
Abstract
Introduction
This project aims to evaluate the ease and confidence of patients when using an iPad to complete an item prompt list (Patient Concerns Inventory) in a busy oncology outpatient clinic.
Patients and methods
100 consecutive patients attending routine maxillofacial oncology review clinic completed a study specific 5 item self-report questionnaire after completion of the PCI.
Results
Of eligible patients attending 14 clinics from March 2016 onwards, one-third (31) preferred to complete the PCI on an iPad with a volunteer in a separate room, while two-thirds (69) preferred to complete the PCI by themselves on an iPad in the waiting room. Previous use of an iPad and patient age (>70) were factors indicating lower confidence and a preference towards needing help in a separate room. Although the majority of patients were able to complete the PCI in the waiting room themselves there is a proportion who for a variety of reasons would prefer to have assistance.
Conclusion
This study helps to inform resource allocation (assistance and clinic area) when adopt the PCI across the whole oncology outpatient setting. Further research is needed to identify cost efficient ways to promote the self-completion of the PCI in those patients less confident.
Similar content being viewed by others


Introduction
Patients can experience considerable physical, functional, social and emotional problems after treatment for head and neck cancer [1]. It can be difficult for them to raise their concerns during clinical consultations. This might lead to unmet needs [2]. The Patient Concerns Inventory (PCI) was developed as an item prompt list [3,4,5]. Patients complete the tool whilst waiting for their consultation and any issues they identify can be discussed during the consultation.
Patient Concerns Inventory
Patients find the PCI helpful as it reminds them of things they otherwise might forget to mention to the clinician. Initially the PCI was completed on paper but as the PCI is also combined with a head and neck cancer quality of life questionnaire this made it difficult to include a summary in real-time for the doctor in clinic. A desktop computer was then tried, but patients found using a mouse problematic [6]. Head and neck cancer patients might be less familiar with computer technology as a proportion come from deprived backgrounds [7] or are elderly [8]. We upgraded to a ‘tablet’ and enlisted the support of a volunteer from the Volunteers Department to help patients to complete the PCI package. More recently we have been using an iPad; anecdotal evidence suggests that patients find the iPad much easier to use. iPad use is not novel [9, 10]; however, there is a paucity of studies reporting its use in head and neck cancer patients. Pollom [11] reported elderly patients found the technology more challenging. Patients over 70 years old may benefit from more assistance with electronic forms and should be allotted more time for completing tablet-based QOL surveys.
Item prompt list in routine clinic
Volunteer availability and side room accessibility for patients completing the PCI are limited, thus restricting wider adoption for all head and neck oncology patients. It would be advantageous if patients could use an iPad in the waiting room without the need for a volunteer.
Objective of the study
The aim of this audit was to evaluate how easy and confident patients felt about using an iPad to complete the PCI without assistance in a busy oncology outpatient review clinic setting.
Methods
Participants and procedure
Eligible patients were those at least 6 weeks post-treatment and disease free. The study was to run in consecutive clinics where the volunteer was available from 23rd March 2016 until 100 patients participated.
The tablet computer used for this study was the iPad™ (iPad is a trademark of Apple, Inc).
Measures
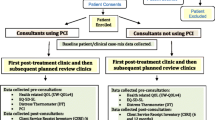
As is standard practice in the clinic eligible patients in the waiting room were invited to complete the PCI on an iPad. They were offered help from a volunteer in a separate room. Afterwards they were asked to complete a one page questionnaire about their use of the iPad and their future preferences for using an iPad to complete the PCI. The time it took to complete the PCI was recorded as were observations from the volunteers; such as whether the patient needed assistance and if so to what extent and for what reason (for example, an inability to see the iPad as the patient had forgotten their glasses). The survey was anonymised with only patient year of birth used to compute patient age.
The survey questionnaire asked five questions: previous iPad use (yes/no), how easy they found using an iPad (10 point scale), how easy they found completing the PCI (10 point scale), how confident did they felt completing the PCI on an iPad without help (10 point scale) and lastly their preference on completing the PCI with an iPad in the waiting room or with help from a volunteer in a separate room.
Analysis
Numerical analysis of recorded data was carried out on the questionnaire answers, patient age and time taken to complete PCI.
The data, which had been collected as part of a service audit rather than for research, and were approved by the local Audit Department.
Results
Participant characteristics
Eligible patients attending 14 clinics between 23 March 2016 and 24th August 2016 were invited to take part until a sample of 100 was obtained. Some eligible patients were not invited due to natural time constraints pertaining within busy clinics, but of those approached in the waiting room only 4 refused to participate. Median age of participants was 64 years with inter-quartile range (IQR) 58–71 years. Median time for completing the PCI by iPad was 10 min, IQR 6–15 min.
Problems completing PCI
One quarter (26) of patients were new to using the PCI. Two-thirds (65) had no problems completing the PCI, and from volunteer notes 14 patients had problems relating to eyesight or lack of glasses, 12 needed a little amount of help (reasons not stated), 6 had their PCI completed for them by daughters (3) or volunteers (2) or required a ‘lot of help’ (1), 1 was helped (extent not stated) by a daughter, 1 found it too noisy with the TV on in the background and 1 did not agree with the questions.
Confidence completing PCI
Three-quarters (75) had used an iPad before. For the three 10-point response questions (Table 1) there was a clear distinction between a minority of patients who indicated most difficulty using an iPad or in completing the PCI or in lacking confidence using an iPad to complete the PCI, and the majority of patients having little or no problems. One quarter (24) of patients were less confident of completing the PCI on an iPad without any help (scores 1–5) while three-quarters (76) were more confident (scores 6–10). One-third (31) preferred to complete the PCI on an iPad with a volunteer in a separate room, while two-thirds (69) preferred to complete the PCI by themselves on an iPad in the waiting room. Previous use of an iPad and patient age of 70 years and over were factors indicating lower confidence and a preference towards needing help in a separate room (Table 2). Whether a patient was new to the PCI at the time of recruitment was irrelevant to confidence and future preference. As expected, those who needed help to complete the PCI and those who took longer to complete it were less confident and more likely in future to require help, as were those who found it less easy to use an iPad or who found it less easy to complete the PCI.
All but one of the 17 patients who were ‘not at all confident’ (scored 1) about completing the PCI on an iPad without help, preferred to complete the PCI on an iPad with a volunteer in a separate room. These 16 patients were also all aged ≥70 years and before this study 13 of these 16 had no previous experience of using an iPad, while the 3 previous users were aged 82, 84 and 94 years. The one patient bucking this trend was aged 48, had used an iPad before and yet while not at all confident about completing the PCI alone did prefer to complete the PCI without help in the waiting room.
Discussion and conclusion
Discussion
Evidence of the completion of the Patient Concerns Inventory has been included as a component of the National Head and Neck Cancer Audit [12]. Although it has been used for many years in one clinic setting there is an imperative to increase patient access. The design of this study was within the context of an ‘audit’ rather than formal research, hence the amount of data collected was relatively limited. The consecutive patient sampling ensured that the patient feedback is representative of those attending the clinic. These patients reflect head and neck cancer patients attending the regional unit for review but the characteristics might be different in other geographical catchment areas where perhaps there is less deprivation or wider use of computer technology. While patients are generally very positive about using the PCI [13], several barriers need to be overcome to enable broader application of electronic completion in head and neck oncology outpatients clinic. Routinely used wider adoption is restricted by reliance of a volunteer and side room.
The findings demonstrate one quarter of patients were not confident to independently use the iPad for PCI completion. Although further research is needed to investigate reasons for this, it seems that this is mostly a generational influence with patients not brought up with computer technology being the least confident. Unfamiliarity with the iPad was identified as a barrier in a clinical setting using a breast health questionnaire application at a public hospital mammography clinic [14]. This work also highlighted the need for availability of instruction and assistance. Most women, especially new users, need brief instruction on how to use touchscreens and a person available for questions. Although using an iPAD might be ‘instinctive’ to those familiar with technology, a simple PCI tutorial video, voice instructions or ‘hints’ for each page could improve patient confidence.
Yaffe et al. [15] found that the addition of an iPad is an efficient and preferable questionnaire format to obtain patient-reported outcomes in a hand and upper extremity surgery practice setting. The iPad was particularly advantageous for longer questionnaires and for use in patients under the age of 50. Scott et al. go on to report no significant difference in patient responses when using paper forms of the PCI vs touch-screen technology [16].
Another aspect is that some patients seem to find it difficult to understand some of the words used in the PCI such as recreation, salivation, and intimacy. The audit is not a longitudinal assessment; however, repeated use of the current system seems unlikely to make a big difference in confidence. Several months can elapse between routine review appointments and patients often forget how they completed it in the past and sometimes even to the extent of forgetting that they have ever completed the PCI. Given the background of some of the patients it is inevitable that some will always prefer the assistance to complete the PCI. This is most likely for those that cannot read or always forget their glasses, again some of the more elderly ‘like it done for them’. It would be helpful to explore measures which could make the iPad easier for the less confident to complete the PCI.
Most patients are happy to complete the PCI in waiting room in particular are those who attend clinic by themselves i.e., do not have a partner/relative to discuss with. We had concerns that patients would want some confidentially away from other patients, but this seems not to be the case. Perhaps they like to sit in the waiting area so they can observe the flow of the clinic and make sure they don’t miss their turn. Only one patient has expressed he prefers to be taken into a room as he finds the noise, TV and general conversations, distracting. He completed without any assistance. A separate room is necessary for those patients who wish assistance to complete the PCI.
Conclusion
The use of tablet computers significantly aids the integration of HRQOL questionnaires and item prompt lists into routine clinical practice. How the technology is used will need to be tailored for individual patients, in particular the elderly and those not familiar with modern technology. The practical implications are that it is possible to identify certain patients who are willing and able to complete the iPad in the waiting area without involving the volunteer. This simple step will aid the wider use amongst patients and allow the time and space for volunteer support to be more focused to those at need.
References
Kanatas A, Ghazali N, Lowe D, Udberg M, Heseltine J, O’Mahony E, Rogers SN (2013) Issues patients would like to discuss at their review consultation: variation by early and late stage oral, oropharyngeal and laryngeal subsites. Eur Arch Otorhinolaryngol 270(3):1067–1074. doi:10.1007/s00405-012-2092-6 (Epub 2012 Jun 29)
Bidstrup PE, C Johansen, Mitchell AJ (2011) Screening for cancer-related distress: summary of evidence from tools to programmes. Acta Oncol 50:194–204
Brandes K, Butow PN, Tattersall MH, Clayton JM, Davidson PM, Young J, Epstein RM, Walczak A (2014) Advanced cancer patients’ and caregivers’ use of a Question Prompt List. Patient Educ Couns 97(1):30–37. doi:10.1016/j.pec.2014.06.010
Rogers SN, El-Sheikha J, Lowe D (2009) The development of a Patients Concerns Inventory (PCI) to help reveal patients concerns in the head and neck clinic. Oral Oncol 45:555–561
Miller N, Rogers SN (2016) A review of question prompt lists used in the oncology setting with comparison to the Patient Concerns Inventory. Eur J Cancer Care (Engl). doi:10.1111/ecc.12489 [Epub ahead of print]
Millsopp L, Frackleton S, Lowe D, Rogers SN (2006) A feasibility study of computer-assisted health-related quality of life data collection in patients with oral and oropharyngeal cancer. Int J Oral Maxillofac Surg 35(8):761–764
Rylands J, Lowe D, Rogers SN (2016) Influence of deprivation on health-related quality of life of patients with cancer of the head and neck in Merseyside and Cheshire. Br J Oral Maxillofac Surg 54(6):669–676. doi:10.1016/j.bjoms.2016.03.030
Rogers SN, Audisio RA, Lowe D (2015) Do the elderly raise different issues when using the Patient Concerns Inventory in routine head and neck cancer follow-up clinics? Eur J Cancer Care (Engl) 24(2):189–197. doi:10.1111/ecc.12289 (Epub 2015 Feb 4)
Schick-Makaroff K, Molzahn A (2014) Brief communication: patient satisfaction with the use of tablet computers: a pilot study in two outpatient home dialysis clinics. Can J Kidney Health Dis. 1:22. doi:10.1186/s40697-014-0022-9 (eCollection 2014)
Pierce L, Hocking MC, Schwartz LA, Alderfer MA, Kazak AE, Barakat LP (2016) Caregiver distress and patient health-related quality of life: psychosocial screening during pediatric cancer treatment. Psycho Oncol. doi:10.1002/pon.4171 [Epub ahead of print]
Pollom EL, Wang E, Bui TT, Ognibene G, von Eyben R, Divi V, Sunwoo J, Kaplan M, Dimitri Colevas A, Le QT, Hara WY (2015) A prospective study of electronic quality of life assessment using tablet devices during and after treatment of head and neck cancers. Oral Oncol 51(12):1132–1137. doi:10.1016/j.oraloncology.2015.10.003 (Epub 2015 Oct 23)
National Head and Neck Cancer Audit 2014. http://content.digital.nhs.uk/catalogue/PUB18081/clin-audi-supp-prog-head-neck-dahn-13-14.pdf. Accessed 21 Sep 2016
Rogers SN, Lowe D (2014) An evaluation of the head and neck cancer patient concerns inventory across the Merseyside and Cheshire Network. Br J Oral Maxillofac Surg 52:615–623. doi:10.1016/j.bjoms.2014.04.011
Bravo C, O’Donoghue C, Kaplan CP, Luce J, Ozanne E (2014) Can mHealth improve risk assessment in underserved populations? Acceptability of a breast health questionnaire app in ethnically diverse, older, low-income women. J Health Dispar Res Pract 7(4):1–19
Yaffe M, Goyal N, Kokmeyer D, Merrell GA (2015) The use of an iPad to collect patient-reported functional outcome measures in hand surgery. Hand (N Y) 10(3):522–528. doi:10.1007/s11552-014-9731-x
Scott B, Ghazali N, Lowe D, Bekiroglu F, Rogers SN (2013) The Patients Concerns Inventory in head and neck cancer: comparison between self-completed paper and touch screen versions in the clinic setting. Eur J Oncol Nurs 17(6):863–869. doi:10.1016/j.ejon.2013.05.002 (Epub 2013 May 31)
Acknowledgements
The authors would like to thank Ruth Sturgeon, Volunteers Department, for her support in clinic with regards completion of the PCI. We also thank the IT Department at Aintree University Hospital for writing the programme making it wifi available in the clinical areas.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We have no conflicts of interest.
Ethics statement/confirmation of patient’s permission
The data, which had been collected as part of a service audit rather than for research, met the criteria of the local Clinical Governance Department for service evaluation.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Rogers, S.N., Pearson, T. & Lowe, D. How easy and confident do patients feel about using an iPad to complete the Patient Concerns Inventory without assistance in a busy head and neck oncology outpatient review clinic. Oral Cancer 1, 1–5 (2017). https://doi.org/10.1007/s41548-017-0001-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41548-017-0001-9