
Abstract
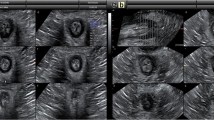
PURPOSE: A recent application of endosonography in the evaluation of anal sphincter morphology has led to controversy about the possibility of precisely assessing the diameter of external and internal anal sphincter muscles. On the other hand, magnetic resonance imaging (MRI) has been proposed to allow a more detailed view of the anatomy of the pelvic floor. However, both techniques have not yet been compared directly. METHODS: Eight healthy volunteers (age range, 25–40 years; 5∶3, male∶female) participated. Anal ultrasound was performed using a 7.5-MHz rectal transducer which produced a transversal panorama display of 360, allowing an image perpendicular to the anal canal. Imaging of the diameter of the internal and external anal sphincter muscles was performed with the transducer placed in the midanal canal, and measurement was always performed by the same investigator in dorsal projection. MRI was performed using a 1.5 Tesla Magnetom (Siemens, Erlangen, Germany) to obtain sagittal and angled axial (perpendicular to the anal canal) planes for consecutive 3-mm slices which were evaluated by four independent raters. RESULTS: Muscle thickness of the sphincter muscles in dorsal projection was 1.96±0.61 mm for the internal sphincter and 6.35±1.07 mm for the external sphincter using ultrasound. It was 1.72±0.13 mm and 3.99±0.99 mm, respectively, using MRI. When both measures were compared, only the internal sphincter data correlated significantly (r=0.818,P=0.0023) between both measures. Sagittal resonance imaging of the anal canal did not allow for differentiation of both muscles at all. Differentiation among mucosa, submucosa, and internal anal sphincter is not possible with MRI but may well be performed with high-resolution ultrasound. CONCLUSION: Anal ultrasound carries the potential of becoming a routine clinical procedure for evaluation of the anal anatomy and morphology in defecation disorders, but current MRI assessment of the anal anatomy is elaborate, costly, and does not provide any further insights.
Similar content being viewed by others


References
Rifkin D. Endosonography of the prostate: clinical applications. AJR 1987;148:1137–42.
Dragsted J, Gammelgaard J. Endoluminal ultrasonic scanning in the evaluation of rectal cancer. Gastrointest Radiol 1983;8:367–9.
Beynon J, Mortensen NJ, Channer JL, Rigby H. Rectal endosonography accurately predicts depth of penetration in rectal cancer. Int J Colorectal Dis 1992;7:4–7.
Goldman S, Norming U, Svensson C, Glimelius B. Transanorectal ultrasonography in the staging of anal epidermoid carcinoma. Int J Colorectal Dis 1991;6:152–7.
Law PJ, Bartram CI. Anal endosonography: technique and normal anatomy. Gastrointest Radiol 1989;14:349–53.
Pittmann JS, Benson TB, Sumners JE. Physiologic evaluation of the anorectum—a new ultrasound technique. Dis Colon Rectum 1990;33:476–8.
Gantke B, Enck P, Schäfer A, Lübke H. Morphology and function: sonographic, manometric and myographic evaluation of the anal sphincters. Dis Colon Rectum 1993;36:1037–41.
Burnett SJD, Bartram CI. Endosonographic variations in the normal internal anal sphincter. Int J Colorectal Dis 1991;6:2–4.
Law PJ, Kamm MA, Bartram CI. Anal endosonography in the investigation of faecal incontinence. Br J Surg 1991;78:312–4.
Schäfer A, Enck P, Wilhelm K, Gantke B, Lübke HJ, Strohmeyer G. Endosonography of the anal sphincters: incontinent and continent patients and healthy controls [abstract]. Gastroenterology 1993;104:A577.
Sultan AH, Kamm MA, Hudson CN, Bartram CI. Vaginal delivery causes sphincter disruption in 37 percent of patients (prospective ultrasound study) [abstract]. Gastroenterology 1992;102:A522.
Law PJ, Talbot RW, Bartram CI, Northover JM. Anal endonography in the evaluation of perianal sepsis and fistula in ano. Br J Surg 1989;76:752–5.
Eckardt VF, Nix W. The anal sphincter in patients with myotonic muscular dystrophy. Gastroenterology 1991;100:424–30.
Kamm MA, Hoyle CH, Burleigh DE,et al. Heditary internal anal sphincter myopathy causing proctalgia fugax and constipation. Gastroenterology 1991;100:805–10.
Kruyt RH, Delemarre JB, Doornbos J, Vogel HJ. Normal anorectum: dynamic MR imaging anatomy. Radiology 1991;179:159–63.
Aronson MP, Lee RA, Berquist TH. Anatomy of anal sphincters and related structures in continent women studied with magnetic resonance imaging. Obstet Gynecol 1990;76:846–51.
Mortensen N. Rectal and anal endosonography. Gut 1992;33:148–9.
Lestar B, Penninckx F, Rigauts H, Kerremans R. The internal anal sphincter can not close the anal canal completely. Int J Colorectal Dis 1992;7:159–61.
Law PJ, Kamm MA, Bartram CI. A comparison between electromyography and anal endosonography in mapping external anal sphincter defects. Dis Colon Rectum 1990;33:370–3.
Author information
Authors and Affiliations
Additional information
Supported by Grant En 50/10 from the Deutsche Forschungs-gemeinschaft.
Abstract published in Gastroenterology 1994;104:A577.
About this article
Cite this article
Schäfer, A., Enck, P., Fürst, G. et al. Anatomy of the anal sphincters. Dis Colon Rectum 37, 777–781 (1994). https://doi.org/10.1007/BF02050142
Issue Date:
DOI: https://doi.org/10.1007/BF02050142