
Abstract
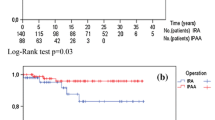
To compare the clinical and functional results of ileorectostomy (IR) and ileal pouch-anal anastomosis (IPAA) in patients with familial adenomatous polyposis (FAP), we reviewed the results of 94 IPAA patients and 21 IR patients who were operated upon between 1978 and 1988. The groups were similar with respect to age and sex. None of the patients died postoperatiyely. Postoperative complications occurred in 28 percent of the IPAA group and in 17 percent of the IR group (P >0.1). Seven percent of IPAA patients described symptoms compatible with pouchitis. Sixty-one percent of IR patients required subsequent fulguration of rectal polyps at least once. IR patients had a mean (±SD) of 4 (±2) stools per day, while IPAA patients had 5 (±2) stools per day (P >0.05). No significant difference in daytime soiling was present between IR (6 percent) and IPAA (4 percent). Nighttime spotting was also similar between the two groups. Nighttime soiling, however, was reported by 4 percent of IPAA patients but not by IR patients (P <0.05). One IPAA patient (1 percent) required pouch excision for a desmoid tumor, while two IR patients (11 percent) required proctectomy and ileostomy for recurrent dysplastic polyps (P <0.05). Adhesions and a shortened ileal mesentery prevented the construction of an ileoapal procedure in these latter patients. In conclusion, the postoperative complication rate and functional results are similar after IR and IPAA in patients with FAP; however, IR does not eradicate rectal polyps and may indeed preclude IPAA for those requiring subsequent proctectomy.
Similar content being viewed by others

References
Bussey HJR. Familial polyposis coli: family studies, histopathology, differential diagnosis and results of treatment. Baltimore: The Johns Hopkins University Press, 1975.
Gingold BS, Jagelman D, Turnbull RB. Surgical management of familial polyposis and Gardner's syndrome. Am J Surg 1979;137:54–6.
Bussey HJR, Eyers AA, Ritchie SM, Thomson JP. The rectum in adenomatous polyposis: the St. Mark's policy. Br J Surg 1985;72(suppl):S29–31.
Newton CR, Baker WNW. Comparison of bowel function after ileorectal anastomosis for ulcerative colitis and colonic polyposis. Gut 1975;16:785–91.
Sarre RG, Jagelman DG, Beck GJ,et al. Colectomy with ileorectal anastomosis for familial adenomatous polyposis: the risk of rectal cancer. Surgery 1987;101:20–6.
Bess MA, Adson MA, Elveback LR, Moertel CG. Rectal cancer following colectomy for polyposis. Arch Surg 1980;115;460–7.
Pemberton JH, Kelly KA, Beart RW Jr, Dozois RR, Wolff BG, Ilstrup DM. Ileal pouch-anal anastomosis for chronic ulcerative colitis: long-term results. Ann Surg 1987;206:504–13.
Dozois RR, Kelly KA, Welling DR,et al. Ileal pouch-anal anastomosis: comparison of results in familial adenomatous polyposis and chronic ulcerative colitis. Ann Surg 1989;210:268–73.
Pemberton JH, Phillips SF, Ready RR, Zinsmeister AR, Beahrs OH. Quality of life after Brooke ileostomy and ileal pouch-anal anastomosis: comparison of performance status. Ann Surg 1989;209:620–8.
Dozois RR, Berk T, Bulow S,et al. Surgical aspects of familial adenomatous polyposis. Int J Colorectal Dis 1988;3:1–16.
Slors JF, den Hartog Jager FCA, Trum JW, Taat CW, Brummelkamp WH. Long-term follow-up after colectomy and ileorectal anastomosis in familial adenomatous polyposis coli: is there still a place for the procedure? Hepatogastroenterology 1989;36:109–12.
Author information
Authors and Affiliations
Additional information
Read in part at the meeting of The American Society of Colon and Rectal Surgeons, St. Louis, Missouri, April 29 to May 4, 1990.
About this article
Cite this article
Ambroze, W.L., Dozois, R.R., Pemberton, J.H. et al. Familial adenomatous polyposis: Results following ileal pouch-anal anastomosis and ileorectostomy. Dis Colon Rectum 35, 12–15 (1992). https://doi.org/10.1007/BF02053332
Issue Date:
DOI: https://doi.org/10.1007/BF02053332