
Abstract
Athletes are increasingly required to travel domestically and internationally, often resulting in travel fatigue and jet lag. Despite considerable agreement that travel fatigue and jet lag can be a real and impactful issue for athletes regarding performance and risk of illness and injury, evidence on optimal assessment and management is lacking. Therefore 26 researchers and/or clinicians with knowledge in travel fatigue, jet lag and sleep in the sports setting, formed an expert panel to formalise a review and consensus document. This manuscript includes definitions of terminology commonly used in the field of circadian physiology, outlines basic information on the human circadian system and how it is affected by time-givers, discusses the causes and consequences of travel fatigue and jet lag, and provides consensus on recommendations for managing travel fatigue and jet lag in athletes. The lack of evidence restricts the strength of recommendations that are possible but the consensus group identified the fundamental principles and interventions to consider for both the assessment and management of travel fatigue and jet lag. These are summarised in travel toolboxes including strategies for pre-flight, during flight and post-flight. The consensus group also outlined specific steps to advance theory and practice in these areas.
Similar content being viewed by others

Travelling athletes experience travel fatigue and jet lag that intensify their subjective burden and may influence performance and increase illness and injury risk. |
Literature on management of travel fatigue and jet lag in athletes is limited. Based on physiological principles and laboratory-based studies, this review and consensus identified the most important interventions to counter. |
Travel fatigue: maximise the amount of sleep obtained during travel. |
Jet lag: maximise the rate at which the body clock adapts to the new time-zone, by following a guide that specifies 3h periods of light exposure and avoidance. |
Other useful interventions include: |
Travel fatigue: plan meticulously, prevent illness, formulate hydration and food strategies. |
Jet lag: preserve sleep, coincide exercise training with light exposure, adjust meal timing and composition, and sensible use of melatonin at the new destination. |
Manipulating exposure to time-givers, e.g. light and exogenous melatonin, may aid in successful circadian re-alignment following travel in athletes. Conversely, inappropriate exposure may be counterproductive and cause detrimental side effects. |
Reliable and repeatable multi-centre field studies, over longer durations and involving randomised allocation of potential therapeutic interventions are needed to advance theory and practice in these areas. |
1 Introduction
The modern-day athlete is often required to travel domestically and internationally including high-frequency short distances (< 3 h) and low-frequency long distances (> 3 h) that may involve the crossing of numerous time zones. The subsequent travel fatigue and jet lag experienced result in a myriad of shared symptoms, such as daytime fatigue, decreased concentration and alertness, sleep disruption and gastrointestinal disturbances [1, 2]. These can lead to increased illness and injury risk as well as adverse effects on athletic performance [2,3,4,5,6,7,8,9].
Travel fatigue and jet lag are two distinct entities that may co-occur when travelling east or west across three or more time zones [2, 4, 10,11,12]. Travel fatigue occurs in all travelling athletes and can be acute following any individual long journey, or chronic (cumulative) as a consequence of repetitive travel within a season [4, 10]. It is a multi-domain disturbance that generally occurs with any travel regardless of the direction of travel or the number of time-zones crossed [2, 4, 10, 13]. It is caused by the demands of travel itself, such as cramped conditions, prolonged mild hypoxia, changes in the external environment (trans-latitudinal travel i.e. winter–summer/summer–winter) and reduced physical activity [10]. Jet lag is episodic with similar but more severe and prolonged symptoms compared to travel fatigue and follows rapid travel across 3 or more time-zones (transmeridian travel i.e. east–west/west–east) [4, 10]. It is typically characterised by the desynchronisation between the internal human circadian system and the time at the new destination [2, 4, 10, 11, 14]. As a result, the circadian rhythm of several psychological, physiological and behavioural variables with a typical early morning nadir and late-afternoon peak is misaligned with the new local time. Depending on the training or competition time, this could directly affect athletic performance [2, 4, 5].
Although the circadian system is well understood and described in the circadian physiology literature [5, 15,16,17,18,19], it remains difficult to translate and to apply this knowledge to travel management practice within sport. Research in this area is complex due to factors, such as inter-individual differences and the challenge of measuring the circadian phase in field studies, using markers, such as core body temperature (CBT) and melatonin. A recent systematic review on the management of travel fatigue and jet lag in athletes concluded that no evidence exists for specific travel fatigue interventions and that evidence for interventions targeting jet lag is of low quality [20].
Since evidence-based data underpinning travel fatigue and jet lag management are under-developed [3, 21], an expert panel was formed to define criteria from existing recommendations [22, 23], and to inform sport science and medicine practitioners and sport programme managers on current consensus-based recommendations from a practice-led perspective [24]. This paper aims to define the terminology commonly used in the field of circadian physiology; provide basic information on the human circadian system and how it is affected by time-givers (zeitgebers); discuss the causes and consequences of travel fatigue and jet lag; and provide consensus recommendations on managing travel fatigue and jet lag in athletes.
2 Methods
Our methodology is based on a recent publication, recommending specific criteria to reach consensus [23]. A lead group of three authors (CJvR, AJvR, PF) initially discussed the writing of a consensus document. A further 23 experienced researchers and clinical practitioners in the fields of travel fatigue, jet lag and sleep in the sports setting were invited to participate on the expert panel to formalise a consensus document and recommendations. The average experience of the authors in this field ranged from 4 to 25 years. The group consisted of 14 males and 12 females and embodied global representation from 11 different countries. Their expertise included 18 scientists (including sleep and circadian physiologists, sport scientists, a nutritionist and a statistician) and 8 medical team practitioners (medical doctors and physical therapists). The authors conducted comprehensive literature searches in PubMed, MEDLINE, CINAHL, Google Scholar, and SPORTDiscus to obtain relevant peer-reviewed publications regarding the human circadian system and the management of travel fatigue and/or jet lag. Two authors (CJvR, AJvR) compiled the first draft and sent it for initial comments by the full author group. The reviewed draft consisted of sections on terminology, the circadian system, travel fatigue and jet lag. According to preference, the authors chose primary working clusters from the four sections. Eight total Qualtrics surveys were sent for those sections where recommendations are provided, i.e. list of terminology (3), management options for travel fatigue (2) and management options for jet lag (3). A statistician (TC) analysed all feedback collected in the 8 surveys. To govern the threshold of agreement, only the statistician had access to the feedback provided by the authors.
The terminology group (AB, ID, TC) listed terms included in this consensus document that are commonly used to describe the human circadian system. The group provided three definitions for each term and administered a Qualtrics survey to systematically combine expert opinions and arrive at an informed group consensus on the selected terms. After the first round, a threshold of 80% agreement [23] was reached on the definitions of the following terms: biological night, chronobiotic, chronotype, circadian rhythm, jet lag, phase shift, phase response curve, re-entrainment, and suprachiasmatic nucleus. For the next round, the rest of the terms were included: body clock, core body temperature minimum (CBTmin), dim light melatonin onset (DLMO), internal desynchrony, melatonin, nadir, phase, process C, process S, retino-hypothalamic pathway, sedative (hypnotic), and zeitgebers (time-givers). For these terms, definitions with the least votes were excluded and the remaining two definitions were adapted according to comments suggested by the authors. In the 3rd round, the senior author group (CJvR, AJvR, PF) based consensus on the majority vote since authors could not agree on phrasing the definition of terms. Further comments from all authors were applied to reach the final definition for each term.
The circadian system group (DS, MD) summarised and documented relevant literature on the physiological, psychological and behavioural variables of the human circadian system. They focussed on the relevance to translate theory into practice.
The travel fatigue group (KoS, ACS, JV, KM, MB, ML, MN, SH) summarised current literature regarding the causes and consequences of travel fatigue. This group also listed potential management options based on available literature including current opinions, expert recommendations and research-based studies (laboratory and field) on the management of travel fatigue. All authors voted on the inclusion or exclusion of each management option. Consensus was reached after the 2nd Qualtrics survey. A threshold of 80% agreement [23] was used to indicate a consensus among the authors. The average response rate by the author group to reach consensus was 96.2%.
The jet lag group (HF, ACS, CS, GV, GR, JMA, LG, MS, MDo, RC, TP) summarised current literature regarding the causes and consequences of jet lag. This group listed potential management options based on available literature including current opinions, expert recommendations as well as research-based studies (laboratory and field) on the management of jet lag. All authors voted on the inclusion or exclusion of each management option using a Qualtrics survey. After three rounds of Qualtrics surveys, consensus was reached. A threshold of 75% agreement [23] to each survey was used to indicate consensus among the authors. The average response rate by the author group to reach consensus was 92.3%.
Each sub-group within the consensus group provided sections on their relevant topics to form a second draft. The lead group (CJvR, AJvR, PF) reviewed and collated the different sections into a third draft. The author group collectively revised this third draft. Extensive discussions by all members of the consensus group followed, and all authors provided comments and suggestions. The lead group accepted or declined all responses within reason and sent the 4th draft for another round of input from the author group. Subsequently, all authors of the consensus group reviewed and approved the final manuscript.
3 Terminology
Terminology in the field of circadian physiology is complex. The following detailed explanations in Table 1 were developed by consensus and is an overview of specific terms and phrases commonly used when (a) referring to the human circadian system, or (b) when practitioners are contributing to travel planning and intervention design.
Although well described in the literature of circadian physiology, the information on the human circadian system is very detailed and beyond the scope of time-poor practitioners. The section below provides relevant information to aid practitioners to translate and apply circadian physiology into practical travel management.
4 Circadian System
The circadian system regulates the diurnal cyclical rhythms exhibited by physiological, psychological, and behavioural processes of the body over approximately 24 h [35, 36]. This system is regulated by a central “master clock”, the suprachiasmatic nucleus (SCN), as well as peripheral clocks located in almost every cell of the body [16,17,18]. These are synchronised by a sophisticated system of neuronal, hormonal and autonomous signalling [13]. Output signals from the clocks are subsequently generated, influencing physiological, psychological and behavioural processes [15]. The master and peripheral clocks of the circadian system synchronise through zeitgebers or time-givers [37].
4.1 Time-Givers/Zeitgebers
Common time-givers are light, sleep–wake transition, physical activity, social cues and meals [38, 39]. Light is arguably the most critical time-giver, as photic stimuli, via the retino-hypothalamic pathway, stimulates or inhibits the SCN [13, 15, 16, 18]. The timing, intensity, duration and spectral composition of light appear to be the most critical factors in altering the timing of the circadian system [13, 27] (Fig. 1).

Schematic diagram of the circadian clock entrainment pathways. Light directly entrains the suprachiasmatic nucleus (SCN), whereas other non-photic zeitgebers exhibit rhythmic changes and entrain the SCN and peripheral clocks throughout 24 h—adapted with permission from Buttgereit et al. [40] and Hood and Amir [41]
4.2 Phase Markers
Key players in successful circadian re-alignment are the phase markers melatonin and CBTmin. Melatonin is a hormone secreted by the pineal gland that aids in the process to consolidate sleep. The onset of secretion under dim light conditions, termed dim light melatonin onset (DLMO), occurs ~ 2 h before habitual bedtime and aligns with the start of the biological night [15,16,17,18]. The circadian rhythm of CBT oscillates ~ 0.8–1.0 °C between a night-time minimum and a daytime maximum in a rhythmic 24-h pattern [42, 43], with CBTmin typically occurring between 03:00 and 07:00 [44, 45].
4.3 Sleep Regulation
When CBT is at its lowest or is falling rapidly, it is easier to initiate sleep, whereas it is difficult to sleep when CBT is high or rising rapidly [2, 46]. Internal physiological changes that occur due to the circadian system also play an important role in initiating sleep. As sleep homeostasis/sleep pressure commonly referred to as Process S, accumulates with increasing waking hours of sleep, circadian-induced secretion of melatonin along with reductions in CBT and blood pressure, known as Process C allows a person to sleep [32]. Misalignment between these processes often leads to sleep disruption, including difficulty initiating and/or maintaining sleep [32].
4.4 Phase-Shift
Exposure to a time-giver induces a wave response and can shift the circadian system (phase-advance or phase-delay). The strength of the shift is often described using a phase response curve (PRC). Light exposure during the 0–6 h period on either side of the CBTmin is effective but 0–3 h results in maximum phase shifts [47,48,49]. Although the dose–response relationship is non-linear, the wavelength (shorter blue light, 400–495 nm) and intensity of bright light (≥ 2500 lx) [50, 51], and the duration of exposure (longer) will determine the degree to which the timing of the circadian system can be shifted [52,53,54]. The pattern of endogenous melatonin secretion is inversely related to body temperature—peak melatonin secretion occurs at the nadir of CBT (Fig. 2) [55]. Manipulating exposure to time-givers (Fig. 1) may aid in successful circadian re-alignment mitigating the effects of jet lag. Conversely, inappropriate exposure may be counter-productive and cause detrimental side effects. An example of this is evidenced by the impact of irregular exposure to bright light leading to cognitive deficits and mood alterations [56].

Normal profile of endogenous melatonin (red line) and schematic human phase response curves to light (dark blue line) and exogenous melatonin (light blue line). The y-axis on the right shows the endogenous melatonin concentration. The y-axis on the left shows the direction and relative magnitude of the phase shift following light exposure or exogenous melatonin administration at various times as presented on the x-axis. The magnitude of phase shifts will depend on the dosage used and should not be directly compared—adapted with permission from Eastman and Burgess [5] and Burgess et al. [57]
4.5 Individual Differences
Re-entrainment following a time-zone change is believed to also depend on an individual’s chronotype [13, 19, 58]. Hypothetically, the population consists of 3 chronotypes: morning-type- (18–30%), intermediate-type- (50–60%) and evening-type individuals (18–20%) [19, 59]. Currently, evidence to support links between chronotype and jet lag symptoms is based on social jet lag and shift worker studies [60,61,62,63]. To assist practitioners in understanding their travelling athlete, and help individualise scheduled intervention (e.g. light therapy), please refer to the advice presented online in Electronic Supplementary Material Table S1: morning-type subjects vs. evening-type subjects [2, 13, 19, 58,59,60,61,62,63,64,65,66,67,68,69]. Additionally, genetic differences regarding re-entrainment are of potential interest. Specifically, within the Period (PER) gene family, the PER34 allele is associated with extreme evening-type, whereas the PER35 allele is associated with extreme morning-type [69].
5 The Concept and Relationship Between Travel Fatigue and Jet Lag
Travel fatigue is a multi-domain disturbance that can be either acute or cumulative due to repetitive travel over a season, regardless of the mode of transport (road, rail, plane), the travel direction or the number of time zones crossed [2, 4, 10, 13]. Jet lag follows any journey rapidly crossing three or more time-zones, is episodic and implies full recovery after resynchronisation [2, 4, 10,11,12]. The relationship between travel fatigue and jet lag is conceptualised in (Fig. 3) and further discussed in Sects. 6 and 7.

A proposed multifactorial model of travel fatigue and jet lag—adapted with permission from Samuels [4]. Travel fatigue (on the left) is influenced by both internal and external factors. Allowing a recovery window taking into account travel distance, travel time, travel frequency and the length of the season combined with monitoring and appropriate management will lead to the ideal outcome. Jet lag (on the right) is also influenced by external factors and less so by internal factors. Travel direction and travel distance, specifically the number of time zones crossed will affect the severity experienced by the individual. Recovery to achieve the ideal outcome relies on resynchronisation of the body clock
6 Travel Fatigue
6.1 Causes and Consequences
Travel fatigue refers to exhaustion and tiredness associated with any long journey [4, 70, 71] following trans-latitudinal travel (north–south/south–north) or transmeridian travel. It is a complex summation of physical, physiological and psychological factors that accrue during an individual trip [4, 9], and could accumulate over a competition season. At present, there is substantial anecdotal evidence of its prevalence [4, 9, 61, 72,73,74]. There is however a lack of empirical evidence of the mechanisms underpinning travel fatigue, and how it might be prevented or its impact lessened [20]. Some commonly perceived contributors to travel fatigue are highlighted in Fig. 3 and Table 2.
When discussing the burden of travel fatigue on athletes, there are four key factors to consider: the total distance travelled, the time of travel (am or pm), the frequency of travel, and the length of the season. This concept is also referred to as the “recovery window” and indicates the available time for recovery (Fig. 3). The first three factors are well-documented in some professional sports [83, 86, 87]. For example, the National Basketball Association’s (NBA) regular season continues over 6 months consisting of 41 home games and 41 away games often inclusive of back-to-back games [87]. Congested schedules often include large travel distances as experienced by teams within the 4 top professional leagues [i.e. the National Hockey League (NHL), Major League Baseball (MLB), National Football League (NFL), and the NBA] in the United States entailing travel between 40,000 km (once around the world) and 80,000 km (twice around the world) per season [88].
There is limited evidence on the potential consequences of travel fatigue. Studies have assessed the acute effects of air travel without crossing time zones on performance and perceptual measures among team sports players [6,7,8,9]. Overall, under these circumstances, travel has no noticeable effect on indicators of performance (i.e. technical and tactical performance during competition; countermovement jump performance; Yo-Yo intermittent recovery test performance), but negatively influences perceptual measures (e.g. reduced alertness, motivation and mood, increased perceived stress and fatigue) [4, 6,7,8,9].
6.2 Assessment of Teams and Athletes
Athlete monitoring tools may help to understand both acute and chronic travel fatigue in athletes. In this respect, the creation and validation of a travel fatigue scale would improve understanding of the travelling effect [72] and should target measurement of the main symptoms of travel fatigue, namely persistent fatigue, recurrent illness, behaviour and mood changes and loss of motivation. An ideal tool should detect a significant part of travel fatigue including travel, sport, personal, social and seasonal factors and also provide scores for both individual trips and accumulative travel fatigue over a season (repeated measures design). Additionally, the coefficient of variation between different assessments of the same athlete should be small in comparison with the difference between athletes. Finally, its levels should not vary significantly in the same athletes under the same conditions at different times. As this is a highly individualised measurement, it should be used primarily to detect intra-individual changes. Travel fatigue is multifactorial and presently no single marker quantifies all these requirements. Surrogate markers for travel fatigue must include subjective ratings of sleep quality, stress/mood, fatigue, and recovery [89]. Current recommended tools include the Total Quality of Recovery Scale [90] to measure psychophysiological recovery (i.e. mood states and body signals, such as sensations of soreness or heaviness), the Daily Analysis of Life Demands for Athletes Questionnaire and the Acute Recovery Stress Scale [91], which are also practical and intelligible measures that can be used to monitor general changes in fatigue and recovery states [92]. Athletes must be thoroughly familiarised with these perceptual rating scales in order to benefit. Notably, travel fatigue-specific assessments would only be used in a scenario where jet lag is not a problem (e.g. teams competing in the UEFA European Football Championship), as there is shared symptomatology and it is difficult to separate out the fatigue caused by the travel itself. It is also important to take into account that too many different psychometric tools will add to the daily burden on athletes and may lead to superficial feedback.
6.3 Current Recommendations in the Management of Travel Fatigue
A recent systematic review reported that no research exists on interventions that specifically manage travel fatigue in athletes [20] with available studies limited to opinions and collective experience rather than original research [93]. While travel distance or duration may be the key factor in the magnitude of travel fatigue experienced, having an adequate period to recover from travel (e.g. a recovery window) to prepare for training or competition is critical [4] and should be accounted for in travel arrangements. This may be unfeasible for athletes that travel frequently. Hence, they may need to implement interventions before and during travel to reduce fatigue (e.g. protecting sleep) or to treat fatigue post-travel (e.g. utilising napping and caffeine) [4, 94]. Following consensus, the information discussed in Table 3 was determined valuable for the management of travel fatigue.
7 Jet Lag
7.1 Causes and Consequences
7.1.1 Causes
The concept of “time-zone differential” relies on the function of distance travelled, i.e. travel duration and number of time-zones crossed as well as the travel direction. It is a circadian phenomenon specifically relating to jet lag [4] (Fig. 3). After rapid transmeridian travel (air travel across 3 or more time-zones) or trans-latitudinal travel including crossing of three or more time zones, the circadian system cannot immediately adjust to the light–dark cycle in the new time zone. This causes internal desynchrony, between both the master and peripheral clocks [2], as well as with sleep homeostasis [5, 104]. As a result, the circadian system remains aligned, at least initially, with the timing of the light–dark cycle in the departure time zone rather than the arrival time zone [105]. The circadian system must be re-entrained, whereby the internal clocks resynchronise with external time-givers (Fig. 2) [17, 18], over several days [2]. As a rule of thumb, the duration of natural alignment is 0.5 days per time-zone crossed in a westerly direction, i.e. 2 h per day, and 1 day per time zone crossed in an easterly direction, i.e. 1 h per day [5, 57]. Until re-entrainment is complete, the physiological and psychological systems that are regulated by the circadian system (e.g. digestion, sleep, or mood) will remain misaligned with the new local time, and depending on time of training or competition, this may impact performance [2, 5, 9, 21].
7.1.2 Consequences
The most common symptoms of jet lag are gastrointestinal discomfort, daytime fatigue/sleepiness, impaired mental or physical performance and poor sleep [71, 106]. The intensity and duration of jet lag symptoms worsen with an increasing number of time zones crossed, i.e. crossing 3–4 time zones produces milder symptoms compared to crossing 10–12 time zones [106]. The experience of jet lag is also greatly influenced by the direction of travel [5]. For example, after a westward flight over 8 time zones, athletes will feel sleepy, their performance will be impaired in the evening, and they will wake earlier than usual in the morning [21]. In contrast, after an eastward flight over 8 time zones, athletes will also feel sleepy, but their performance will be impaired in the early afternoon, they will have difficulty falling asleep at their regular bedtime, and they will sleep in later than usual [21]. Chronotype may also influence these responses as morning larks adapt better to eastward travel (easier to shift circadian rhythms earlier), whereas night owls adapt better to westward travel (easier to shift circadian rhythms later) [62].
7.2 Assessment of Teams and Athletes
Given the complexity of the disruption to the circadian system, as well as the variety of associated physiological and psychological symptoms, several assessment tools can be used to assess the different aspects of jet lag. These may include questionnaires, sleep diaries in conjunction with actigraphy and circadian-phase markers.
Of the available questionnaires, the Liverpool Jet Lag Questionnaire appears to be the most valid and reliable subjective tool [74, 107]. This questionnaire is a visual analogue scale with 15 subjective ratings about overall perceived jet lag and its symptoms (sleep, fatigue, appetite, mental performance and bowel function), measured at different times of the day. Other tools such as the Columbian Jet Lag Scale [108] may offer suitable alternatives [109].
Actigraphy typically utilises movement-derived algorithms to provide estimates of sleep timing, duration and quality, and is commonly used in athletic settings in conjunction with sleep diaries [110, 111]. While actigraphy can help with information regarding rest–activity and/or sleep behaviour during travel, there is minimal evidence to support its use in evaluating jet lag per se. Circadian-phase markers perhaps represent the most accurate objective measure to assess jet lag, as they examine a phase response to interventions (e.g. CBT, salivary melatonin,[48, 112] body skin temperature) [13, 113, 114] but are unlikely suitable for sport due to the practicality, cost and invasiveness. If feasible, these circadian-phase markers could give insight into designing optimal jet lag interventions. A technique to indicate if sleep–wake behaviour has adapted is to measure the change in the mid-point of the sleep period between home and destination time zone, i.e. the difference in the median hours between bedtime and get-up time as assessed by actigraphy [60, 115]. The authors suggest this as a possible alternative to measuring CBT and salivary melatonin-phase markers.
There are several online jet lag calculators and mobile applications which provide advice on the timing of interventions to theoretically help adjust to a new time-zone [116,117,118]. In the elite sport environment, these calculators and mobile applications still require validation of the scientific base used to provide this advice, i.e. how is circadian phase determined, and are the proposed interventions evidence-based [119]. The consensus group cautions against the use of these until further research examining the efficacy and effectiveness of these tools in the athlete environment has been conducted.
Choosing measures to assess jet lag depends on a range of factors, such as the intention of the measure, validity and reliability, suitability for laboratory or field testing, as well as cost, time, practicality and expertise of operation. Teams or athletes are best served to select a tool that serves their direct purpose. Further research is needed to determine appropriate assessment measures of jet lag for teams and athletes [20, 120].
7.3 Current Recommendations in the Management of Jet Lag
Most literature refers to light, melatonin and preservation of sleep as the best options to mitigate jet lag. Considering the impact of sleep loss on performance, one of the main goals taking into account the athlete’s training and competition schedules, should be to preserve sleep. Other strategies include exercise, nutrition, melatonin analogues, sedatives and stimulants. The literature regarding recommendations on management strategies is published mainly as opinions [4, 13, 93, 106], collective experience manuscripts [3, 5, 21, 121], laboratory research studies on how to induce a phase shift [122,123,124,125] and laboratory research studies on how to recover from a phase shift [20, 48, 49]. Considering the literature referenced in this consensus paper, extrapolating evidence from healthy community and military populations and following the findings of a recent systematic review [20], the author group collectively summarised current recommendations based on consensus (Table 4, Figs. 4, 5 and 6).


Recommended interventions to help prevent or reduce the effect of jet lag

Combined interventions and short-term travel recommendations to help prevent or reduce the effect of jet lag

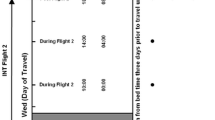
The combined use of light (exposure or avoidance), exogenous melatonin ingestion and administration of short-acting hypnotics to facilitate adaptation to phase shifts from the day of arrival. a Depicts westward travel with the first row illustrating normal home time. The next three rows illustrate travel crossing 4, 8 and 12 h time zones, respectively. Each row represents the current phase of the circadian system on the day of arrival. The CBTmin shifts by 0.5 days per time zone crossed, i.e. delays by 2 h per day and application of interventions need to be adapted according to the shifting of the CBTmin. b Depicts eastward travel with the first row illustrating normal home time. The next three rows illustrate travel crossing 4, 8 and 12 h time zones, respectively. Each row represents the current phase of the circadian system on the day of arrival. The CBTmin shifts by 1 day per time zone crossed, i.e. advances by 1 h per day and application of interventions need to be adapted according to the shifting of the CBTmin. We constructed a recommendation based on a scientific measurement (CBTmin and DLMO) that can be reasonably applied for any number of time zones crossed. Travelling > 8 h EAST, it may be preferable to adapt by delay (moving backward) instead of advance (moving forward) as the body clock adjusts to large delays more easily than to large advances). Once CBTmin at the destination occurs within the scheduled sleep period, partial adaptation is achieved, and the individual is likely to encounter less sleep disruption. Once CBTmin at the destination occurs at the same time as pre-travel (home time), complete adaptation is achieved
8 Theoretical Concepts to Guide Future Research
To address the gaps in knowledge, high-quality multi-centre research that is repeatable and reliable is required in athletes, and utilising multi-disciplinary methodology in an attempt to adopt a holistic approach [146]. Specific measurements are required [e.g. CBT, melatonin, electroencephalogram (EEG)] otherwise the “research” will continue to either be surrogate measures, opinions or collective experiences.
For travel fatigue, randomised trials and longitudinal studies are needed to compare interventions aiming to reduce travel fatigue. Cabin conditions including seat size in buses, trains and planes can contribute to travel fatigue and require more research. The impact of specific parameters related to air travel, such as the average flight altitude, and the frequency and magnitude of atmospheric pressure, changes during the flight, which affects air cabin oxygen saturation levels are also worth exploring. Additionally, information on how travel fatigue is impacted following short distance (< 3 h) vs. long distance (> 3 h) travel, as well as the direction of travel (north–south/south–north, east–west/west–east) and the frequency of travel across a season is required. From a different perspective, there may be value in qualitative research evaluating how much athletes, coaches and support staff value and use monitoring tools. Determining the specific intervention, and the reason why coaches and athletes utilise these to minimise travel fatigue is also important. This is significant considering the burden which can be associated with athlete monitoring, the role of coaches and support staff in interpreting such data, concerns about whether such data are used in a meaningful manner, and the importance of athlete psychological health in perceived fatigue [147].
Well-controlled field-based jet lag studies that examine circadian adaptation and the impact of light exposure or avoidance schedules, using an appropriate phase marker, are required. To better understand risk factors and develop at-risk profiles for suitable interventions aligned to these profiles, tools to predict jet lag symptom severity and chronicity in individual travelling athletes need to be developed. Multi-centre studies exploring travel across a season, in competitions that involve frequent transmeridian travel (e.g. World Rugby 7 Series) rather than just assessing the impact of once-off travel will be valuable. Polysomnography (PSG) baseline data in more sports, sexes and age groups may be useful to identify sleep disorders in athletes and those who may be more at risk when travelling and also to compare PSG data on return to home to assess how long it takes for sleep to normalise.
9 Conclusion
This review and consensus statement highlights the complexity and lack of empirical research surrounding the measurement and management of travel fatigue and jet lag in athletes, curtailing the provision of strong recommendations. It concurs that travel fatigue and jet lag can inflict real and impactful issues on athletes regarding their performance and risk of illness or injury. Considering strategies pre-flight, during flight and after arrival at the destination, experts working in the field reached consensus on the management of travel fatigue and jet lag in athletes. Travel toolboxes covering fundamental principles and expert consensus recommendation for interventions are provided. Key interventions after travel include adjusting the sleep–wake cycle to counter travel fatigue and maximising the rate at which the body clock adapts to the new time zone by specifying 3 h periods of light exposure and avoidance to reduce jet lag. Importantly, inappropriate exposure may be counter-productive causing detrimental side effects. Lastly, this review outlines specific steps to advance theory and practice in the field, suggesting detailed areas of future research on travel fatigue and jet lag management in athletes.
References
Arendt J, Marks V. Physiological changes underlying jet lag. Br Med J (Clin Res Ed). 1982;284(6310):144–6.
Waterhouse J, Reilly T, Atkinson G, Edwards B. Jet lag: trends and coping strategies. Lancet. 2007;369(9567):1117–29.
Van DCJR, van Rensburg AJ, Schwellnus MP. Coping with jet lag and protecting athlete health when travelling. Aspetar Sports Med J. 2019;8(19):214–22.
Samuels CH. Jet lag and travel fatigue: a comprehensive management plan for sport medicine physicians and high-performance support teams. Clin J Sport Med. 2012;22(3):268–73.
Eastman CI, Burgess HJ. How to travel the world without jet lag. Sleep Med Clin. 2009;4(2):241–55.
McGuckin TA, Sinclair WH, Sealey RM, Bowman P. The effects of air travel on performance measures of elite Australian rugby league players. Eur J Sport Sci. 2014;14(sup1):S116–22.
Richmond LK, Dawson B, Stewart G, Cormack S, Hillman DR, Eastwood PR. The effect of interstate travel on the sleep patterns and performance of elite Australian Rules footballers. J Sci Med Sport. 2007;10(4):252–8.
Fowler P, Duffield R, Vaile J. Effects of domestic air travel on technical and tactical performance and recovery in soccer. Int J Sports Physiol Perform. 2014;9(3):378–86.
Fowler P, Duffield R, Vaile J. Effects of simulated domestic and international air travel on sleep, performance, and recovery for team sports. Scand J Med Sci Sports. 2015;25(3):441–51.
Reilly T, Waterhouse J, Edwards B. Some chronobiological and physiological problems associated with long-distance journeys. Travel Med Infect Dis. 2009;7(2):88–101.
Reilly T, Waterhouse J, Edwards B. Jet lag and air travel: implications for performance. Clin Sports Med. 2005;24(2):367–80.
Atkinson G, Batterham AM, Dowdall N, Thompson A, van Drongelen A. From animal cage to aircraft cabin: an overview of evidence translation in jet lag research. Eur J Appl Physiol. 2014;114(12):2459–68.
Arendt J. Managing jet lag: some of the problems and possible new solutions. Sleep Med Rev. 2009;13(4):249–56.
Reilly T, Atkinson G, Edwards B, Waterhouse J, Åkerstedt T, Davenne D, et al. Coping with jet-lag: a position statement for the European College of Sport Science. Eur J Sport Sci. 2007;7(1):1–7.
Foster RG, Kreitzman L. The rhythms of life: what your body clock means to you! Exp Physiol. 2014;99(4):599–606.
Zee PC, Attarian H, Videnovic A. Circadian rhythm abnormalities. Continuum. 2013;19(1 Sleep Disorders):132.
Golombek DA, Casiraghi LP, Agostino PV, Paladino N, Duhart JM, Plano SA, et al. The times they’re a-changing: effects of circadian desynchronization on physiology and disease. J Physiol Paris. 2013;107(4):310–22.
Dibner C, Schibler U, Albrecht U. The mammalian circadian timing system: organization and coordination of central and peripheral clocks. Annu Rev Physiol. 2010;72:517–49.
Adan A, Archer SN, Hidalgo MP, Di Milia L, Natale V, Randler C. Circadian typology: a comprehensive review. Chronobiol Int. 2012;29(9):1153–75.
van Rensburg DCJ, van Rensburg AJ, Fowler P, Fullagar HK, Stevens D, Halson S, et al. How to manage travel fatigue and jet lag in athletes? A systematic review of interventions. Br J Sports Med. 2020;54(16):960–8. https://doi.org/10.1136/bjsports-2019-101635.
Roach GD, Sargent C. Interventions to minimise jet lag after westward and eastward flight. Front Physiol. 2019;10:927.
Harbour R, Miller J. A new system for grading recommendations in evidence based guidelines. BMJ. 2001;323(7308):334–6.
Diamond IR, Grant RC, Feldman BM, Pencharz PB, Ling SC, Moore AM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. 2014;67(4):401–9.
Buchheit M. Houston, we still have a problem. Int J Sports Physiol Perform. 2017;12(8):1111–4.
Lewin R. Making waves: Irving Dardik and his superwave principle. Rodale; 2005.
Rollag MD, Berson DM, Provencio I. Melanopsin, ganglion-cell photoreceptors, and mammalian photoentrainment. J Biol Rhythms. 2003;18(3):227–34.
Foster RG, Hankins MW. Circadian vision. Curr Biol. 2007;17(17):R746–51.
Foster RG. Neurobiology: bright blue times. Nature. 2005;433(7027):698.
Lucas RJ, Freedman MS, Muñoz M, Garcia-Fernández J-M, Foster RG. Regulation of the mammalian pineal by non-rod, non-cone, ocular photoreceptors. Science. 1999;284(5413):505–7.
Simpson N, Gibbs E, Matheson G. Optimizing sleep to maximize performance: implications and recommendations for elite athletes. Scand J Med Sci Sports. 2017;27(3):266–74.
Hull JT, Czeisler CA, Lockley SW. Suppression of melatonin secretion in totally visually blind people by ocular exposure to white light: clinical characteristics. Ophthalmology. 2018;125(8):1160–71.
Borbély AA, Daan S, Wirz-Justice A, Deboer T. The two-process model of sleep regulation: a reappraisal. J Sleep Res. 2016;25(2):131–43.
Rupp TL, Wesensten NJ, Bliese PD, Balkin TJ. Banking sleep: realization of benefits during subsequent sleep restriction and recovery. Sleep. 2009;32(3):311–21.
Dement WC. Sleep extension: getting as much extra sleep as possible. Clin Sports Med. 2005;24(2):251–68.
Halberg F. The 24-hour scale: a time dimension of adaptive functional organization. Perspect Biol Med. 1960;3(4):491–527.
Patke A, Young MW, Axelrod S. Molecular mechanisms and physiological importance of circadian rhythms. Nat Rev Mol Cell Biol. 2020;21(2):67–84.
Martinez-Nicolas A, Madrid JA, Rol MA. Day–night contrast as source of health for the human circadian system. Chronobiol Int. 2014;31(3):382–93.
Roenneberg T, Merrow M. The circadian clock and human health. Curr Biol. 2016;26(10):R432–45.
Schulz P, Steimer T. Neurobiology of circadian systems. CNS Drugs. 2009;23(2):3–13.
Buttgereit F, Smolen JS, Coogan AN, Cajochen C. Clocking in chronobiology in rheumatoid arthritis. Nat Rev Rheumatol. 2015;11(6):349.
Hood S, Amir S. The aging clock: circadian rhythms and later life. J Clin Investig. 2017;127(2):437–46.
Baker FC, Waner JI, Vieira EF, Taylor SR, Driver HS, Mitchell D. Sleep and 24 hour body temperatures: a comparison in young men, naturally cycling women and women taking hormonal contraceptives. J Physiol. 2001;530(3):565–74.
Waterhouse J, Drust B, Weinert D, Edwards B, Gregson W, Atkinson G, et al. The circadian rhythm of core temperature: origin and some implications for exercise performance. Chronobiol Int. 2005;22(2):207–25.
Lack L, Lushington K. The rhythms of human sleep propensity and core body temperature. J Sleep Res. 1996;5(1):1–11.
Krauchi K, Wirz-Justice A. Circadian rhythm of heat production, heart rate, and skin and core temperature under unmasking conditions in men. Am J Physiol Regul Integr Comp Physiol. 1994;267(3):R819–29.
Richardson GS. The human circadian system in normal and disordered sleep. J Clin Psychiatry. 2005;66(15):3–9.
Berry RB, Wagner MH. Sleep medicine pearls e-book. Elsevier; 2014.
Arendt J. Approaches to the pharmacological management of jet lag. Drugs. 2018;78(14):1419–31.
Bin YS, Postnova S, Cistulli PA. What works for jetlag? A systematic review of non-pharmacological interventions. Sleep Med Rev. 2019;43:47–59.
Barion A, Zee PC. A clinical approach to circadian rhythm sleep disorders. Sleep Med. 2007;8(6):566–77.
Kripke DF, Elliott JA, Youngstedt SD, Rex KM. Circadian phase response curves to light in older and young women and men. J Circadian Rhythms. 2007;5(1):1–13.
Zee PC. Science of circadian rhythms, an issue of sleep medicine clinics. Elsevier; 2015.
St Hilaire MA, Gooley JJ, Khalsa SBS, Kronauer RE, Czeisler CA, Lockley SW. Human phase response curve to a 1 h pulse of bright white light. J Physiol. 2012;590(13):3035–45.
Rüger M, St Hilaire MA, Brainard GC, Khalsa SBS, Kronauer RE, Czeisler CA, et al. Human phase response curve to a single 6.5 h pulse of short-wavelength light. J Physiol. 2013;591(1):353–63.
Atkinson G, Drust B, Reilly T, Waterhouse J. The relevance of melatonin to sports medicine and science. Sports Med. 2003;33(11):809–31.
LeGates TA, Fernandez DC, Hattar S. Light as a central modulator of circadian rhythms, sleep and affect. Nat Rev Neurosci. 2014;15(7):443–54.
Burgess HJ, Sharkey KM, Eastman CI. Bright light, dark and melatonin can promote circadian adaptation in night shift workers. Sleep Med Rev. 2002;6(5):407–20.
Vitale JA, Weydahl A. Chronotype, physical activity, and sport performance: a systematic review. Sports Med. 2017;47(9):1859–68.
Díaz-Morales JF. Morning and evening-types: exploring their personality styles. Pers Individ Differ. 2007;43(4):769–78.
Darwent D, Dawson D, Roach GD. Prediction of probabilistic sleep distributions following travel across multiple time zones. Sleep. 2010;33(2):185–95.
Reilly T, Atkinson G, Waterhouse J. Travel fatigue and jet-lag. J Sports Sci. 1997;15:365–9.
Postolache TT, Hung T-M, Rosenthal RN, Sorianoa JJ, Montese F, Stiller JW. Sports chronobiology consultation: from the lab to the arena. Clin Sports Med. 2005;24:415–56.
Wittmann M, Dinich J, Merrow M, Roenneberg T. Social jetlag: misalignment of biological and social time. Chronobiol Int. 2006;23(1–2):497–509.
Fabbian F, Zucchi B, De Giorgi A, Tiseo R, Boari B, Salmi R, et al. Chronotype, gender and general health. Chronobiol Int. 2016;33(7):863–82.
Montaruli A, Galasso L, Caumo A, Cè E, Pesenti C, Roveda E, et al. The circadian typology: the role of physical activity and melatonin. Sport Sci Health. 2017;13:469–476
Wennman H, Kronholm E, Partonen T, Peltonen M, Vasankari T, Borodulin K. Evening typology and morning tiredness associates with low leisure time physical activity and high sitting. Chronobiol Int. 2015;32(8):1090–100.
Vitale JA, La Torre A, Baldassarre R, Piacentini MF, Bonato M. Ratings of perceived exertion and self-reported mood state in response to high intensity interval training. A crossover study on the effect of chronotype. Front Psychol. 2017;8:1232.
Lastella M, Roach GD, Halson SL, Sargent C. The chronotype of elite athletes. J Hum Kinet. 2016;54(1):219–25.
Archer SN, Robilliard DL, Skene DJ, Smits M, Williams A, Arendt J, et al. A length polymorphism in the circadian clock gene Per3 is linked to delayed sleep phase syndrome and extreme diurnal preference. Sleep. 2003;26(4):413–5.
Reilly T. How can travelling athletes deal with jet-lag? Kinesiology. 2009;41(2):128–35.
Waterhouse J, Reilly T, Edwards B. The stress of travel. J Sports Sci. 2004;22(10):946–66.
Calleja-Gonzalez J, Marques-Jimenez D, Jones M, Huyghe T, Navarro F, Delextrat A, et al. What are we doing wrong when athletes report higher levels of fatigue from traveling than from training or competition? Front Psychol. 2020;11:194.
Flower DJ, Irvine D, Folkard S. Perception and predictability of travel fatigue after long-haul flights: a retrospective study. Aviat Space Environ Med. 2003;74(2):173–9.
Waterhouse J, Edwards B, Nevill A, Atkinson G, Reilly T, Davies P, et al. Do subjective symptoms predict our perception of jet-lag? Ergonomics. 2000;43(10):1514–27.
Cesarone MR, Belcaro G, Errichi BM, Nicolaides AN, Geroulakos G, Ippolito E, et al. The LONFLIT4-Concorde deep venous thrombosis and edema study: prevention with travel stockings. Angiology. 2003;54(2):143–54.
Basri B, Griffin MJ. Predicting discomfort from whole-body vertical vibration when sitting with an inclined backrest. Appl Ergon. 2013;44(3):423–34.
Smulders M, Naddeo A, Cappetti N, van Grondelle E, Schultheis U, Vink P. Neck posture and muscle activity in a reclined business class aircraft seat watching IFE with and without head support. Appl Ergon. 2019;79:25–37.
Hamada K, Doi T, Sakurai M, Matsumoto K, Yanagisawa K, Suzuki T, et al. Effects of hydration on fluid balance and lower-extremity blood viscosity during long airplane flights. JAMA. 2002;287(7):844–5.
Leatherwood WE, Dragoo JL. Effect of airline travel on performance: a review of the literature. Br J Sports Med. 2013;47(9):561–7.
Coste O, Van Beers P, Touitou Y. Hypoxia-induced changes in recovery sleep, core body temperature, urinary 6-sulphatoxymelatonin and free cortisol after a simulated long-duration flight. J Sleep Res. 2009;18(4):454–65.
Geertsema C, Williams AB, Dzendrowskyj P, Hanna C. Effect of commercial airline travel on oxygen saturation in athletes. Br J Sports Med. 2008;42(11):877–81.
Halson SL, Burke LM, Pearce J. Nutrition for travel: From jet lag to catering. Int J Sport Nutr Exerc Metab. 2019;29(2):228–35.
Lastella M, Roach GD, Sargent C. Travel fatigue and sleep/wake behaviors of professional soccer players during international competition. Sleep Health. 2019;5(2):141–7.
Thompson CJ, Noon M, Towlson C, Perry J, Coutts AJ, Harper LD, et al. Understanding the presence of mental fatigue in English academy soccer players. J Sports Sci. 2020;38(13):1524–30.
Hede AJ. Using mindfulness to reduce the health effects of community reaction to aircraft noise. Noise Health. 2017;19(89):165.
Fowler P, Duffield R, Howle K, Waterson A, Vaile J. Effects of northbound long-haul international air travel on sleep quantity and subjective jet lag and wellness in professional Australian soccer players. Int J Sports Physiol Perform. 2015;10(5):648–54.
Sampaio J, McGarry T, Calleja-González J, Jiménez Sáiz S, del Alcázar XS, Balciunas M. Exploring game performance in the National Basketball Association using player tracking data. PLoS ONE. 2015;10(7):e0132894.
Macdonald B, Pulleyblank W. Realignment in the NHL, MLB, NFL, and NBA. J Quant Anal Sports. 2014;10(2):225–40.
Hooper SL, Mackinnon LT. Monitoring overtraining in athletes. Recommendations. Sports Med. 1995;20(5):321–7.
Kentta G, Hassmen P. Overtraining and recovery. A conceptual model. Sports Med. 1998;26(1):1–16 (PM:9739537).
Nässi A, Ferrauti A, Meyer T, Pfeiffer M, Kellmann M. Development of two short measures for recovery and stress in sport. Eur J Sport Sci. 2017;17(7):894–903.
Coutts AJ, Slattery KM, Wallace LK. Practical tests for monitoring performance, fatigue and recovery in triathletes. J Sci Med Sport. 2007;10(6):372–81.
van Rensburg DCJ, Fowler P, Racinais S. Practical tips to manage travel fatigue and jet lag in athletes. Br J Sports Med. 2020. https://doi.org/10.1136/bjsports-2020-103163.
Walsh NP, Halson SL, Sargent C, Roach GD, Nédélec M, Gupta L, et al. Sleep and the athlete: narrative review and 2021 expert consensus recommendations. Br J Sports Med. 2021;55(7):356–68.
Roach GD, Matthews R, Naweed A, Kontou TG, Sargent C. Flat-out napping: the quantity and quality of sleep obtained in a seat during the daytime increase as the angle of recline of the seat increases. Chronobiol Int. 2018;35(6):872–83.
Berry RB, Gamaldo CE, Harding SM, Brooks R, Lloyd RM, Vaughn BV, Marcus CL. AASM Scoring Manual Version 2.2 updates: new chapters for scoring infant sleep staging and home sleep apnea testing. J Clin Sleep Med 2015;11(11):1253–4.
Dunican IC, Walsh J, Higgins CC, Jones MJ, Maddison K, Caldwell JA, et al. Prevalence of sleep disorders and sleep problems in an elite super rugby union team. J Sports Sci. 2019;37(8):950–7.
Saugy JJ, Schmitt L, Fallet S, Faiss R, Vesin J-M, Bertschi M, et al. Sleep disordered breathing during live high-train low in normobaric versus hypobaric hypoxia. High Alt Med Biol. 2016;17(3):233–8.
Sargent C, Schmidt WF, Aughey RJ, Bourdon PC, Soria R, Claros JCJ, et al. The impact of altitude on the sleep of young elite soccer players (ISA3600). Br J Sports Med. 2013;47(Suppl 1):i86–92.
Roach GD, Schmidt WF, Aughey RJ, Bourdon PC, Soria R, Claros JCJ, et al. The sleep of elite athletes at sea level and high altitude: a comparison of sea-level natives and high-altitude natives (ISA3600). Br J Sports Med. 2013;47(Suppl 1):i114–20.
Australian Institute of Sport AIS A message from the AIS CMO on travel risk management. Available from: https://www.sportaus.gov.au/media-centre/news/a-message-fromthe-ais-cmo-on-travel-risk-management. Accessed Aug 2020.
Baker LB, Jeukendrup AE. Optimal composition of fluid-replacement beverages. Compr Physiol. 2011;4(2):575–620.
Evans GH, James LJ, Shirreffs SM, Maughan RJ. Optimizing the restoration and maintenance of fluid balance after exercise-induced dehydration. J Appl Physiol. 2017;122(4):945–51.
Wever RA. Phase shifts of human circadian rhythms due to shifts of artificial Zeitgebers. Chronobiologia. 1980;7:303–27.
Winget CM, DeRoshia CW, Markley CL, Holley DC. A review of human physiological and performance changes associated with desynchronosis of biological rhythms. Aviat Space Environ Med. 1984;55(12):1085–96.
Sack RL. Jet lag. N Engl J Med. 2010;362(5):440–7.
Ledger S, Bin YS, Nour M, Cistulli P, Bauman A, Allman-Farinelli M, et al. Internal consistency and convergent and divergent validity of the Liverpool jetlag questionnaire. Chronobiol Int. 2020;37(2):218–26.
Spitzer R, Terman M, Williams J, Terman J, Malt U, Singer F, et al. Jet lag: clinical features, validation of a new syndrome-specific scale, and lack of response to melatonin in a randomised, double-blind trial. Am J Psychiat. 1999;156:1392–6.
Sack RL, Auckley D, Auger RR, Carskadon MA, Wright KP Jr, Vitiello MV, et al. Circadian rhythm sleep disorders: part I, basic principles, shift work and jet lag disorders. Sleep. 2007;30(11):1460–83.
Miller DJ, Sargent C, Vincent GE, Roach GD, Halson SL, Lastella M. Sleep/wake behaviours in elite athletes from three different football codes. J Sports Sci Med. 2017;16(4):604.
Fullagar HH, Duffield R, Skorski S, White D, Bloomfield J, Kölling S, et al. Sleep, travel, and recovery responses of national footballers during and after long-haul international air travel. Int J Sports Physiol Perform. 2016;11(1):86–95.
Paul MA, Miller JC, Gray GW, Love RJ, Lieberman HR, Arendt J. Melatonin treatment for eastward and westward travel preparation. Psychopharmacology. 2010;208(3):377–86.
Dijk DJ, Dufy J. Novel approaches for assessing circadian rhythmicity in humans: A review. J Biol Rhythms. 2020;35(5):421–38.
Dijk D-J, Duffy JF, Silva EJ, Shanahan TL, Boivin DB, Czeisler CA. Amplitude reduction and phase shifts of melatonin, cortisol and other circadian rhythms after a gradual advance of sleep and light exposure in humans. PLoS ONE. 2012;7(2):e30037.
Rutters F, Lemmens SG, Adam TC, Bremmer MA, Elders PJ, Nijpels G, et al. Is social jetlag associated with an adverse endocrine, behavioral, and cardiovascular risk profile? J Biol Rhythms. 2014;29(5):377–83.
British Airways. Jet lag advisor. Available from: https://www.britishairways.com/travel/drsleep/public/en_gb. Accessed 28 Jun 2020.
Jet Lag Rooster: In conjunction with the Mayo Clinic Center for Sleep Medicine and Rush University Medical Center. Available from: www.jetlagrooster.com. Accessed 28 Jun 2020.
Timeshifter. The Jet Lag App. Available from: https://www.timeshifter.com/. Accessed 28 Jun 2020.
Simmons E, McGrane O, Wedmore I. Jet lag modification. Curr Sports Med Rep. 2015;14(2):123–8.
Fowler PM, Knez W, Crowcroft S, Mendham AE, Miller J, Sargent C, et al. Greater effect of east versus west travel on jet lag, sleep, and team sport performance. Med Sci Sports Exerc. 2017;49(12):2548–61.
Vitale KC, Owens R, Hopkins SR, Malhotra A. Sleep hygiene for optimizing recovery in athletes: review and recommendations. Int J Sports Med. 2019;40(8):535.
Leonardo-Mendonça RC, Martinez-Nicolas A, de Teresa GC, Ocaña-Wilhelmi J, Rusanova I, Guerra-Hernández E, et al. The benefits of four weeks of melatonin treatment on circadian patterns in resistance-trained athletes. Chronobiol Int. 2015;32(8):1125–34.
Jurvelin H, Takala T, Nissilä J, Timonen M, Rüger M, Jokelainen J, et al. Transcranial bright light treatment via the ear canals in seasonal affective disorder: a randomized, double-blind dose-response study. BMC Psychiatry. 2014;14(1):1–11.
Waterhouse J, Edwards B, Nevill A, Carvalho S, Atkinson G, Buckley P, et al. Identifying some determinants of “jet lag” and its symptoms: a study of athletes and other travellers. Br J Sports Med. 2002;36(1):54–60.
Youngstedt SD, Elliott JA, Kripke DF. Human circadian phase–response curves for exercise. J Physiol. 2019;597(8):2253–68.
Piérard C, Beaumont M, Enslen M, Chauffard F, Tan D-X, Reiter RJ, et al. Resynchronization of hormonal rhythms after an eastbound flight in humans: effects of slow-release caffeine and melatonin. Eur J Appl Physiol. 2001;85(1–2):144–50.
Sainz I, Collado-Mateo D, Del Coso J. Effect of acute caffeine intake on hit accuracy and reaction time in professional e-sports players. Physiol Behav. 2020;224:113031.
Burke TM, Markwald RR, McHill AW, Chinoy ED, Snider JA, Bessman SC, et al. Effects of caffeine on the human circadian clock in vivo and in vitro. Sci Transl Med. 2015;7(305):305ra146.
Pujalte GG, Benjamin HJ. Sleep and the athlete. Curr Sports Med Rep. 2018;17(4):109–10.
Badr MS, Belenky G, Bliwise DL, Buxton OM, Buysse D, Dinges DF, et al. Recommended amount of sleep for a healthy adult: a joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. J Clin Sleep Med. 2015;11(06):591–2.
Arnal PJ, Lapole T, Erblang M, Guillard M, Bourrilhon C, Leger D, et al. Sleep extension before sleep loss: effects on performance and neuromuscular function. Med Sci Sports Exerc. 2016;48(8):1595–603.
Drake C, Roehrs T, Shambroom J, Roth T. Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed. J Clin Sleep Med. 2013;9(11):1195–200.
Stutz J, Eiholzer R, Spengler CM. Effects of evening exercise on sleep in healthy participants: a systematic review and meta-analysis. Sports Med. 2019;49(2):269–87.
Potter GD, Cade JE, Grant PJ, Hardie LJ. Nutrition and the circadian system. Br J Nutr. 2016;116(3):434–42.
Oike H. Modulation of circadian clocks by nutrients and food factors. Biosci Biotechnol Biochem. 2017;81(5):863–70.
Herxheimer A. Jet lag. BMJ Clin Evid. 2014;2014:2303.
Thomas D, Erdman K, Burke L, American College of Sports Medicine Joint Position Statement. Nutrition and athletic performance. Med Sci Sports Exerc. 2016;48(3):543–68.
Herxheimer A, Petrie KJ. Melatonin for the prevention and treatment of jet lag. Cochrane Database Syst Rev. 2002. Available from: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD001520/full. Accessed Jun 2018.
Morin CM, Benca R. Chronic insomnia. Lancet. 2012;379(9821):1129–41.
Rajaratnam SM, Polymeropoulos MH, Fisher DM, Roth T, Scott C, Birznieks G, et al. Melatonin agonist tasimelteon (VEC-162) for transient insomnia after sleep-time shift: two randomised controlled multicentre trials. Lancet. 2009;373(9662):482–91.
Zee PC, Wang-Weigand S, Wright KP Jr, Peng X, Roth T. Effects of ramelteon on insomnia symptoms induced by rapid, eastward travel. Sleep Med. 2010;11(6):525–33.
Cook CJ, Crewther BT, Kilduff LP, Drawer S, Gaviglio CM. Skill execution and sleep deprivation: effects of acute caffeine or creatine supplementation-a randomized placebo-controlled trial. J Int Soc Sports Nutr. 2011;8(1):2.
Beaumont M, Batejat D, Pierard C, Van Beers P, Denis J-B, Coste O, et al. Caffeine or melatonin effects on sleep and sleepiness after rapid eastward transmeridian travel. J Appl Physiol. 2004;96(1):50–8.
Burgess HJ, Molina TA. Home lighting before usual bedtime impacts circadian timing: a field study. Photochem Photobiol. 2014;90(3):723–6.
WADA. World Anti-Doping Agency. Prohibited list. Montreal. Available from: https://www.wada-ama.org/en/what-we-do/prohibited-list. Accessed Jun 2020.
Lo M, Aughey RJ, Stewart AM, Gill N, McDonald B. The road goes ever on and on-a socio-physiological analysis of travel-related issues in Super Rugby. J Sports Sci. 2021;39(3):289–95.
Miles KH, Clark B, Fowler PM, Miller J, Pumpa KL. Sleep practices implemented by team sport coaches and sports science support staff: a potential avenue to improve athlete sleep? J Sci Med Sport. 2019;22(7):748–52.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No sources of funding were used to assist in the preparation of this article.
Conflict of interest
Dina C (Christa) Janse Van Rensburg, Audrey Jansen van Rensburg, Peter M Fowler, Amy M Bender, David Stevens, Kieran O Sullivan, Hugh HK Fullagar, Juan-Manuel Alonso, Michelle Biggins, Amanda Claassen-Smithers, Rob Collins, Michiko Dohi, Matthew W Driller, Ian C Dunican, Luke Gupta, Shona L Halson, Michele Lastella, Kathleen H Miles, Mathieu Nedelec, Tony Page, Greg Roach, Charli Sargent, Meeta Singh, Grace E. Vincent, Jacopo A. Vitale, Tanita Botha declare that they have no conflicts of interest relevant to the content of this review.
Ethical approval
Ethical approval was received from the University of Pretoria, South Africa (REC 428/2015).
Consent to participate
Not applicable.
Consent for publication
All Authors approved of this version for publication.
Availability of data and material
Not applicable.
Code availability
Not applicable.
Authors’ contributions
Dina C (Christa) Janse van Rensburg (DCJvR): consensus concept, manuscript planning, manuscript writing (first draft), development of surveys towards consensus voting, manuscript review and editing, approved the version to be published. Audrey Jansen van Rensburg (AJvR): manuscript planning, manuscript writing (first draft), development of surveys towards consensus voting, manuscript review and editing, approved the version to be published. Peter Fowler (PF): manuscript planning, manuscript writing (first draft), consensus voting, manuscript review and editing, approved the version to be published. Amy Bender (AB): group lead for terminology section, manuscript writing (first draft), development of surveys towards consensus voting, manuscript review and editing, approved the version to be published. David Stevens (DS): group lead for human circadian section, manuscript writing (first draft), consensus voting, manuscript review and editing, approved the version to be published. Kieran O Sullivan (KoS): group lead for travel fatigue section, manuscript writing (first draft), consensus voting, manuscript review and editing, approved the version to be published. Hugh Fullagar (HF): group lead for jet lag section, manuscript writing (first draft), consensus voting, manuscript review and editing, approved the version to be published. Tanita Botha (TB): statistician, manuscript writing (first draft), development of surveys towards consensus voting, analyses of surveys, manuscript review and editing, approved the version to be published. All other co-authors [Juan-Manuel Alonso (JMA), Michelle Biggins (MB), Amanda Claassen-Smithers (ACS), Rob Collins (RC), Michiko Dohi (MDo), Matthew Driller (MD), Ian Dunican (ID), Luke Gupta (LG), Shona Halson (SH), Michele Lastella (ML), Kathleen Miles (KM), Mathieu Nedelec (MN), Tony Page (TP), Greg Roach (GR), Charli Sargent (CS), Meeta Singh (MS), Grace Vincent (GV), Jacopo A. Vitale (JV)] contributed to manuscript writing (first draft), consensus voting, manuscript review and editing, approved the final version to be published.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Janse van Rensburg, D.C., Jansen van Rensburg, A., Fowler, P.M. et al. Managing Travel Fatigue and Jet Lag in Athletes: A Review and Consensus Statement. Sports Med 51, 2029–2050 (2021). https://doi.org/10.1007/s40279-021-01502-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-021-01502-0