parks' coloanal pull-through anastomosis for severe complicated radiation proctitis. Dis Colon Rectum 1985;28:110–4.
Kimose HH, Fischer L, Spjeldnaes N, Wara P. Late radiation injury of the colon and rectum-surgical management and outcome. Dis Colon Rectum 1989;32:684–9.
Aitken RJ, Elliot MS. Sigmoid exclusion: a new technique in the management of radiation induced fistula. Br J Surg 1985;72:731–2.
Drake DB, Pemberton JH, Beart RW, Dozois RR, Wolff BG. Coloanal anastomosis in the management of benign and malignant rectal disease. Ann Surg 1987;206:600–5.
Browning GGP, Varma JS, Smith AN, Small WP, Duncan W. Late result of mucosal proctectomy and coloanal sleeve anastomosis for chronic irradiation rectal injury. Br J Surg 1987;74:31–4.
Nicholls RJ, Lubrowsky DZ, Donaldson DR. Comparison of colonic reservoir and straight coloanal reconstruction after rectal excision. Br J Surg 1988;75:318–20.
Author information
Authors and Affiliations
About this article
Cite this article
Pricolo, V.E., Shellito, P.C. Surgery for radiation injury to the large intesine. Dis Colon Rectum 37, 675–684 (1994). https://doi.org/10.1007/BF02054411
Issue Date:
DOI: https://doi.org/10.1007/BF02054411