
Abstract
Background
The survival rate of infants with gastroschisis has improved significantly. It is over 90% in developed countries, but 50% in developing countries. This study aimed to investigate the factors improving the survival rate of infants with gastroschisis in developing countries.
Methods
Neonates meeting the inclusion criteria, who presented to our center since the establishment of delivery room surgery, were enrolled into this retrospective study. Data were evaluated specifically to determine the role of delivery room surgery in reducing the mortality and morbidity of infants with gastroschisis and to identify factors optimizing the conditions of outborn infants.
Results
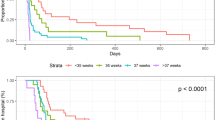
A total of 64 infants were identified. The overall survival rate of the infants was 60.9%. The survival rate of infants in inborns was 76.5%, and the survival rate of infants in outborns was 43.3%. Infants of the outborn group took more time to reach full enteral feeding, and were more likely to require a prolonged stay in hospital when compared with those of the inborn group. Logistic analysis identified that the surgical technique, the presence of sepsis and intestinal necrosis could be expected to influence the outcome of gastroschisis.
Conclusions
The strategy of delivery of patients in a center prepared to perform delivery room closure of gastroschisis appears to improve the survival of patients with gastroschisis. Further reduction in mortality rates will depend on improved conditions of outborn infants.
Article PDF
Similar content being viewed by others


References
Holland AJ, Walker K, Badawi N. Gastroschisis: an update. Pediatr Surg Int 2010;26:871–878.
Knutrud O, Bjordal RI, Rø J, Bø G. Gastroschisis and omphalocele. Prog Pediatr Surg 1979;13:51–61.
Nembhard WN, Waller DK, Sever LE, Canfield MA. Patterns of first-year survival among infants with selected congenital anomalies in Texas, 1995–1997. Teratology 2001;64:267–275.
Sekabira J, Hadley GP. Gastroschisis: a third world perspective. Pediatr Surg Int 2009;25:327–329.
Coughlin JP, Drucker DE, Jewell MR, Evans MJ, Klein MD. Delivery room repair of gastroschisis. Surgery 1993;114:822–826.
Cowan KN, Puligandla PS, Laberge JM, Skarsgard ED, Bouchard S, Yanchar N, et al. The gastroschisis prognostic score: reliable outcome prediction in gastroschisis. J Pediatr Surg 2012;47:1111–1117.
Olieman JF, Poley MJ, Gischler SJ, Penning C, Escher JC, van den Hoonaard TL, et al. Interdisciplinary management of infantile short bowel syndrome: resource consumption, growth, and nutrition. J Pediatr Surg 2010;45:490–498.
Jager LC, Heij HA. Factors determining outcome in gastroschisis: clinical experience over 18 years. Pediatr Surg Int 2007;23:731–736.
Payne NR, Pfleghaar K, Assel B, Johnson A, Rich RH. Predicting the outcome of newborns with gastroschisis. J Pediatr Surg 2009;44:918–923.
Banyard D, Ramones T, Phillips SE, Leys CM, Rauth T, Yang EY. Method to our madness: an 18-year retrospective analysis on gastroschisis closure. J Pediatr Surg 2010;45:579–584.
Hadley GP, Mars M. Improving neonatal transport in the third world-technology or teaching? S Afr J Surg 2001;39:122–124.
Pastor AC, Phillips JD, Fenton SJ, Meyers RL, Lamm AW, Raval MV, et al. Routine use of a SILASTIC spring-loaded silo for infants with gastroschisis: a multicenter randomized controlled trial. J Pediatr Surg 2008;43:1807–1812.
Kidd JN Jr, Jackson RJ, Smith SD. Evolution of staged versus primary closure of gastroschisis. Ann Surg 2003;237:759–765.
Eggink BH, Richardson CJ, Malloy MH, Angel CA. Outcome of gastroschisis: a 20-year case review of infants with gastroschisis born in Galveston, Texas. J Pediatr Surg 2006;41:1103–1108.
McNamara WF, Hartin CW, Escobar MA, Lee YH. Outcome differences between gastroschisis repair methods. J Surg Res 2011;165:19–24.
Gelas T, Gorduza D, Devonec S, Gaucherand P, Downham E, Claris O, et al. Scheduled preterm delivery for gastroschisis improves postoperative outcome. Pediatr Surg Int 2008;24:1023–1029.
Ergün O, Barksdale E, Ergün FS, Prosen T, Qureshi FG, Reblock KR, et al. The timing of delivery of infants with gastroschisis influences outcome. J Pediatr Surg 2005;40:424–428.
Hadidi A, Subotic U, Goeppl M, Waag KL. Early elective cesarean delivery before 36 weeks vs late spontaneous delivery in infants with gastroschisis. J Pediatr Surg 2008;43:1342–1346.
Chen IL, Lee SY, Ou-Yang MC, Chao PH, Liu CA, Chen FS, et al. Clinical presentation of children with gastroschisis and small for gestational age. Pediatr Neonatol 2011;52;219–222.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Du, L., Pan, WH., Cai, W. et al. Delivery room surgery: an applicable therapeutic strategy for gastroschisis in developing countries. World J Pediatr 10, 69–73 (2014). https://doi.org/10.1007/s12519-014-0455-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12519-014-0455-3