
Abstract
Introduction
Healthcare professionals tend to recommend emollients based primarily on patient/consumer preference and cost, with cheaper options assumed to be therapeutically equivalent. The aim of this study was therefore to compare the effects on skin hydration of two emollients prescribed in the UK, Doublebase Dayleve™ gel (DELP) and a cheaper alternative, Zerobase Emollient™ cream (ZBC).
Methods
This was a single-centre, randomised, double-blind, concurrent bi-lateral (within-patient) comparison in 18 females with atopic eczema and dry skin on their lower legs. DELP gel and ZBC cream were each applied to one lower leg twice daily for 4 days and on the morning only on day 5. The efficacy of both products was assessed by hydration measurements using a Corneometer CM825 probe (Courage-Khazaka Electronic). The measurements were made three times daily on days 1 to 5. The primary efficacy variable was the area under the curve (AUC) of the change from baseline corneometer readings over the 5 days.
Results
Skin hydration using DELP gel was significantly higher than using ZBC cream (p < 0.0001). The cumulative increase in skin hydration observed for DELP gel was substantial and long lasting. In contrast, for ZBC cream, there was no significant improvement of the cumulative skin hydration as measured by the AUC (p = 0.22).
Conclusion
DELP gel achieved substantial, long-lasting and cumulative skin hydration, whilst ZBC cream achieved no measurable improvement in skin hydration compared to before treatment. Healthcare professionals should be aware that different emollients can perform differently.
Funding
Dermal Laboratories Ltd.
Trial Registration
EudraCT number:2014-001026-16.
Similar content being viewed by others



Introduction
Atopic eczema (AE) is a chronic, relapsing, inflammatory disease affecting up to 20% of children and young adults [1]. The key characteristics of the disease are loss of skin barrier function leading to generalised skin dryness, with some areas exhibiting redness and inflammation that invariably become itchy [2].
Emollient therapy is the first-line treatment for AE and works chiefly by maintaining increased skin water content, particularly in the outermost stratum corneum layer [3,4,5]. There is a lack of good-quality evidence on the effectiveness of emollients in atopic patients, especially when used under conditions more relevant to real-life situations [3, 5,6,7,8,9]. Some healthcare professionals are under the impression that all emollient preparations are equally effective. As a result, these products tend to be recommended based primarily on patient/consumer preference and cost, with cheaper options assumed to be therapeutically equivalent. However, in the UK, the National Institute for Health and Care Excellence (NICE) recognises that there is a lack of comparative data on emollients and has urged more research to be conducted in this area [5].
The aim of this study was to compare two emollients prescribed in the UK: one, a licensed medicine formally approved by the Medicines and Healthcare products Regulatory Agency, namely Doublebase Dayleve™ gel, PL 00173/0199 (DELP); the other, a cheaper and self-certified Class I medical device, namely Zerobase Emollient™ cream (ZBC). Their compositions are listed in Table 1. Their performances were compared using objective corneometry measurements of cumulative effects on skin hydration, and using patients’ subjective assessment of product acceptability.
Methods
The study design was a single-centre, double-blind, randomised, concurrent bilateral (within-patient) comparison of DELP gel (Dermal Laboratories Ltd, Hitchin, UK) and ZBC cream (Thornton & Ross Ltd, Huddersfield, UK) applied to the lower legs of atopic eczema sufferers (as confirmed by the investigator according to the NICE standard diagnostic criteria [5]), between 16 and 65 years of age.
The study was conducted with full ethics (NRES Committee South Central-Berkshire B, UK) and regulatory approvals, and in compliance with the principles of the Declaration of Helsinki and in accordance with Good Clinical Practice (GCP). It was registered on the EU Clinical Trials Register (EudraCT number:2014-001026-16). Written informed consents were obtained from all subjects.
Participation was restricted to females only because it is well documented that excessive hair interferes with corneometry measurements [10]. Eligible subjects committed to following a sedentary lifestyle during the study (to avoid more frequent washing/bathing than permitted).
Exclusion criteria were: significant concurrent illness or skin disease currently involving the test sites; systemic disease that may adversely influence participation in the trial, history of allergy relevant to the test products or their ingredients; use of any topical or systemic treatment likely to affect skin response; use of oral and topical (on lower legs) antibiotics, steroids and immunosuppressants for any condition within the previous 4 weeks; use of any unlicensed medicine within the previous 30 days, visible skin abnormality or excessive hair growth likely to interfere with instrumental measurements; irritation, tattoos, scars or birthmarks at the test measurement sites; participation in any irritation or sensitisation study presently or within the past 3 months; having another member of the household enrolled in the study; breastfeeding and pregnancy; being of child-bearing potential and not taking adequate contraceptive precautions; and being unable or unlikely to attend the necessary follow-up visits. Also, removal of leg hair was not allowed within 48 h prior to or during participation. Patients were asked to avoid excessive exposure of the test sites to natural sunlight, sun beds or sun lamps, and not to use any skin-tanning products on these sites. Employees of either Reading Clinical Research or Dermal Laboratories, or their immediate family members, were not allowed to participate.
Consenting patients were entered into a 1-week washout/run-in period where they were given Simple® soap (see Table 1 for details of composition and manufacturer) to use for washing, and asked not to apply any moisturising products to their lower legs and to avoid shaving or using depilatory products on these areass.
Following the 1-week washout/run-in, baseline measurements of skin hydration on both lower legs were performed using the Multiprobe Adapter MPA5 with a Corneometer CM825 probe (Hydration) (Courage-Khazaka Electronic, Germany) at about 0900 hours on day 1 on skin areas on the lower legs located in the same position for each subject using templates. To be eligible to progress to randomisation and the treatment phase, subjects’ baseline corneometer readings had to be less than 45 units (indicating that their skin was dry or very dry), and differing by no more than 6 units between their left and right legs.
The two test products are white semi-solids, essentially indistinguishable from one another in appearance and texture, and were presented, for blinding purposes, in identical 100-g pre-weighed white tubes, labelled left and right according to a randomisation prepared by the statistician. The labels were colour-coded to help compliance with the correct right and left leg assignment.
Subjects were asked to apply the products to their lower legs twice daily (immediately after the 0900 hours corneometry measurement and at approximately 2100 hours, at least 30 min before going to bed at night) for the next 4 days and on the morning only on day 5. This dosage regimen was consistent with most patients’ practical circumstances which limits their use of emollients to twice daily only. They were shown how to apply enough of each product to treat the whole of the respective lower leg (as a guide, described as being about 1 in (c.2.5 cm) of product squeezed from the tube or a mass about the size of a 20p piece) using a few gentle strokes to smooth the products across the skin in the direction of hair growth. Subjects’ first applications on day 1 were supervised at the study centre by personnel not involved in the corneometry measurements, to ensure they followed the correct left/right allocation of the two products, applied them to the whole of the respective lower leg (i.e. front and back, from the ankle to the knee) and avoided cross-contamination.
Corneometry measurements were performed three times daily (nominally 0900, 1300 and 1700 hours) for 5 consecutive days. Measurements were performed in triplicate.
While using the emollients, subjects were asked to refrain from bathing, showering or washing their lower legs at any time, except on days 2 and 4 when they were permitted to wash with Simple® soap before the evening applications. Subjects were not permitted to use any other skin moisturiser on their legs at any time during their participation in the study, nor any other topical or systemic medication considered by the chief investigator to potentially interfere with the study outcome.
Primary Efficacy Parameter
The primary efficacy parameter was the degree and duration of stratum corneum skin hydration as determined by the area under the curve (AUC) of the change in the skin corneometry measurements from baseline, collected for each leg over the 5-day treatment period. AUC was calculated using the trapezoidal rule using the arithmetic mean and the actual time recorded for the corneometry measurements (conducted in triplicate). The primary endpoint was analysed using a mixed model taking into account the within-patient design, with patient as a random effect and leg, randomised group and treatment as fixed effects and with baseline corneometry measurement as a covariate. Statistical significance was set at the 5% level (2-sided). The Full Analysis Set, which comprised all randomised patients, was used for this Intention-To-Treat analysis.
Secondary Efficacy Parameters
Secondary parameters included:
-
(a)
Comparison between DELP and ZBC in the change from baseline to the first corneometry measurement obtained on each of days 2 to 5.
-
(b)
Comparison of the first corneometry measurement on each of days 2, 3, 4 and 5 versus baseline for DELP and ZBC, separately.
-
(c)
Three patient-reported outcomes were recorded using a cosmetic acceptability questionnaire on day 5. These outcomes were: (1) overall acceptability, defined as the percentage of subjects ticking “Like Strongly” or “Like Slightly” from a list of 5 options, also including “Neither Like nor Dislike”, “Dislike Slightly” and “Dislike Strongly”; (2) whether the subjects would use each product again; and (3) whether the subject preferred either product.
A hierarchical testing regime was used for these secondary efficacy outcomes in order to preserve the overall significance level—i.e. they were only analysed if the primary endpoint was statistically significant at the 5% level, and then starting from day 5 through to day 2. The corneometry outcomes were analysed as for the primary outcome for comparisons between study treatments, and using paired t tests for analysis of each product separately. Prescott’s test was used for the patient-reported secondary outcomes. All statistical testing was 2-sided using a 5% significance level and in accordance with the protocol and the statistical analysis plan finalised prior to blind break.
For exploratory purposes, additional questions were asked in regard to product attributes, but these results are not presented as no statistical analysis of these attributes was undertaken.
This study was designed to test superiority for the primary efficacy parameter only. A sample size of 14 subjects was calculated to give 90% power to detect a difference in mean AUC of 524 between DELP and ZBC, using a 5% significance level. This difference in mean AUC was based on the results from a similar previous study [11]. Up to 20 subjects were therefore planned in order to allow for possible dropouts.
Results
Twenty-four potential subjects were screened. Three failed screening due to not having AE on their lower legs, so 21 commenced washout. Three of these later failed, due to their baseline corneometry readings being above 45 units, leaving 18 randomised to take part in the treatment phase. All 18 completed the study and were included in the analysis.
Five adverse events (all minor) were reported but none were considered as being possibly treatment related.
The study was performed in three cohorts (comprising 9, 3 and 6 subjects) and there were no major protocol deviations. Adherence with the twice daily treatment regimen (as recorded in subjects’ treatment diaries) was good, with only one subject failing to apply the study products on one occasion. Whilst there were no significant differences between the amounts of products used on left versus right legs, subjects used on average 22% more DELP than ZBC [mean difference being 2.5 g (95% CI 0.9–4.0 g)], while 94% of the subjects recorded that they bathed their lower legs or showered in the evening on day 2, and 100% on day 4.
Primary Efficacy Analysis
Over the 5-day treatment period, the cumulative increase in skin hydration, as measured by the AUC in change from baseline corneometer readings, was statistically significantly greater for the legs treated with DELP compared to the legs treated with ZBC (difference DELP − ZBC = 1601, 95% CI 1277–1924, p < 0.0001) (Table 2). For the legs treated with ZBC, the cumulative increase in skin hydration was not statistically different from zero (p = 0.22). The increase in skin hydration for legs treated with DELP was estimated to be approximately ten times that seen for ZBC.
The improved skin hydration of DELP over ZBC was seen at every time point over the 5-day period. The mean corneometer readings are shown in Fig. 1. The long-lasting and cumulative benefit of DELP over ZBC is particularly illustrated by the morning readings each day, taken typically 12 h after the latest application of the products the day before, which were significantly greater than the baseline reading (day 1, 0900 hours) and increased step-wise from day 2 through to day 5—even following the washing/bathing permitted during the evenings of days 2 and 4. In contrast, for ZBC cream, there was no significant improvement in the cumulative skin hydration as measured by the AUC.

Mean corneometer readings with 95% confidence interval
Secondary Efficacy Analysis
-
(a)
The mean change from baseline corneometry measurements for the first measurement of the day on days 2 to 5 are presented in Fig. 2. There was a large statistically significant difference (p < 0.05) between the study products in the change from baseline to the first corneometry measurement of the day on days, 2, 3, 4 and 5, with the DELP-treated legs showing much greater moisturisation than the legs treated with ZBC. The largest treatment difference was on day 4 (DELP–ZBC difference in change from baseline = 16.3, 95% CI 12–20, p < 0.0001).
Fig. 2 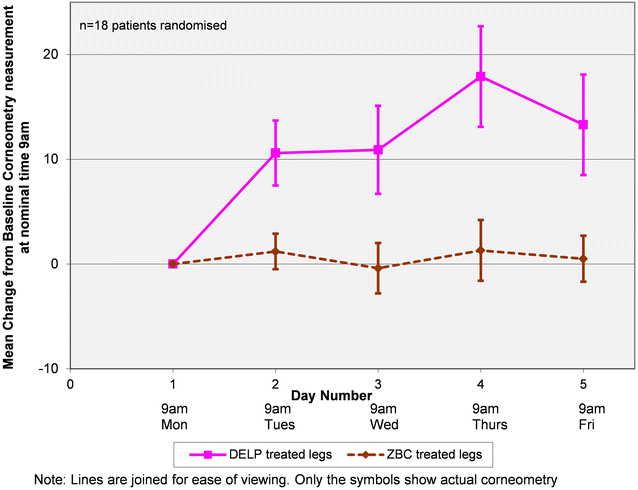
Mean and 95% CI change from baseline for the first corneometry measurement of each day
-
(b)
When analysed separately, for the legs treated with DELP, the first corneometry measurement on days 2 to 5 were significantly higher than baseline (Table 3). Since the first corneometry measurement of each day was nominally 12 h after the latest treatment application, the significant improvement in the first corneometry measurement on days 2 to 5, compared to the day 1 baseline, demonstrates that the hydration was long lasting. In contrast, the first corneometry measurements of the day for legs treated with ZBC were not significantly different from those at day 1 baseline, indicating that any hydration effects were short-lived.
Table 3 First corneometry measurements (days 2 to 5 vs. day 1) for DELP and ZBC separately -
(c)
Patient reported outcomes.
-
1.
Overall product acceptability
For DELP, 72% of subjects selected either “Like Slightly” or “Like Strongly” compared to 50% for ZBC (Table 4). This difference in overall product acceptability was not statistically significant (using Prescott’s test to allow for effect of leg, p = 0.61).
Table 4 Acceptability of DELP and ZBC -
2.
Willingness to use the products again
Two-thirds of subjects (67%) indicated that they would use DELP again, compared to 56% for ZBC (Table 5). Statistical testing was not performed in accordance with pre-determined Statistical Analysis Plan since the secondary efficacy analysis of overall product acceptability was not statistically significant.
Table 5 Willingness to use DELP and ZBC again -
3.
Product preference
All patients stated a preference, with two-thirds indicating that they preferred the product on the leg treated with DELP, and one-third of patients stating that they preferred the product on the leg treated with ZBC (Table 6). In accordance with the Statistical Analysis Plan, statistical testing was not performed since the secondary efficacy analysis of overall product acceptance was not statistically significant.
Table 6 Preferred treatment option
-
1.

Discussion
Atopic eczema (AE) is a chronic, relapsing, inflammatory disease mainly affecting children and young adults, and the key characteristic of the disease is impaired skin barrier function [12]. Current recommendation is that AE patients should apply their emollients generously and frequently in order to maintain the hydration of the stratum corneum [13]. Nevertheless, patients often do not follow these daily regimes and some may only use emollients once or twice daily to fit around busy daily routines [14]. The dosage regimen in this study, twice daily, was therefore chosen to enable comparison of the two products when used under conditions mimicking the generally low compliance among eczema sufferers.
This study provides clear evidence of the superiority of DELP gel over ZBC cream in increasing skin hydration (as measured by change from baseline corneometry measurements) over 5 days of twice-daily application. The cumulative increase in skin hydration for DELP gel was approximately 10 times that seen for ZBC. In contrast, after 5 days of treatment, the cumulative increase in skin hydration for ZBC was not statistically different from zero.
The long-lasting nature of the skin moisturisation achieved by DELP was also clearly demonstrated by the statistically significant change from baseline corneometry measurements from day 2 to day 5 (Fig. 2), which were taken between 9 and 13 h after the most recent application of the product.
These results also show that washing, followed by reapplication of DELP gel in the evening, resulted in morning measurements on days 3 and 5 that were similar to those observed on days 2 and 4 when no washing occurred (and patients reapplied the product) the night before. This suggests that the moisturising effect of DELP is resistant to washing. This effect is consistent with DELP’s formulation which is designed to break down irreversibly in contact with skin electrolytes (salt), thereby depositing the oily ingredients and rendering them less easily re-emulsified and removed by washing.
The significantly greater hydration performance of DELP over ZBC may be attributed to a higher oil content of DELP compared to ZBC (30% vs. 21% as declared by the manufacturers) and to their differing substantivities on the skin [15]. In addition, DELP contains high levels of glycerol, which is a humectant and has the ability to bind and retain water within the entire thickness of the stratum corneum [16,17,18]. Fluhr et al. [17] have shown faster barrier repair, measured using transepidermal water loss (TEWL), and increased hydration in glycerol-treated sites in comparison to untreated controls. These researchers concluded that glycerol accelerates recovery of skin barrier function in vivo. Similarly, humectants are also reported to compensate for reduced levels of natural moisturising factors, which are required to maintain the skin’s plasticity and prevent corneocyte dehydration. If not addressed, this leads to the development of cracks between the corneocytes, resulting in inflammation and pruritus [18]. Povidone is another possible contributing factor because, when the formulation breaks down in contact with the skin, this forms a film to help improve both the formulation’s barrier properties on the skin and the water-holding capacity of the gel [13, 19, 20].
In this study, subjects applied, on average, 22% more DELP than ZBC, but the reason for this difference is unclear. It could be due to the nature of the products themselves or patient preference.
Prescribers tend to recommend emollients based primarily on patient/consumer preference and cost, and the cosmetic acceptability of emollients is very important because patients are unlikely to use formulations with poor cosmetic appeal, resulting in no clinical benefit [12]. In this blinded study, patients generally found both products to be acceptable. The physical characteristics of DELP were rated more favourably than ZBC for all three parameters (acceptability, willingness to use again and product preference).
Finally, in relation to safety, patients reported a total of 161 applications of each product during the study, with no adverse reactions deemed to be related to the study products.
Although corneometry is a well-established measure of skin hydration, which is itself a universally accepted therapeutic aim in the management of dry skin conditions such as AE, a possible limitation of this study is that it may be regarded as a surrogate clinical end point. Similar criticisms may also apply to TEWL measurements. Future studies of this sort should ideally include clinical endpoints, albeit with the attendant limitations of cost and practicality.
Conclusions
The results of this study provide strong evidence that DELP is a well-tolerated, effective and long-lasting product that increased skin hydration levels—estimated to be approximately ten times that seen with ZBC. DELP is therefore especially suitable for use by patients who, for whatever reason, can only re-apply their emollient treatment as infrequently as twice daily. These results also confirm that emollients are not equally effective skin moisturisers [19], and this is something that healthcare professionals should be aware of when prescribing these products.
References
Williams H, Stewart A, von Mutius E, Cookson W, Anderson HR. Is eczema really on the increase worldwide? J Allergy Clin Immunol. 2008;121(4):947–54.
Kownacki S. The importance of emollients in treating the increasing incidence of atopic eczema. Nurs Times. 2009;105:28.
Clark C. How to chose a suitable emollient? Pharm J. 2004;273:351–3.
Cork MJ, Danby S. Skin barrier breakdown: a renaissance in emollient therapy. Br J Nurs. 2009;18(14):872, 874, 876–7.
NICE. Management of atopic eczema in children from birth up to the age of 12 years. National Institute for Health and Clinical Excellence. 2007;Clinical guidelines, CG57.
Simpson EL. Atopic dermatitis prevention. Dermatol Ther. 2006;19(2):108–17.
MeRec. The use of emollients in dry skin conditions. MeReC Bull. 1998;9(12):45.
Lewis-Jones S. Dry skin in childhood and ther misery of eczema and its treatments. In: Loden M, Maibach H, editors. Treatment of dry skin syndrome—the art and science of moisturisers. New York: Springer; 2012. p. 41–58.
Tucker R. What evidence is there for moisturisers? PJ Online. 2011:1–4.
Loden M, Hagforsen E, Lindberg M. The presence of body hair influences the measurement of skin hydration with the Corneometer. Acta Derm Venereol. 1995;75(6):449–50.
Djokic-Gallagher J, Rosher P, Walker J, Sykes K, Hart V. Emollient efficacy and acceptability in the treatment of eczematous dry skin: a double-blind, randomised comparison of two UK-marketed products. J Dermatol Treat. 2016;27(5):461–6.
Cork MJ. The importance of skin barrier function. J Dermatol Treat. 1997;8(S1):s7.
Cork MJ. The importance of complete emollient therapy. Med Matt Prim Care. 2007;142:1–8.
Hon KL, Wang S, Pong H, Leung TF. The Ideal moisturizer: A survey of parental expectations and practice in childhood-onset eczema. J Dermatol Treat. 2013;24(1):7–12.
Djokic-Gallagher J, Rosher P, Walker J, Hart V. Objective and subjective in vivo comparison of two emollient products. Clin Cosmet Investig Dermatol. 2012;5:85–91.
Okamoto T, Inoue H, Anzai S, Nakajima H. Skin-moisturizing effect of polyols and their absorption into human stratum corneum. J Cosmet Sci. 1998;49:57–8.
Fluhr JW, Gloor M, Lehmann L, Lazzerini S, Distante F, Berardesca E. Glycerol accelerates recovery of barrier function in vivo. Acta Derm Venereol. 1999;79(6):418–21.
Moncrieff G, Cork M, Lawton S, Kokiet S, Daly C, Clark C. Use of emollients in dry-skin conditions: consensus statement. Clin Exp Dermatol. 2013;38(3):231–8.
Moncrieff G. Complete Emollient therapy—a personal view. PCDS Bull. Spring 2013:9–14.
Gallagher J, Rosher P, Mohammed D, Oliveira G, Lane M. The role of the excipient povidone in an advanced gel formulation specially designed for the treatment of dry skin conditions. In: 23rd EADV Congress; Amsterdam, Netherlands 2014.
Acknowledgements
This study was sponsored by Dermal Laboratories Ltd, Hitchin, UK, and carried out by Reading Clinical Research, Reading, UK. Article processing charges were funded by Dermal Laboratories Ltd. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis. A summary of the data detailed in this paper has been presented at the 14th EADV Spring Symposium, May 2017, Brussels, Belgium.
Disclosures
Jasmina Djokic-Gallagher is a full-time employee of Dermal Laboratories Ltd, Hitchin, UK. Phil Rosher is a full-time employee of Dermal Laboratories Ltd, Hitchin, UK. Gabriela Oliveira is a full-time employee of Dermal Laboratories Ltd, Hitchin, UK. Jennine Walker is a full-time employee of Dermal Laboratories Ltd, Hitchin, UK.
Compliance with Ethics Guidelines
All procedures followed were in accordance with the ethical approval given for this study by the responsible Ethics committee and with the Helsinki Declaration of 1964, as revised in 2013. Informed consent was obtained from all patients for being included in the study.
Data Availability
The datasets during and/or analysed during the current study are available from the corresponding author on reasonable request.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/4F98F0602F92C153.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Djokic-Gallagher, J., Rosher, P., Oliveira, G. et al. A Double-Blind, Randomised Study Comparing the Skin Hydration and Acceptability of Two Emollient Products in Atopic Eczema Patients with Dry Skin. Dermatol Ther (Heidelb) 7, 397–406 (2017). https://doi.org/10.1007/s13555-017-0188-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-017-0188-z