
Summary
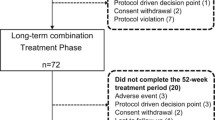
The purpose of this study, designed as an open multicenter trial, was to test the antihypertensive efficacy, patient acceptability, and side effects of long-term treatment with slow-release nifedipine in alarge population. The drug was studied in 330 outpatients with essential hypertension, WHO stage 1–2, recruited in 20 hospital centers. After washout period was completed, nifedipine (20 mg bid) was given for 1 month (phase 1). Then, the treatment was extended for 4 months (phase 2) with variable doses (rang 20–80 mg daily). No other antihypertensive drugs were administered during phase 1. However diuretics, beta blockers, or captorpril were added to nifedipine during phase 2 in 11 patients. Seventy patients did not meet ciiteria for inclusion at washout. During phase 1 and 2, 66 additional patients were excluded due to side effects, the need of other antihyperftnsive drugs, or noncomplicance. Systolic blood pressure significantly lowered (10% or more) in 84% patients in phase 1 and in 76% in phase 2. No responders were 6.1% and 3.6%, respectively. Diastolic blood pressure was normalized in 60% of patients after 5 months of therapy. Effects on blood pressure were equal in young patients and in the elderly, but a minimal rise in heart rate was recroded in younger patients.
At least one side effect occurred in 46.6% patients, mainly headeche (15.4%), hot flashes (13.3%), ankle edema (12.8%), or palpitation (6.6%). Sixteen patients (8.2%) were obliged to stop nifedipine treatment due to the severity of the side effects. This trial confirms the efficacy of nifedipine in hypertension, both in young and in aged patients. The adherence of patients to the twice-daily regimen was very good, without the development of tolerance in long-term treatment. The drug does not affect the physiologic cardiovacscuolar response to standing, but induces several relatively common, very seldom severe, adverse reactions.
Similar content being viewed by others


References
Hagino K. Application of ipoveratrial in the pharmacotherapy of hypertension.Jpn J Clin Exp Med 1968;45:208–213.
Zanchetti A. Perspectives in antihypertensive treatment. In: Zanchetti A, Krikler D edsCalcium antagonits in cardiovascular therapy. Amsterdam: Excerpta Medica, 1981:292.
Muiesan G, Agabiti rosei E, et al. Antihypertensive and homoral effects of verapamil and nifedipine in essential hypertension.J Cardiovasc Pharmacol 1982:4:S325.
Grun G, Fleckenstein A. Die elektromechanische entkopplung der glatten gesfassumskulatur als grundprinzip der coronardilatationdurch 4-(2-nitrophenyl)-2, 6-dimethyl-1,4-dihydropirindin-c arbosaure-dimethylester (Bay 1040, nifedipine).Arzneim-Forsch (Drug Reserach) 1972:22:334–343.
Robinson BF, Dobbs RJ, Kelsey CR. Effects of nifedipine on resistance vessels, arteries and veins in man.Br J Clin Pharmacol 1980:10:433–439.
Murakami M, Murakami E, Takekoshi N et al. Antihypertensive effect of nifedipine, a new coronary dilator.Jpn Heart J 1972;13:128–135.
Olivari MT, Bartorelli C, Polese A, et al. Treatment of hypertension with nifedipine, a calcium antagonist agent.Circulation 1979:59:1056–1060.
Taburet AM, Singlas E, Colin JN, et al. Pharmacokinetic studies on nifedipine tablet: Correlation with antihypertensive effects.Hypertension 1983;5(Suppl II):29
Murphy MB, Scriven AJI, Dollery CT, Role of nifedipine in the treatment of hypertension.Br Med J 1983:287:257–262.
Bonaduce D, Canonico, V, Mazza F et al. Evaluation of the efficacy of slow release nifedipine in systemic hypertension by ambulatory intraarterial blood pressure monitoring.J Cardiovasc Pharmacol 1985:7:145–151.
Menard J, Chatellier G, Degoulet P et al. How much can blood presure be lowered?Hypertension 1983:5(Suppl III):21.
Management Committee. The Australian Therapeutic trial in mild hypertension.Lancet 1980:1:1261–1267.
Leonetti G, Sala C, Bianchini C et al. Antihypertensive and renal effects of orally administered verapamil.Eur J Pharmacol 1980:18:375–382.
Henry PD. Calcium antagonist as cell protectant. In: Terroux P, Waters DD, edsProc 1 st Int Can Nifedipine Symp. Amsterdam: Exceepta Medica, 1983:196.
Nayler WG, Calcium antagonist.Eur Heart J 1980:1:225–238.
Schnapp P, Hermamm H, Cernak P, Kalay J. Nifedipine monotherapy in the hypertensive elderly: A placebocontrolled clinical trial.Curr Med res Opin 1986:10:407–413.
Erne P, Bolci P, Bertel O, et al. Factors influenceng the hypotension effect of calcium antagonists.Hypertension 1983:5(Suppl II):97–102.
Midtbo K. Efficacious and safe. In: Calcium antagonists—New perspectives. Oxford Medical Education Service, 1985:6.
Thibonnier M, Sassano P, Corvol P. Evaluation de l'effect antihypertenseur des formes capsule et comprimé de nifedipine dans l'hypertension.Arch Mal Coeur 1985:78:25–31.
Haynes RB, Sackett DL, Gibson ES et al. Improvement of medication compliane in uncontrolled hypertension.Lancet 1976:1:1265.
Opie LH, Jee LD, Nifedipine: Exanding indications in hypertension. in: Opie LH, ed.Calcium antagonistis and cardiovascular disease. New York: Raven Press 1984:333–342.
Hornung RS, Gould BA, Jones RI, et al. Nifedipine tablest for hypertension: A study using continous ambulatory intra-arterial recording.Am J Cardiol 1983:51:1323–1327.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Arrigo, F., Consolo, F. Long-term therapy with slow-release nifedipine in essential hypertension. Cardiovasc Drug Ther 4 (Suppl 5), 941–945 (1990). https://doi.org/10.1007/BF02018297
Issue Date:
DOI: https://doi.org/10.1007/BF02018297