
Summary
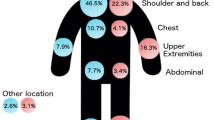
To assess the significance of spontaneous regression in superficial spreading melanoma (SSM), 36 patients with clinical signs of regression in their primary tumor were compared to 200 patients with regular SSMs (controls). SSMs with regression were found to have the following, distinctive clinical features, which were significantly different from controls (P<0.05):(1) male predominance (69%), (2) preferential localization on the trunk (80.6%), (3) lower tumor thickness (Breslow), (4) clustering in Clark levels II and III, and (5) a larger surface area. The incidence of metastases was lower in patients with regressing SSMs (13.9%) compared to controls (20.5%) although the time until relapse was slightly shorter (20.6 months versus 28.1 months for controls). These prognostic parameters were not significantly different. However, of the patients who died, 2 of 4 with zones of regression had thin melanomas (≦1.5 mm), compared to only 1 of 27 without regression zones (P<0.05). SSMs with regression therefore have unique clinical features, which may be related to their pathogenesis, and they may have some prognostic significance.
Similar content being viewed by others


References
McGovern VJ (1975) Spontaneous regression of melanoma. Pathology 7:91–99
Little JH (1972) Histology and prognosis in cutaneous malignant melanoma. In: Melanoma and skin cancer, Proc Int Cancer Conf Sydney, VCN Blight, Government Printer, pp 95–106
McLean DI, Lew RA, Sober AJ, Mihm MC Jr, Fitzpatrick TB (1979) On the prognostic importance of white depressed areas in the primary lesion of superficial spreading melanoma. Cancer 43:157–161
Trau H, Kopf AW, Rigel DS, Levine J, Rogers G, Levenstein M, Bart RS, Mintzis MM, Friedman RJ (1983) Regression in Malignant melanoma. J Am Acad Dermatol 8:363–368
Balch CM, Tariq MM, Soong S-J, Ingalls AL, Halpern NB, Maddox WA (1978) A multifactorial analysis of melanoma: Prognostic histopathological features comparing Clark's and Breslow's staging methods. Ann Surg 188:732–742
Gromet MA, Epstein WL, Blois MS (1978) The regressing thin malignant melanoma. A distinctive lesion with metastatic potential. Cancer 42:2282–2292
Paladugu RR, Yonemoto RH (1983) Biologic behavior of thin malignant melanomas with regressive changes. Arch Surg 118:41–44
McGovern VJ (1972) Growth patterns, multiplicity and regression. In: Melanoma and skin cancer. Proc Int Cancer Conf Sydney, VCN Blight, Government Printer, pp 95–106
Milton GW, Shaw HM, Farago GA, McCarthy WH (1980) Tumor thickness and the site and time of first recurrence in cutaneous malignant melanoma (stage I). Br J Surg 67:543–546
Trau H, Rigel DS, Harris MN, Kopf AW, Friedman RJ, Gumport SL, Bart RS, Grier WRN (1983) Metastases of thin melanomas. Cancer 51:553–556
Ariel IM (1982) Malignant melanoma of the trunk: A retrospective review of 1128 patients. Cancer 49:1070–1078
Chang P, Knapper WH (1982) Metastatic melanoma of unknown primary. Cancer 49:1106–1111
Lopez R, Holyoke ED, Moore RH, Karakousis CJ (1982) Malignant melanoma with unknown primary site. J Surg Oncol 19:151–154
Auerbach R, Auerbach W (1982) Regional differences in the growth of normal and neo-plastic cells. Science 215:127–134
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Czarnetzki, B.M., Denter, M., Bröcker, E.B. et al. Clinical features of superficial spreading melanomas with zones of regression. J Cancer Res Clin Oncol 107, 225–228 (1984). https://doi.org/10.1007/BF01032612
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01032612