
Abstract
Depending on the stage of the disease, autopsy findings of COVID-19 may include a spectrum of cardiopulmonary pathologies including alveolar hyaline membrane formation, vascular thrombosis, and intracardiac thrombi. Identification of a COVID-19 positive decedent in the absence of clinical history relies primarily on post-mortem nasopharyngeal (NP) or oropharyngeal (OP) swabs for real time polymerase chain reaction (RT-PCR). In the absence of definitive microbiology testing, post-mortem computed tomography (PMCT) may be a powerful adjunct tool for screening. Persistence of pathological changes may prolong physiological alterations and increase the risk of cardiopulmonary compromise. This current case outlines the forensic presentation, utilization of screening tools including PMCT, and the autopsy findings of a recent toxicology related sudden death case in the context of severe sequelae of COVID-19 pneumonia. This case demonstrates the limitation of NP and OP swabs in the post-mortem setting, the value of PMCT as an adjunct screening tool, and raises the consideration of COVID-19 sequelae as a potential contributing risk factors in sudden death cases in the community.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The novel human coronavirus (COVID-19) pandemic poses a major public health challenge globally. COVID-19 transmissions are primarily through the respiratory system via droplets or contact with secretions [1], and hospital autopsy pathology has been crucial in elucidating the clinical course and anatomical sequelae of the disease to guide management [2]. Sudden deaths in the community due to COVID-19 infections have also been a major concern given the rapid spread of the virus among vulnerable populations, particularly the residents of long-term care homes or those with history of opioid abuse [3, 4]. Pathological findings of COVID-19 in the community could present on a spectrum of severity compared to pathologies described in hospital cases [1, 5], and documenting decedents’ comorbidities may shed light on how COVID-19 infection interact with existing conditions. Therefore, post-mortem forensic investigation plays an integral role in expanding pathological knowledge of COVID-19 and understanding its community health impacts.
In sudden death investigations, decedents are of various age, sex, health status, and socioeconomic backgrounds, and forensic pathologists are uniquely positioned to document the broad spectrum of COVID-19 presentations from the community at large. However, with limited records and histories, working with potentially infectious cases presents a health and safety risk for autopsy personnel. At our institution, suspicion of COVID-19 infection during necropsies would prompt post-mortem swabs for quantitative real time PCR (RT-PCR). Post-mortem swabs are minimally invasive and easy to perform, but false negative results have been reported despite convincing pathological findings of COVID-19 during autopsy [5]. Post-mortem RT-PCR has a reported sensitivity of 96.8% within 1 week of death [6], however post-mortem computed tomography (PMCT) may be a helpful alternative should swab results be inconclusive or incompatible [7].
In this case report, we describe findings of advanced and persistent sequelae of COVID-19 pneumonia in a decedent with history of COVID-19 infection and substance use. In addition, we demonstrate the utility of PMCT when approaching a suspicious but swab negative case. Finally, we explore how sustained pathophysiologic changes of COVID-19 may increase the risk of sudden death.
Case description
A 51-year-old man was found deceased in the stairwell of a parking garage with drug paraphernalia. Twenty days prior he had tested positive for COVID-19 and required hospital admission due to decreased level of consciousness. The hospital toxicology report at the time was notable for benzodiazepines, cocaine, and amphetamines. He subsequently recovered and was discharged from the hospital.
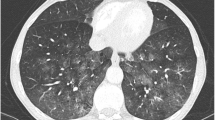
Given his prior COVID-19 history, per institutional protocol post-mortem nasopharyngeal (NP) and oropharyngeal (OP) swabs were performed which were negative for COVID-19. However, post-mortem computed tomography (PMCT) demonstrated diffuse ground glass opacities and interstitial markings involving all lobes (Fig. 1) compatible with COVID-19 pneumonia.

Post-mortem CT scan of the chest revealed ground glass opacities of the lung parenchyma involving all 5 lobes. Prominent interstitial markings were present and diffuse. These findings were compatible with COVID-19 pneumonia
A medicolegal autopsy was performed. The external examination documented an Asian male, whose appearance correlated to the reported age of 51 years. There were no external injuries. A limited evisceration for the chest bloc and targeted organ examination was performed as per the institutional safety protocol for suspected COVID-19 cases. Standard toxicological samples were collected, including heart and femoral bloods, and a urine specimen. On macroscopic examination the lungs were heavy with the right lung weighing 1340 g and the left lung weighing 940 g. On sectioning, the lungs showed bilateral consolidation involving all lobes. There were no grossly evident pulmonary emboli. The heart weight was within normal limits (410 g), and incidentally there was an adherent thrombus occupying the right ventricle. On microscopic examination, the lungs showed features of diffuse alveolar damage (DAD) characterized by organizing pneumonia with hyaline membrane formation, and reactive type 2 pneumocytes (Fig. 2). Organized thrombus of the right ventricle was confirmed on histology, along with evidence of scattered thrombosis within the pulmonary vasculature (Fig. 3). The remainder of the autopsy findings included moderate coronary artery disease, and passive venous congestion of the liver with chronic hepatitis.

Histological sections of from the consolidated lung parenchyma. Routine haematoxylin and eosin section a reveals type 2 pneumocyte hyperplasia and interstitial inflammation. Trichome staining b confirms the presence of hyaline membrane formation compatible with organizing pneumonia

Haematoxylin and eosin section form the right ventricle a shows adherent organizing thrombus. Additional thrombi were present in sampled the lung parenchyma b, however macroscopic pulmonary emboli were not evident
Toxicology results from femoral blood revealed significant fentanyl levels above laboratory fatal reference levels (> 3 ng/mL) at 15 ng/mL, and N-desalkylflurazepam, an active metabolite of benzodiazepine, at 0.014 mg/L. Benzodiazepine could synergistically potentiate effects of opioids through central nervous system and respiratory depression, thereby increasing the risk of fatal opioid overdose. However, the blood fentanyl quantity was several times above the fatal levels in this decedent who also had evidence of extensive DAD and thrombosis, therefore the cause of death was primarily attributed to fentanyl toxicity with contributing complications of COVID-19 pneumonia.
Discussion
In this case report, findings of persistent cardiorespiratory complications were evident in a decedent with prior history of COVID-19 infection and fatal fentanyl toxicity. Macroscopic and microscopic examination of the lung tissue demonstrated extensive lobar consolidation with organizing hyaline membrane formation, and presence of thrombi. These findings are consistent with previously reported spectrum of autopsy findings in COVID-19 pneumonia [2, 5, 8]. Active COVID-19 infection is also associated with increased risk of venous thromboembolic events with one report noting the incidence of pulmonary embolism to be up to 24% [9, 10]. In this case report, we also note the presence of a right intraventricular thrombosis in addition to findings of pulmonary thrombosis. Intracardiac thrombi are an uncommon cardiac complication of COVID-19 with reported prevalence of 2.5% at autopsy [11]. Formation of ventricular thrombus may be attributed to endotheliitis due to direct viral effects of COVID-19, however specific histological findings of endotheliitis are controversial [11]. Clinically intracardiac thrombi are diagnosed with transthoracic echocardiogram (TTE), and timely resolution of thrombosis require anticoagulation therapy [12, 13]. In this case, the timeline of the right ventricular thrombus formation is unclear as the decedent did not have documented antemortem cardiac imaging or history of anticoagulation therapy. Nonetheless, presence of right ventricular thrombus may serve as a source of microscopic emboli to the lungs, thereby increase the risk of extensive pulmonary thromboembolism.
Post-mortem NP swabs with RT-PCR are utilized to rule out COVID-19 in the autopsy setting to aid in risk reduction for staff during necropsies. Nasopharyngeal swabs are pursued in suspected COVID-19 cases due to higher viral load within the nasal fossa during acute phase of the infection [14]. In this case both OP and NP swabs were utilized 20 days after initial antemortem swab positivity. Evidence from the literature suggests that positive detection of COVID-19 by RT-PCR in the post-mortem period may vary with anatomical location of sample collection, therefore multiple swabs from the upper respiratory tract was recommended [15]. Negative Post-mortem RT-PCR results may be attributed to sampling error, remitting infection with low viral load, and involvement of lower respiratory tracts with elapsed time since initial diagnosis [14, 15]. A lower respiratory tissue sample was not pursued in this case as the decedent had a confirmed antemortem COVID-19 diagnosis, and routine use of PMCT was performed as per institutional protocol. False negative RT-PCR results have been reported in the literature and use of computed tomography imaging may be more sensitive in suspected cases [16,17,18,19]. In the absence of microbiology confirmation, CT imaging may be a powerful adjunct screening tool. Consistent radiological findings of COVID-19 pneumonia were previously demonstrated in a case series utilizing PMCT at our institution which highlighted the potential for COVID-19 screening using PMCT [7]. Unlike in clinical settings, routine use of PMCT for screening purposes would not be limited by the potential radiation related risks, though interpretation of PMCT would require adequate knowledge of common post-mortem artefacts. Additionally, PMCT allows the pathologist to plan appropriate dissection approach to target pathological findings. In suspected infectious cases, such as COVID-19, PMCT may allow the pathologist to do limited approaches to minimize pathogen exposure. Despite the utility of PMCT, definitive diagnosis of COVID-19 as cause of death would require a combination of clinical, microbiological, and pathological findings. In our case, we reaffirm the potential of PMCT for screening in a case of double negative COVID-19 swabs, which allowed for targeted and safe autopsy.
The autopsy findings also raise some additional considerations in sudden death investigation. Namely elucidating cause of death in individuals with prior history of COVID-19 infection and role of persistent cardiorespiratory pathologies. In this decedent, a toxic level of fentanyl was detected which in isolation could be sufficient for cause of death. However, elucidating a cause of death may be more challenging in an alternative scenario where sub-toxic levels of substances were detected or other competing natural conditions such as heart diseases. The concurrent DAD features and vascular thrombi may suggest that individuals recovering from COVID-19 may have lower cardiorespiratory reserve thresholds and therefore be more vulnerable to additional stressors, including non-toxic levels of respiratory depressant drugs. In this decedent he potentially had multiple pathologies that may contribute to poorer cardiopulmonary outcomes. First, the decedent may have decreased respiratory capacity due to diffusely edematous lungs as evidenced by histological findings of DAD. Second, residual venous thromboembolism may result in ventilation perfusion mismatch, which in turn increases the risk of respiratory failure. Finally, the presence of intracardiac thrombus may precipitate further thrombi formation, right heart failure, or increased risk of arrhythmic events with hemodynamic instability [13, 20]. Persistent sequelae of COVID-19 pneumonia may pose a sustained risk factor for sudden death in individuals recovering from acute phase of the disease. Autopsy pathologists should therefore be aware of macroscopic, CT and microscopic findings of COVID-19 in different stages. Now with the majority of the population becoming vaccinated in some countries, atypical presentations can present with other disease pathology or deaths due to substance abuse.
In summary, this report documents persistent COVID-19 features in a decedent with prior infection confirmed on antemortem testing. Post-mortem NP and OP swabs were negative, however use of PMCT demonstrated diffuse opacities of both lungs, in keeping with COVID-19 pneumonia. PMCT is a powerful non-invasive screening tool which enable safe practices in a potentially infectious cases and allows pathologists to alter dissection approaches as appropriate. Targeted autopsy revealed DAD, venous thrombosis, and intracardiac thrombus at 20 days after antemortem confirmatory testing. In this case, cause of death was attributed to toxic levels of fentanyl, however the potential hazardous effects of persistent COVID-19 pathologies should be considered as a contributing factor especially in individuals with competing explanations for cause of death.
Key points:
-
1.
We report advance thrombosis of the right atrium in addition to other autopsy features of COVID-19 which include diffuse organizing pneumonia and extensive pulmonary thrombosis.
-
2.
Use of post-mortem computational tomography may help identify severe sequela of COVID-19 in the setting of a negative post-mortem nasopharyngeal swab.
-
3.
Persistent pathological changes of COVID-19 pneumonia as a contributing risk factor in sudden death should be considered when determining a cause of death.
References
Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N Engl J Med. 2020;383:1199–207.
Borczuk AC, Salvatore SP, Seshan SV, et al. COVID-19 pulmonary pathology: a multi-institutional autopsy cohort from Italy and New York City. Mod Pathol. 2020;33:2156–68.
Fisman DN, Bogoch I, Lapointe-Shaw L, McCready J, Tuite AR. Risk factors associated with mortality among residents with coronavirus disease 2019 (COVID-19) in long-term care facilities in Ontario, Canada. JAMA Netw Open. 2020;3:e2015957.
Linas BP, Savinkina A, Barbosa C, et al. A clash of epidemics: Impact of the COVID-19 pandemic response on opioid overdose. J Subst Abuse Treat. 2021;120:108158.
Youd E, Moore L. COVID-19 autopsy in people who died in community settings: the first series. J Clin Pathol. 2020;73:840–4.
Hall JA, Harris RJ, Emmett HE, et al. On the sensitivity and specificity of post-mortem upper respiratory tract testing for SARS-CoV-2. J Infect Dis. 2021;224:389–94.
Williams AS, Dmetrichuk JM, Kim P, Pollanen MS. Postmortem radiologic and pathologic findings in COVID-19: The Toronto experience with pre-hospitalization deaths in the community. Forensic Sci Int. 2021;322:110755.
Buja LM, Wolf DA, Zhao B, et al. The emerging spectrum of cardiopulmonary pathology of the coronavirus disease 2019 (COVID-19): report of 3 autopsies from Houston, Texas, and review of autopsy findings from other United States cities. Cardiovasc Pathol. 2020;48:107233.
Long B, Brady WJ, Koyfman A, Gottlieb M. Cardiovascular complications in COVID-19. Am J Emerg Med. 2020;38:1504–7.
Bompard F, Monnier H, Saab I, et al. Pulmonary embolism in patients with COVID-19 pneumonia. Eur Respir J. 2020;56:2001365.
Roshdy A, Zaher S, Fayed H, Coghlan JG. COVID-19 and the heart: a systematic review of cardiac autopsies. Front Cardiovasc Med. 2020;7:626975.
Calvi E, Bernardi N, Cimino G, et al. Unusual intracardiac thrombosis in two patients with coronavirus disease 2019 (COVID-19): case series. Eur Heart J Case Rep. 2021;5:ytaa518.
Merlo E, Grutta G, Tiberio I, Martelli G. Right heart thrombus in an adult COVID-19 patient: A case report. J Crit Care Med. 2020;6:237–42.
Fernández-Rodríguez A, Casas I, Culebras E, Morilla E, Cohen MC, Alberola J. COVID-19 and post-mortem microbiological studies. Span J Leg Med. 2020;46:127–38.
Dell’Aquila M, Cattani P, Fantoni M, et al. Postmortem swabs in the severe acute respiratory syndrome coronavirus 2 pandemic: report on 12 complete clinical autopsy cases. Arch Pathol Lab Med. 2020;144:1298–302.
Feng H, Liu Y, Lv M, Zhong J. A case report of COVID-19 with false negative RT-PCR test: necessity of chest CT. Jpn J Radiol. 2020;38:409–10.
Winichakoon P, Chaiwarith R, Liwsrisakun C, et al. Negative nasopharyngeal and oropharyngeal swabs do not rule out COVID-19. J clinical microbiology. 2020;58:e00297-e320.
Quaia E, Baratella E, Crimi F, Cancian L, Crivelli P, Vianello A. High-resolution CT features in patients with COVID-19 pneumonia and negative nasopharyngeal and oropharyngeal swabs. Pulmonology. 2021;27:351–3.
Fang Y, Zhang H, Xie J, et al. Sensitivity of chest CT for COVID-19: comparison to RT-PCR. Radiology. 2020;296:E115–7.
Ullah W, Saeed R, Sarwar U, Patel R, Fischman DL. COVID-19 complicated by acute pulmonary embolism and right-sided heart failure. JACC: Case Rep. 2020;2:1379–82.
Author information
Authors and Affiliations
Contributions
All authors contributed to the case report conception and design. Relevant information was collected by Jayantha C Herath. The first draft and the revised manuscript was written by Youheng Xie. All authors provided response to reviewers and commented on previous versions of the manuscript. All authors read and approved the final version.
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Xie, Y., Herath, J.C. A case of persistent severe sequelae of COVID-19 infection: potential role in sudden death?. Forensic Sci Med Pathol 18, 69–73 (2022). https://doi.org/10.1007/s12024-021-00435-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12024-021-00435-4