
Summary
Purpose: The poor results from treatment of high grade glioma prompted us to explore new protocols involving concurrent radio-chemotherapy. Our primary objective was to evaluate the feasibility of very early postoperative chemotherapy with BCNU, concurrent radio-chemotherapy with carboplatin and teniposide, and post-radiotherapy BCNU. Our secondary objectives were to evaluate time to progression, and overall survival.
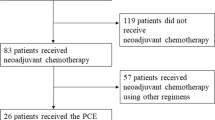
Patients and methods: We treated 24 newly diagnosed patients (pts) with BCNU 150 mg/m2 seven days after surgery. Thirty days later, we started radiotherapy, 1.8 to 2 Gy/day for 5 days a week on limited fields up to 60 Gy, and concurrent chemotherapy with carboplatin 250 mg/m2 on days 1, 22, and 43, and teniposide 50 mg/m2 on days 1, 2, 3, 22, 23, 24, 43, 44 and 45. Two cycles of 150 mg/m2 BCNU were then given at 30 and 70 days, respectively, after the end of the radio-chemotherapy course. Therapy was then suspended, but if disease progression was evident, treatment was resumed with drugs that had not been previously employed. Surgical reintervention was not routinely considered.
Results: Following radio-chemotherapy treatment in the 24 pts evauble for response, we observed partial remissions in 8 cases (33%) and stable disease in 12 (50%). Actuarial estimates of progression free survival (PFS) were 33 weeks, with 56 wks for anaplastic astrocytoma and 31 weeks for glioblastoma. Median survival time (MST) of all pts was 58 weeks; 51 weeks for glioblastoma and was not reached for anaplastic astrocytoma. This regimen was feasible. Of 144 planned cycles, 139 were delivered, and among these only in 13 and 9 cycles the doses were reduced by 75 and 50%, respectively. We did not observe any gastrointestinal toxicity. Grade 2 hematological toxicity occurred in 25% of pts, grade 3 in 4% and neurological toxicity in 3% of the pts during BCNU delivery, probably due to a sharp increase in intracranial pressure.
Conclusion: Early chemotherapy, concurrent chemo-radiotherapy and brief post-radio-therapy chemotherapy are feasible and well tolerated. The objective response and disease stabilization rates appear similar to previous experiences.
Similar content being viewed by others

References
Brandes A, Soesan M, Fiorentino M: Medical treatment in high grade malignant gliomas in adults: an overview. Anti cancer Research 11: 719–728, 1991
Levin VA, Silver P, Hannigan J et al.: Superiority of postradiotherapy adjuvant chemotherapy with CCNU, Procarbazine and Vincristine (PCV) over BCNU for anaplastic gliomas: NCOG 6G61 final report. Int J Radiat Oncology Biol Phys 18: 321–324, 1990
Shapiro JR, Mehta BP, Fiola M et al.: A minor sub population of cells in freshly resected malignant gliomas is BCNU-resistant, secretes PDGF-like peptides and becomes the dominant population after BCNU treatment. Abs Eight International Conference on Brain Tumor Research and Therapy, Lausanne, 530, 109, 1989
Vokes EE, Wechselbaum R: Concomitant chemoradiotherapy: rationale and clinical experience in patients with solid tumors. J Clin Oncol 8: 911–934, 1990
EORTC Brain Tumor Group: Cisplatin does not enhance the effect of radiation therapy in malignant gliomas. Eur J Cancer 21(5): 568–572, 1991
Yung WK, Mechtler L, Gleason MJ: Intravenous carboplatin for recurrent malignant glioma: a phase II study. J Clin Oncol 9: 860, 1991
Durand RE, Goldie JH: Interaction of etoposide and cisplatin in an in vitro tumor model. Cancer Treat Rep 71: 673–679, 1987
Spremulli E, Schulz JJ, Speckart VJ: Phase II study of VM-26 in adult malignancies. Cancer Treat Rep 64: 147, 1980
Jeremic B, Grujicic D, Jevremovic S: Carboplatin and etoposide chemotherapy regimen for recurrent malignant glioma: a phase II study. J Clin Oncol 10: 1074–1077, 1992
Burger PC: Malignant astrocytic neoplasms: classification, pathology, anatomy and response to treatment. Semin Oncol 13(1): 16–26, 1986
Macdonald DR, Cascino TL, Clifford S: Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol 8: 1277–1280, 1990
WHO Handbook for reporting results of cancer treatment. WHO offset publication N° 48 Neoplasma 20: 37–46, 1980
Kaplan EL, Meier P: Non parametric estimation for incomplete observation. J Am Stat Assoc 53: 457–481, 1958
Coughlin CT, Richmond RC: Biologic and clinical developments of cisplatin combined with radiation: concepts: utility, projections for new trials, and the emergence of carboplatin. Seminars in oncol 16: 31–43, 1989
Doz F, Berens M, Doughery D et al.: Comparison of the cytotoxic activities of cisplatin and carboplatin against glioma cell lines at pharmacologically relevant drug exposures. Journal of Neurooncology 11: 27–35, 1991
Walker RW, Cairncross JG, Posner JB: Cerebral herniation in patients receiving cisplatin. J of Neuro-Oncology 6: 61–65, 1988
Wallner KE, Galicich JH, Krol G et al.: Patterns of failure following treatment for glioblastoma multiforme and anaplastic astrocytoma. Int J Radial Oncol Biol Phys 16: 1405–1409, 1989
Hochberg FH, Pruitt A: Assumptions in the radiotherapy of glioblastoma. Neurology 30: 907–911, 1980
Bonadonna G, Robustelli della Cuna G: Manuele di Oncologia Medica. Masson, Milan 1991, pp 506–509
Walker MD, Eben A, Hunt WE et al.: Evaluation of BCNU and/or radiotherapy in the treatment of anaplastic gliomas. J Neurosurg 49: 333–343, 1978
Walker MD, Green SB, Byar DP et al.: Randomized comparisons of radiotherapy and nitrosoureas for the treatment of malignant glioma after surgery. New Engl J Med 303 (23): 1323–1329, 1980
Green SB, Byar DP, Walker MD et al.: Comparisons of carmustine, procarbazine, and high-dose methylprednisolone as additions to surgery and radiotherapy for the treatment of malignant glioma. Cancer Treat Rep 67(2): 121–132, 1983
Deutsch M, Green SB, Strike T et al.: Results of a randomized trial comparing BCNU plus radiotherapy, streptozotocin plus radiotherapy, BCNU plus hyperfractionated radiotherapy, and following misonidazole plus radiotherapy in the postoperative treatment of malignant glioma. Int J Radial Oncol Biol Phys 16: 1389–1396, 1989
Shapiro WR, Green SB, Burger PC et al.: Randomized trial of three chemotherapy regimens and two radiotherapy regimens in postoperative treatment of malignant glioma. J Neurosurg 71: 1–9, 1989
Shapiro WR, Green SB, Burger PC et al.: A randomized comparison of intra-arterial versus intravenous BCNU, with or without intravenous 5-fluorouracil, for newly diagnosed patients with malignant glioma. J Neurosurg 76: 772–781, 1992
Chang CH, Horton J, Schoenfeld D et al.: Comparison of postoperative radiotherapy and combined postoperative radiotherapy and chemotherapy in the multidisciplinary management of malignant glioma. Cancer 52: 997–1007, 1983
Levin VA, Wara WM, Davis RL et al.: Phase III comparison of BCNU and the combination of procarbazine, CCNU, and vincristine administered after radiotherapy with hydroxyurea for malignant gliomas. J Neurosurg 63: 218–223, 1985
Yung WKA, Janus TJ, Maor M et al.: Adjuvant chemotherapy with carmustine and cisplatin for pts with malignant gliomas. J Neuro-Oncol 12: 131–135, 1992
Cvitkovic FB, Haie-Meder C, Papadimitrakopoulou V et al.: Pilot study of 6 weeks of chemoradiotherapy with 5-FU and hydroxyuera in malignant glioma. J of Neuro-Oncol 15: 9–17, 1993
Lange OF, Haase KD, Scheef W: Simultaneous radio- and chemotherapy of inoperable brain tumors. Radiotherapy and Oncology 8: 309–314, 1987
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Brandes, A.A., Rigon, A., Zampieri, P. et al. Early chemotherapy and concurrent radio-chemotherapy in high grade glioma. J Neuro-Oncol 30, 247–255 (1996). https://doi.org/10.1007/BF00177276
Issue Date:
DOI: https://doi.org/10.1007/BF00177276