
Abstract
Introduction
Bariatric surgery is the most effective therapy for weight loss in patients with morbid obesity. One of the most common long-term complications includes cholelithiasis. There is not a clear consensus in how to treat an asymptomatic gallbladder disease before and after bariatric surgery.
Methods
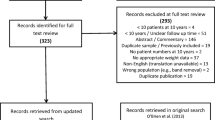
Prospective study with every patient submitted to bariatric surgery from 2012 to 2014. The gallbladder status was assessed with an ultrasound before and after surgery (12 months), and a conservative management was conducted for patients with asymptomatic disease (preoperative and de novo); the need for delayed cholecystectomy was reported. Secondarily, an analysis of weight loss (%EWL) and gallbladder status was performed.
Results
Two-hundred and two bariatric surgeries were performed. The global incidence of preoperative gallbladder disease was 34.3 %, with 14.2 % presenting sludge, 20.1 % asymptomatic gallstones, and 2.3 % symptomatic gallstones. The final analysis was based on 146 patients; female sex comprised 81.1 % of cases with a mean age of 38.5 years. After 12 months, de novo gallbladder disease was observed in 21.2 %. The overall rate of cholecystectomy because of symptomatic disease after 12 months was 3.4 % (2 % developed acute cholecystitis). There were no differences in %EWL between patients with de novo gallbladder disease and those without.
Conclusion
Conservative management of asymptomatic gallbladder disease in candidates to bariatric surgery is safe and can be offered in every case, based on the low percentage of patients requiring further cholecystectomy after 12 months. Also, a conservative management can be offered to patients developing de novo sludge/cholelithiasis without related symptoms.


Similar content being viewed by others


References
Angrisani L, Santonicola A, Iovino P, et al. Bariatric surgery worldwide 2013. Obes Surg. 2015;25:1822–32.
Bozkurt S. Complications in bariatric surgery. Eur J Endosc Laparosc Surg. 2014;1:238–46.
Fobi M, Lee H, Igwe D, et al. Prophylactic cholecystectomy with gastric bypass operation: incidence of gallbladder disease. Obes Surg. 2002;12:350–3.
Jonas E, Marsk R, Rasmussen F, Freedman J. Incidence of postoperative gallstone disease after antiobesity surgery: population-based study from Sweden. Surg Obes Relat Dis. 2010;6:54–8.
Dittrick GW, Thompson JS, Campos D, et al. Gallbladder pathology in morbid obesity. Obes Surg. 2005;15:238–42.
Worni M, Guller U, Shah A, et al. Cholecystectomy concomitant with laparoscopic gastric bypass: a trend analysis of the nationwide inpatient sample from 2001 to 2008. Obes Surg. 2012;22:220–9.
Shiffman ML, Sugerman HJ, Kellum JM, Moore EW. Changes in gallbladder bile composition following gallstone formation and weight reduction. Gastroenterology. 1992;103:214–21.
Liddle RA, Goldstein RB, Saxton J. Gallstone formation during weight-reduction dieting. Arch Intern Med. 1989;149:1750–3.
de Oliveira C IB, Adami Chaim E, da Silva BB. Impact of rapid weight reduction on risk of cholelithiasis after bariatric surgery. Obes Surg. 2003;13:625–8.
Villegas L, Schneider B, Provost D, et al. Is routine cholecystectomy required during laparoscopic gastric bypass? Obes Surg. 2004;14:206–11.
Mason EE, Renquist KE. Gallbladder management in obesity surgery. Obes Surg. 2002;12:222–9.
Quesada BM, Kohan G, Roff HE, et al. Management of gallstones and gallbladder disease in patients undergoing gastric bypass. World J Gastroenterol. 2010;16:2075–9.
Amstutz S, Michel JM, Kopp S, Egger B. Potential benefits of prophylactic cholecystectomy in patients undergoing bariatric bypass surgery. Obes Surg. 2015;25:2054–60.
Tarantino I, Warschkow R, Steffen T, et al. Is routine cholecystectomy justified in severely obese patients undergoing a laparoscopic Roux-en-Y gastric bypass procedure? A comparative cohort study. Obes Surg. 2011;21:1870–8.
Tucker ON, Fajnwaks P, Szomstein S, Rosenthal RJ. Is concomitant cholecystectomy necessary in obese patients undergoing laparoscopic gastric bypass surgery? Surg Endosc. 2008;22:2450–4.
Weiss AC, Inui T, Parina R, et al. Concomitant cholecystectomy should be routinely performed with laparoscopic Roux-en-Y gastric bypass. Surg Endosc. 2015;29:3106–11.
Liem RK, Niloff PH. Prophylactic cholecystectomy with open gastric bypass operation. Obes Surg. 2004;14:763–5.
Nougou A, Suter M. Almost routine prophylactic cholecystectomy during laparoscopic gastric bypass is safe. Obes Surg. 2008;18:535–9.
D'Hondt M, Sergeant G, Deylgat B, et al. Prophylactic cholecystectomy, a mandatory step in morbidly obese patients undergoing laparoscopic Roux-en-Y gastric bypass? J Gastrointest Surg. 2011;15:1532–6.
Warschkow R, Tarantino I, Ukegjini K, et al. Concomitant cholecystectomy during laparoscopic Roux-en-Y gastric bypass in obese patients is not justified: a meta-analysis. Obes Surg. 2013;23:397–407.
Raziel A, Sakran N, Szold A, Goitein D. Concomitant cholecystectomy during laparoscopic sleeve gastrectomy. Surg Endosc. 2015;29:2789–93.
Uy MC, Talingdan-Te MC, Espinosa WZ, et al. Ursodeoxycholic acid in the prevention of gallstone formation after bariatric surgery: a meta-analysis. Obes Surg. 2008;18:1532–8.
Adams LB, Chang C, Pope J, et al. Randomized, prospective comparison of ursodeoxycholic acid for the prevention of gallstones after sleeve gastrectomy. Obes Surg. 2015;26(5):990–4.
Miller K, Hell E, Lang B, Lengauer E. Gallstone formation prophylaxis after gastric restrictive procedures for weight loss: a randomized double-blind placebo-controlled trial. Ann Surg. 2003;238:697–702.
Karadeniz M, Gorgun M, Kara C. The evaluation of gallstone formation in patients undergoing Roux-en-Y gastric bypass due to morbid obesity. Ulus Cerrahi Derg. 2014;30:76–9.
Mechanick JI, Youdim A, Jones DB, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient—2013 update: cosponsored by American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery. Obesity (Silver Spring). 2013;21(Suppl 1):S1–27.
Stokes CS, Gluud LL, Casper M, Lammert F. Ursodeoxycholic acid and diets higher in fat prevent gallbladder stones during weight loss: a meta-analysis of randomized controlled trials. Clin Gastroenterol Hepatol. 2014;12:1090–1100 e1092 .quiz e1061
Hempfling W, Dilger K, Beuers U. Systematic review: ursodeoxycholic acid—adverse effects and drug interactions. Aliment Pharmacol Ther. 2003;18:963–72.
Portenier DD, Grant JP, Blackwood HS, et al. Expectant management of the asymptomatic gallbladder at Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2007;3:476–9.
Lopes TL, Clements RH, Wilcox CM. Laparoscopy-assisted ERCP: experience of a high-volume bariatric surgery center (with video). Gastrointest Endosc. 2009;70:1254–9.
Li VK, Pulido N, Fajnwaks P, et al. Predictors of gallstone formation after bariatric surgery: a multivariate analysis of risk factors comparing gastric bypass, gastric banding, and sleeve gastrectomy. Surg Endosc. 2009;23:1640–4.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institution and/or national research committee and with 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained for all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Pineda, O., Maydón, H.G., Amado, M. et al. A Prospective Study of the Conservative Management of Asymptomatic Preoperative and Postoperative Gallbladder Disease in Bariatric Surgery. OBES SURG 27, 148–153 (2017). https://doi.org/10.1007/s11695-016-2264-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-016-2264-3