
Abstract
Background
Statistical models and scores have been recently suggested to predict remission of type 2 diabetes after bypass surgery, but their relevance in routine clinical practice still needs evaluation. Our objective was to assess these methods on a French cohort and to compare them with other easy-to-use models.
Methods
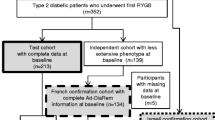
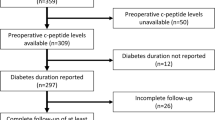
We investigated a cohort of 84 diabetic obese subjects who underwent Roux-en-Y gastric bypass surgery. Diabetes remission 1 year after surgery was defined based on the American Diabetes Association criteria. We tested six methods from the literature and four other models to predict remission of diabetes after bypass surgery using pre-operative bioclinical parameters. Predictive methods for diabetes remission were assessed using cross-validation error rates when appropriate.
Results
Sixty percent of the subjects had diabetes remission. Models from the literature had high error rates in our cohort (from 22.6 to 40.5 %), while published simple scoring systems behaved much better (15.9 and 16.7 %). Using other apprehensible models learned on our cohort did not improve the prediction error (from 17.2 to 19.9 %).
Conclusions
We showed that the scoring system DiaRem is easy to use and provides the best prediction error (15.9 %) compared to other methods. We additionally propose a DiaRem score threshold of ≤6 for likely remission of a subject 1 year after surgery, which may be considered in clinical decision-making.
Similar content being viewed by others

References
Ferchak CV, Meneghini LF. Obesity, bariatric surgery and type 2 diabetes--a systematic review. Diabetes Metab Res Rev. 2004;20:438–45.
Mingrone G, Panunzi S, De Gaetano A, Guidone C, Iaconelli A, Leccesi L, et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med. 2012;366:1577–85.
Buchwald H. The evolution of metabolic/bariatric surgery. Obes Surg. 2014;1–10.
Pories WJ, Swanson MS, MacDonald KG, Long SB, Morris PG, Brown BM, et al. Who would have thought it? An operation proves to be the most effective therapy for adult-onset diabetes mellitus. Ann Surg. 1995;222:339–50. discussion 350–352.
Davies SW, Efird JT, Guidry CA, Penn RI, Sawyer RG, Schirmer BD, et al. Long-term diabetic response to gastric bypass. J Surg Res. 2014;190(2):498–503.
Pournaras DJ, Aasheim ET, Søvik TT, Andrews R, Mahon D, Welbourn R, et al. Effect of the definition of type II diabetes remission in the evaluation of bariatric surgery for metabolic disorders. Br J Surg. 2012;99:100–3.
Adams ST, Salhab M, Hussain ZI, Miller GV, Leveson SH. Preoperatively determinable factors predictive of diabetes mellitus remission following Roux-en-Y gastric bypass: a review of the literature. Acta Diabetol. 2013;50:475–8.
Wang G-F, Yan Y-X, Xu N, Yin D, Hui Y, Zhang J-P, et al. Predictive factors of type 2 diabetes mellitus remission following bariatric surgery: a meta-analysis. Obes Surg. 2014.
Hayes MT, Hunt LA, Foo J, Tychinskaya Y, Stubbs RS. A model for predicting the resolution of type 2 diabetes in severely obese subjects following Roux-en Y gastric bypass surgery. Obes Surg. 2011;21:910–6.
Dixon JB, Chuang L-M, Chong K, Chen S-C, Lambert GW, Straznicky NE, et al. Predicting the glycemic response to gastric bypass surgery in patients with type 2 diabetes. Diabetes Care. 2013;36:20–6.
Lee W-J, Hur KY, Lakadawala M, Kasama K, Wong SKH, Chen S-C, et al. Predicting success of metabolic surgery: age, body mass index, C-peptide, and duration score. Surg Obes Relat Dis. 2013;9:379–84.
Still CD, Wood GC, Benotti P, Petrick AT, Gabrielsen J, Strodel WE, et al. Preoperative prediction of type 2 diabetes remission after Roux-en-Y gastric bypass surgery: a retrospective cohort study. The Lancet Diabetes & Endocrinology. 2014;2:38–45.
Ramos-Levi AM, Matia P, Cabrerizo L, Barabash A, Sanchez-Pernaute A, Calle-Pascual AL, et al. Statistical models to predict type 2 diabetes remission after bariatric surgery. J Diabetes. 2014;6(5):472–7.
Tibshirani R. Regression shrinkage and selection via the lasso. J R Stat Soc Ser B. 1996;58:267–88.
Zou H, Hastie T. Regularization and variable selection via the elastic Net. J R Stat Soc Ser B. 2005;67:301–20.
Buse JB, Caprio S, Cefalu WT, Ceriello A, Prato SD, Inzucchi SE, et al. How do we define cure of diabetes? Dia Care. 2009;32:2133–5.
R Core Team. R: A Language and Environment for Statistical Computing [Internet]. 2014. Disponible sur: http://www.R-project.org/
Hothorn T, Hornik K, Zeileis A. Unbiased recursive partitioning: a conditional inference framework. J Comput Graph Stat. 2006;15:651–74.
Friedman J, Hastie T, Tibshirani R. Regularization paths for generalized linear models via coordinate descent. J Stat Softw. 2010;33:1–22.
Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Ser B Methodol. 1995;57:289–300.
Aminian A, Brethauer SA, Kashyap SR, Kirwan JP, Schauer PR. DiaRem score: external validation. Lancet Diabetes Endocrinol. 2014;2:12–3.
Acknowledgments
We thank Dr. Florence Marchelli and Valentine Lemoine, APHP, Pitié-Salpêtrière, Paris, for the constitution of the database; Rohia Alili, UPMC, INSERM UMR_S U1166, Paris, for samples preparation and logistics; and Jean-Philippe Bastard and Soraya Fellahi, Functional Unit of Inflammatory and Metabolic Bio-markers, Tenon Hospital, Paris, for the measurement of C-peptide. We also thank Guillemette Ramey, Institut Roche de Recherche et Médecine Translationnelle, Boulogne-Billancourt, and Ludovic Le Chat, Institute of Cardiometabolism and Nutrition, Paris, for management of the scientific collaboration between ICAN and Roche.
Conflict of interest
AC, CP, GD, JA, JLB, TS, and KC declare no conflict of interest.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Human and animal rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Grants or fellowships
Clinical Research Contracts/Direction of Clinical Research Assistance Publique des Hôpitaux de Paris (PHRC 02076, CRC Macrophage Infiltration in Human Adipose Tissue, FIBROTA), the National program “Investissements d’avenir” with the reference ANR-10-IAHU-05 (National Agency of Research), Fondation pour la Recherche Médicale (FRM), European Union Metacardis program (FP7). Nutriomics team received a grant from Institut Roche de Recherche en Médicine Translationnelle.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 125 kb)
Rights and permissions
About this article

Cite this article
Cotillard, A., Poitou, C., Duchâteau-Nguyen, G. et al. Type 2 Diabetes Remission After Gastric Bypass: What Is the Best Prediction Tool for Clinicians?. OBES SURG 25, 1128–1132 (2015). https://doi.org/10.1007/s11695-014-1511-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-014-1511-8