
Abstract
Objective
Fractures of the capitellum are rare injuries but are often more complex and of a greater extent than assumed from conventional radiographs. Classification is usually based on their extension in relation to the trochlea the trochlea and on the number of fragments. Information on associated injuries is limited and only reported in small case series. The aim of this retrospective study was to report on our experience with capitellar fractures and their associated injuries.
Methods
We retrospectively reviewed all patients treated for fractures of the capitellum humeri at our institute between 2005 and 2017. Fractures were classified according to the Bryan–Morrey and the Dubberley classification and analyzed for their associated injuries depending on the fracture type using the chi-squared test.
Results
A total of 27 capitellar fractures were treated at our institute between 2005 and 2017. The median age of the patients was 57 years (range, 4–78) and they were all treated operatively. Associated injuries of the elbow were found in 12 cases (ten radial head fractures, two elbow dislocations, two tears of the radial collateral ligament). The injury mechanism was known for 26 patients (four fell on their outstretched arm, 19 suffered a direct blow to their elbow, two had a traffic accident).
Conclusion
The incidence of radial head fractures is high in patients with capitellar fractures. Patients suffering a fracture of the capitellum humeri should be thoroughly examined for such associated injuries since a missed diagnosis can lead to poor outcomes.
Zusammenfassung
Ziel der Arbeit
Frakturen des Capitulum humeri sind seltene Verletzungen, die häufig eine komplexere Frakturmorphologie haben und weitreichender sind als nach konventionellen Röntgenaufnahmen zu vermuten. Die verschiedenen Klassifikationen dieser Fraktur basieren auf der Ausdehnung der Fraktur in Relation zur Trochlea humeri und der Anzahl der Fragmente. Daten über Begleitverletzungen dieser Fraktur sind in der Literatur nur begrenzt vorhanden und beschränken sich meist auf kleine Fallserien. In der vorliegenden Untersuchung berichten die Autoren über ihre Erfahrung in der Behandlung von Capitulumfrakturen und deren Begleitverletzungen.
Methoden
Für diese Untersuchung wurden alle Patienten retrospektiv erfasst, die sich zwischen 2005 und 2017 mit einer Capitulumfraktur in der Klinik der Autoren in Behandlung befanden. Die Frakturen wurden erneut nach der Bryan-Morrey und der Dubberley-Klassifikation eingeteilt. Vorhandene Begleitverletzungen wurden einbezogen. Mithilfe des Chi-Quadrat-Tests wurden Begleitverletzungen mit dem Frakturtyp korreliert.
Ergebnis
Insgesamt wurden 27 Frakturen des Capitulum humeri zwischen 2005 und 2017 mit einem Median von 57 Jahren (zwischen 4 und 78 Jahren) in der Klinik der Autoren behandelt. Bei allen Patienten erfolgte eine operative Versorgung. Begleitverletzungen wurden in 12 Fällen gefunden (10 Radiuskopffrakturen, 2 Ellenbogenluxationen, 2 Rupturen des radialen Kollateralbands). In 26 Fällen war der Unfallmechanismus erinnerlich (4 Stürze auf den ausgestreckten Arm, 19 direkte Anpralltraumata, 2 im Rahmen eines Verkehrsunfalls).
Schlussfolgerung
Die Inzidenz begleitender Frakturen des Radiuskopfes ist im Rahmen von Capitulumfrakturen hoch. Bei der Diagnose einer Capitulumfraktur sollte daher sorgfältig nach möglichen Begleitverletzungen gesucht werden, da übersehene Frakturen zu einem ungünstigeren Ergebnis führen können.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fractures of the capitellum humeri are rare injuries accounting for only 1% of all fractures and around 6% of fractures close to the elbow [15]. Hahn first described a fracture of the capitellum in 1853 [10]. Since then, several classifications have been developed for these fractures. The classifications most commonly used for capitellum fractures are the descriptive Bryan and Morrey classification (modified by McKee et al.) and the Dubberley classification [8, 13,14,15]. Another classification was proposed by Ring et al., generally focusing on coronal shear fractures of the distal humerus [19].
Today, capitellum fractures are usually treated by osteosynthesis. Single-fragment uncomminuted fractures (type I and IV according to the modified Reagan–Morrey classification) can be successfully treated using headless screws (Fig. 1), while fixation of smaller fragments can be achieved with bioabsorbable pins (type II; Fig. 2; [11, 12, 21, 22, 26]). Comminuted fractures (type III) are stabilized by applying an additional buttress plating to the fracture site [19].

a Sagittal computed tomography reconstruction of the injured elbow. Shear fracture of the capitellum (type I) with associated anterior radial head injury (arrow). b After osteosynthesis with two headless screws (in posterior–anterior direction)

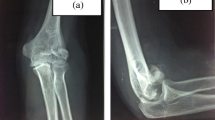
a Lateral and b anterior–posterior radiographs of the injured elbow. Capitellar fracture (type III) with associated Mason-II fracture of the radial head and tear of the lateral collateral ligament after operative treatment. The capitellar fracture was treated with bioabsorbable pins, torn ligaments were refixated using Mitek anchors, and the radial head fracture was osteosynthesized with two small-fragment screws
Capitellum fractures are often more complex than expected upon analyzing conventional radiographs [19]. Computed tomography (CT) is therefore regularly recommended in these cases so as to diagnose the extent of the fracture and to plan operative treatment.
Since capitellar fractures are rare, the data on associated injuries in fractures of the capitellum are limited to smaller studies providing clinical data of these fractures. The aim of this study was to investigate the mechanism of injury, the treatment, and the injuries associated with capitellar fractures.
Patients and methods
Patients with a partial intra-articular distal humerus fracture treated at our institute between 2005 and 2017 were identified by medical chart review. Available imaging studies, including conventional radiographs as well as CT scans, were reviewed. Patients with fractures of the capitellum were included in the study. Fractures involving the epicondyle or low-plane fractures of the distal humerus were excluded. Fractures were then selected and classified using the archived radiographs according to the modified Bryan–Morrey and the Dubberley classifications. All capitellar fractures treated at our institute with available imaging were included in this study comprising 27 patients.
Conventional radiographs, CT scans, and surgical reports were reviewed for associated lesions of the elbow joint. All patients had preoperative conventional radiographs of the elbow joint in anterior–posterior and lateral projection. For 21 patients, a preoperative CT scan was available, and for one patient an additional preoperative magnetic resonance imaging study could be reviewed. Ligamentous injuries were diagnosed intraoperatively. The frequencies of associated lesions and their distribution according to the fracture type were tested with the chi-squared test (95% confidence interval [CI]) using GraphPad Prism version 6.0c for Mac (GraphPad Software, La Jolla CA, USA).
Results
We included 16 female patients and 11 male patients with a median age of 57 years (range, 4–78). Patients reported on the mechanism of their injury in 96% of cases (all but one case). Four patients fell on their outstretched arm, 19 patients suffered a direct blow to their elbow during a fall, and in two cases the injury was associated with a traffic accident on a bicycle (Table 1).
Of the 27 fractures included in our study, 33% could be classified as a type I fracture according to the modified Bryan–Morrey classification (Table 2). The incidence of associated elbow injuries in capitellar fractures was 44% (12 cases; Table 3). Ten of the patients included in our study (37%) had an associated radial head fracture (Fig. 3). In two cases, a terrible triad injury (radial head fracture, posterior dislocation of the elbow joint, and coronoid fracture) was observed. A ligamentous injury to the radial collateral ligament was observed in two cases. The chi-squared test, used to analyze the distribution of associated lesions according to the fracture type (McKee or Dubberley), revealed no significant differences between capitellar fractures of a specific type.

Shear fracture of the capitellum (type I) with associated anterior radial head injury (same case as in Fig. 1). The arrow indicates the injury on the anterior radial head, the asterisk indicates the shear fragment of the capitellum
All patients were treated operatively: ten patients were treated with Herbert screws (five in anterior–posterior orientation, five in posterior–anterior orientation). In general, screw fixation was performed on 17 patients, while plate fixation or a combination of screws, plates, or suture anchors was necessary in ten patients. Bioabsorbable pins were used in two cases. In one patient, a comminuted fracture of the capitellum could not be reconstructed and was therefore excised. Preoperative radiographs or CT scans were available for all patients.
Of the fractures, 26 healed in a timely manner. However, in one case, a comminuted fracture (Bryan–Morrey type III) resulted in necrosis of the capitellum.
Discussion
Associated injuries occur frequently in capitellar fractures. We found injuries to the radial head in more than 37% of all capitellar fractures. Few studies exist providing clinical data of capitellar fractures. Watts et al. presented the largest number of cases [27]. They found a total of 19 radial fractures as well as two complex soft-tissue injuries (one nerve injury of the ulnar nerve in a McKee type IV fracture, one open type I fracture) in 79 partial intra-articular fractures of the distal humerus [27]. However, they could not find a correlation between the type of fracture and an associated injury. Other studies analyzing data on capitellar fractures mostly describe outcomes after specific types of osteosynthesis, such as outcomes after treatment with double-threaded screws, headless screws, cannulated screws, or bioabsorbable pins. There are only a few studies available describing the outcomes of nonoperative treatment or analyzing treatment in adolescents. In these studies, associated radial head injuries were found in up to 66% of type II capitellar fractures or 50% of type IV capitellar fractures (both according to the modified Bryan–Morrey classification; [9, 21]). Ruchelsman et al. were the first to report on the association of associated injuries in capitellum fractures with regard to outcome and specific fracture types [21]. In their cohort of 16 patients, they found five patients with associated radial head fractures. When comparing these two groups, patients with a radial head fracture had a slightly smaller arc of motion and worse functional scores (American Shoulder and Elbow Surgeons’ Score [ASES]: 35 vs. 39 points, Mayo Elbow Performance Index [MEPI]: 87 vs. 94 points). However, none of the clinical parameters in this comparison could be considered as statistically significant. The overall missing evidence of an association between radial head fractures and a specific fracture type might be due to the small number of fractures analyzed in the respective studies. This is also confirmed by the results of Watts et al., where no such association could be found in their study including 79 distal intra-articular shear fractures of the humerus [27].
The severity of intra-articular distal humeral fractures was first appreciated by Ring et al. [19]. They could only appreciate the complexity of the fractures upon surgical exposure during operative treatment and therefore recommend operative treatment with implants buried under the articular surface to restore function [19]. Operative treatment of capitellar fractures has also been shown to confer favorable clinical outcomes compared with nonoperative treatment and is therefore generally recommended in most cases [2, 4, 8, 9, 11,12,13,14, 18, 21, 22, 24,25,26]. A high incidence of associated injuries, especially of the radial head, may be explained as follows: fractures of the capitellum humeri frequently occur during a direct blow to the elbow or a fall on the outstretched arm, identical to the mechanism leading to a radial head fracture [1, 3, 16, 20]. In this scenario, associated radial head fractures (or capitellar fractures) can be viewed as corresponding lesions on the opposite site of the joint, a phenomenon that has been termed “kissing lesion” on the elbow by Claessen et al. [6]. This term is also used for opposing osteochondral lesions in other regions such as the talotibial joint [23]. In the elbow joint, however, this term has also been used for lateral osteochondral lesions caused by repetitive trauma [7].
Generally, cartilage injuries of the capitellum are known to be frequently present in patients with radial head fractures. Such lesions can be missed in preoperative imaging and may only be evident intraoperatively [5, 17]. Interestingly, Nalbantoglu et al. showed that higher grades of cartilage injuries are created by lower-grade radial head fractures, since the intact radial head can cause greater damage to the capitellum [17]. Consequently, both radial head and capitellum fractures, which in most cases result from patients falling on the outstretched arm, are regularly associated with related injuries of the corresponding joint.
Limitations
The present study has certain limitations. First, owing to the low incidence of capitellar fractures, significant injuries associated with certain fracture types could not be found. Also, we only present the retrospective data acquired from patients treated for fractures of the capitellum. Differences in clinical outcomes of capitellar fractures with associated injuries at the elbow joint may reveal specific treatment strategies for these patients and need to be addressed in future studies.
Practical conclusion
-
The incidence of radial head fractures is high in patients with fractures of the capitellum humeri.
-
Missed lesions of the radial head in patients with capitellar fractures may lead to inferior outcomes in such cases.
-
A thorough inspection of the surrounding structures on radiographic images or intraoperatively is imperative, and fractures should be treated accordingly.
References
Amis AA, Miller JH (1995) The mechanisms of elbow fractures: an investigation using impact tests in vitro. Injury 26:163–168. https://doi.org/10.1016/0020-1383(95)93494-3
Ashwood N, Verma M, Hamlet M et al (2010) Transarticular shear fractures of the distal humerus. J Shoulder Elbow Surg 19:46–52. https://doi.org/10.1016/j.jse.2009.07.061
Bennett JB (1993) Radial head fractures: diagnosis and management. J Shoulder Elbow Surg 2:264–273. https://doi.org/10.1016/S1058-2746(09)80088-8
Brouwer KM, Jupiter JB, Ring D (2011) Nonunion of operatively treated capitellum and trochlear fractures. J Hand Surg Am 36:804–807. https://doi.org/10.1016/j.jhsa.2011.01.022
Caputo AE, Burton KJ, Cohen MS, King GJ (2006) Articular cartilage injuries of the capitellum interposed in radial head fractures: a report of ten cases. J Shoulder Elbow Surg 15:716–720. https://doi.org/10.1016/j.jse.2006.01.007
Claessen F, Kachooei A, Verheij K et al (2016) Outcomes of concomitant fractures of the radial head and capitellum: the “kissing lesion”. J Hand Microsurg 8:100–105. https://doi.org/10.1055/s-0036-1585430
Clarke RP (1988) Symptomatic, lateral synovial fringe (plica) of the elbow joint. Arthroscopy 4:112–116. https://doi.org/10.1016/S0749-8063(88)80077-X
Dubberley JH, Faber KJ, Macdermid JC et al (2006) Outcome after open reduction and internal fixation of capitellar and trochlear fractures. J Bone Joint Surg Am 88:46–54. https://doi.org/10.2106/JBJS.D.02954
Frank JM, Saltzman BM, Garbis N, Cohen MS (2016) Articular shear injuries of the capitellum in adolescents. J Shoulder Elbow Surg 25:1485–1490. https://doi.org/10.1016/j.jse.2016.03.013
Hahn NF (1853) Fall von einer besonderen Varietät der Frakturen des Ellenbogens. Z Wundärzte Geburtshelf 6:185–189
Hirvensalo E, Bostman O, Partio E et al (1993) Fracture of the humeral capitellum fixed with absorbable polyglycolide pins. 1‑year follow-up of 8 adults. Acta Orthop Scand 64:85–86. https://doi.org/10.3109/17453679308994538
Mahirogullari M, Kiral A, Solakoglu C et al (2006) Treatment of fractures of the humeral capitellum using herbert screws. J Hand Surg Am 31:320–325. https://doi.org/10.1016/j.jhsb.2006.02.002
McKee MD, Jupiter JB, Bamberger HB (1996) Coronal shear fractures of the distal end of the humerus. J Bone Joint Surg Am 78:49–54
Mehdian H, McKee MD (2000) Fractures of capitellum and trochlea. Orthop Clin North Am 31:115–127. https://doi.org/10.1016/S0030-5898(05)70132-2
Morrey B, Sanchez Sotelo J, Morrey M (2017) The elbow and its disorders, 5th edn., pp 458–465
Morrey BF, An KN, Stormont TJ (1988) Force transmission through the radial head. J Bone Joint Surg Am 70:250–256
Nalbantoglu U, Gereli A, Kocaoglu B et al (2008) Capitellar cartilage injuries concomitant with radial head fractures. J Hand Surg Am 33:1602–1607. https://doi.org/10.1016/j.jhsa.2008.05.016
Ong KL, Mahadev A (2011) Cannulated cancellous screw fixation for capitellum fractures in adolescents. J Orthop Surg (Hong Kong) 19:346–349
Ring D, Jupiter JB, Gulotta L (2003) Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 85–A:232–238
Rizzo M, Nunley JA (2002) Fractures of the elbow’s lateral column radial head and capitellum. Hand Clin 18:21–42. https://doi.org/10.1016/S0749-0712(02)00011-2
Ruchelsman DE, Tejwani NC, Kwon YW, Egol KA (2008) Open reduction and internal fixation of capitellar fractures with headless screws. J Bone Joint Surg Am 90:1321–1329. https://doi.org/10.2106/JBJS.G.00940
Sano S, Rokkaku T, Saito S et al (2005) Herbert screw fixation of capitellar fractures. J Shoulder Elbow Surg 14:307–311. https://doi.org/10.1016/j.jse.2004.09.005
Sijbrandij ES, Van Gils APG, Louwerens JWK, De Lange EE (2000) Posttraumatic subchondral bone contusions and fractures of the talotibial joint: occurrence of “kissing” lesions. AJR Am J Roentgenol 175:1707–1710. https://doi.org/10.2214/ajr.175.6.1751707
Singh AP, Vaishya R, Jain A, Gulati D (2010) Fractures of capitellum: a review of 14 cases treated by open reduction and internal fixation with Herbert screws. Int Orthop 34:897–901. https://doi.org/10.1007/s00264-009-0896-9
Stamatis E, Paxinos O (2003) The treatment and functional outcome of type IV coronal shear fractures of the distal humerus: a retrospective review of five cases. J Orthop Trauma 17:279–284
Vaishya R, Vijay V, Jha GK, Agarwal AK (2016) Open reduction and internal fixation of capitellar fracture through anterolateral approach with headless double-threaded compression screws: a series of 16 patients. J Shoulder Elbow Surg:1–7. https://doi.org/10.1016/j.jse.2016.01.034
Watts AC, Morris A, Robinson CM (2007) Fractures of the distal humeral articular surface. J Bone Joint Surg Br 89:510–515. https://doi.org/10.1302/0301-620X.89B4.18284
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
V. Rausch, M. Königshausen, T.A. Schildhauer, J. Gessmann, and D. Seybold declare that they have no competing interests.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The local ethics committee approved this study (Reg. Nr.: 15-5364). Written consent was given by all participants. In the case of underage patients, consent was obtained from a parent or legal guardian.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Rausch, V., Königshausen, M., Schildhauer, T.A. et al. Fractures of the capitellum humeri and their associated injuries. Obere Extremität 13, 33–37 (2018). https://doi.org/10.1007/s11678-018-0441-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11678-018-0441-9