
Abstract
Objective
An investigation into the incidence and the clinical implication of discrepancies which may sometimes occur between invasive and non-invasive hemodynamic evaluation in septic patients.
Design
A prospective, consecutive comparison.
Setting
Department of Intensive Care Medicine at a University Hospital.
Patients
32 patients undergoing therapy for an episode of septic shock.
Interventions
Conventional hemodynamic support (including volume expansion in all cases and inotropic support if necessary) required to obtain a stable hemodynamic status.
Measurement and results
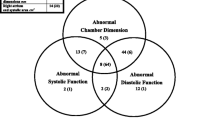
Cardiac output (thermodilution method), cardiac pressures (right heart catheterization) and left ventricular (LV) volumes (two-dimensional echocardiography) were simultaneously recorded. A comparison was thus made between both procedures, particularly concerning preload evaluation and assessment of left ventricular systolic function. Pulmonary artery occlusion pressure measurement was evidenced as an unreliable index of LV end-diastolic volume, determining preload. Assessment of LV systolic function by both methods was conflicting in 11 cases out of the 32.
Conclusions
Frequent discrepancies between to invasive and non-invasive procedure were observed. The reasons for these discrepancies, including low vascular resistance, reduced LV compliance, and a possible overestimation of cardiac output by the thermodilution method, are examined in the light of data recorded. It was concluded that invasive hemodynamic evaluation by right heart catheterization in septic patients should be seriously questioned.
Similar content being viewed by others

References
Ozier Y, Gueret P, Jardin F, Farcot Jc, Bourdarias JP; Margairaz A (1984) Two-dimensional echocardiographic demonstration of acute myocardial depression in septic shock. Crit Care Med 12:596–599
Teboul JL, Besbes M, Andrivet P, Axler O, Douguet D, Zelter M, Lemaire F, Brun-Buisson Ch (1992) A bedside index assessing the reliability of pulmonary artery occlusion pressure measurements during mechanical ventilation with positive end-expiratory pressure. J Crit Care 7:22–29
Triulzi M, Wilkins G, Gillam L, Gentile F, Weyman A (1985) Normal adult cross-sectional echocardiographic values: left ventricular volumes. Echocardiography 2:153–169
Lieppe W, Behar V, Scallion R, Kisslo J (1978) Detection of tricuspid regurgitation with two-dimensional echocardiography and peripheral vein injections. Circulation 57:128–132
Ross J, Braunwald E (1964) The study of left ventricular function in man by increasing resistance to ventricular ejection with angiotensin. Circulation 29:739–749
Jardin F, Brun-Ney D, Auvert B, Beauchet A, Bourdarias JP (1990) Sepsis-related cardiogenic shock. Crit Care Med 18:1055–1060
Bland M, Altman D (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 307–310
Winslow E, Loeb H, Rahimtoola S, Kamath S, Gunnar R (1973) Hemodynamic studies and results of therapy in 50 patients with bacteriemic shock. Am J Med 54:421–432
Weisel R, Vito L, Dennis R, Valeri R, Hechtman H (1977) Myocardial depression during sepsis. Am J Surg 133:512–560
Parker M, Shelhamer J, Barach S, Green M, Natanson C, Frederick T, Damske B, Parillo J (1984) Profound but reversible myocardial depression in patients with septic shock. Ann Intern Med 100: 483–490
Ellrodt G, Riedinger M, Kimchi A, Berman D, Maddahi J, Swan H, Murata G (1985) Left ventricular performance in septic shock: reversible segmental and global abnormalities. Am Heart J 110: 402–409
Schneider A, Teule J, Groeneveld A, Nauta J, Heidendal G, Thijs L (1988) Biventricular performance during volume loading in patients with early septic shock, with emphasis on the right ventricle: a combined hemodynamic and radionuclide study. Am Heart J 116:103–112
Jardin F, Sportiche M, Bazin M, Bourokba A, Margairaz A (1981) Dobutamine: a hemodynamic evaluation in human septic shock. Crit Care Med 9:329–332
Parker M, Shelhamer J, Natanson C, Alling D, Parillo J (1987) Serial cardiovascular variables in survivors and nonsurvivors of human septic shock: heart rate as an early predictor of prognosis. Crit Care Med 15:923–929
Bemis C, Serur J, Borkenhagen D, Sonnenblick E, Urschel C (1974) Influence of right ventricular filling pressure on left ventricular pressure and dimension. Circ Res 34:498–504
Parker M, McCarthy K, Ognibene F, Parillo J (1990) Right ventricular dysfunction and dilatation, similar to left ventricular changes, characterize the cardiac depression of septic shock in humans. Chest 97:126–131
Thys D, Hillel Z, Goldman M, Mindich B, Kaplan J (1987) A comparison of hemodynamic indices derived by invasive monitoring and two-dimensional echocardiography. Anesthesiology 67: 630–634
Wyatt H, Heng M, Meerbaum S, Gueret P, Hestenes J, Dula E, Corday E (1980) Cross-sectional echocardiography. II. Analysis of mathematic models for quantifying volume of the formaline-fixed ventricle. Circulation 61:1119–1125
Chaudry K, Ogawa S, Pauletto F (1978) Biplane measurement of left and right ventricular volume using wide angle cross-sectional echocardiography. Am J Cardiol 41:391–399
Erbel R, Schweitzer P, Lambertz H, Henn G, Meyer J, Krebs W, Effert S (1983) Echoventriculography: a simultaneous analysis of two-dimensional echography and cineventriculography. Circulation 67:205–215
Dodge H, Sandler H, Ballew D (1960) The use of biplane angiography for the measurement of left ventricular volume in man. Am Heart J 60:762–776
Ganz W, Swan H (1972) Measurement of blood flow by thermodilution. Am J Cardiol 29:241–246
Norris S, King G, Grace M, Weir B (1986) Thermodilution cardiac output — an in vitro model of low flow states. Crit Care Med 14:57–59
VanGrondelle A, Ditchey R, Groves B, Wagner W, Reeves J (1983) Thermodilution method overestimates low cardiac output in humans. Am J Physiol 245:H690-H692
Author information
Authors and Affiliations
Additional information
Supported in part by a grant of INSERM (CNEP no. 91CN30)
Rights and permissions
About this article
Cite this article
Jardin, F., Valtier, B., Beauchet, A. et al. Invasive monitoring combined with two-dimensional echocardiographic study in septic shock. Intensive Care Med 20, 550–554 (1994). https://doi.org/10.1007/BF01705720
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01705720