
Abstract
Exposure to environmental chemicals can modulate the developing immune system, but its role in the pathogenesis of type 1 diabetes is largely unexplored. Our objective was to study the levels of circulating concentrations of environmental pollutants during the first years of life and their associations with the later risk of diabetes-predictive autoantibodies. From two birth-cohort studies including newborn infants with HLA-conferred susceptibility to type 1 diabetes (FINDIA and DIABIMMUNE), we identified case children with at least one biochemical diabetes-associated autoantibody (n = 30–40) and from one to four autoantibody-negative controls per each case child matched for age, gender, diabetes-related HLA-risk, delivery hospital, and, in FINDIA, also dietary intervention group. Plasma levels of 13 persistent organic pollutants and 14 per- and polyfluorinated substances were analyzed in cord blood and plasma samples taken at the age of 12 and 48 months. Both breastfeeding and the geographical living environment showed association with circulating concentrations of some of the chemicals. Breastfeeding-adjusted conditional logistic regression model showed association between decreased plasma HBC concentration at 12-month-old children and the appearance of diabetes-associated autoantibodies (HR, 0.989; 95% Cl, 0.978–1.000; P = 0.048). No association was found between the plasma chemical levels and the development of clinical type 1 diabetes. Our results do not support the view that exposure to the studied environmental chemicals during fetal life or early childhood is a significant risk factor for later development of β-cell autoimmunity and type 1 diabetes.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Type 1 diabetes is an autoimmune disease caused by T cell-mediated destruction of the pancreatic β-cells. The disease process takes usually years from its initiation to overt diabetes. In the asymptomatic preclinical period, autoantibodies against several β-cell-derived antigens appear into the peripheral circulation (Bottazzo et al. 1974). These autoantibodies include islet cell antibodies (ICA), insulin autoantibodies (IAA), GAD antibodies (GADA), insulinoma-associated-2 antibodies (IA-2A), and zinc transporter 8 antibodies (ZnT8A) (Pietropaolo et al. 2012). The destruction of the pancreatic β-cells is perceived to be mediated by autoreactive T cells. Overactivation of IFN-γ-secreting Th1 (Foulis et al. 1991; Kallmann et al. 1997) and IL-17-secreting Th17 cells (Honkanen et al. 2010) and impaired function of regulatory T cells (Treg) (Lindley et al. 2005; Putnam et al. 2009) have been reported in animal models of autoimmune diabetes as well as in human type 1 diabetes. In addition, aberrancies in the phenotype and function of dendritic cells have been associated with the development of type 1 diabetes (Nieminen et al. 2012).
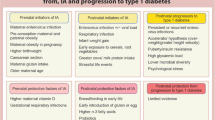
In industrialized countries, the widespread use of chemicals has been increasing simultaneously with the rise in the incidence rate of type 1 diabetes (Onkamo et al. 1999). Some of the chemicals are very persistent in the environment, bioaccumulative, and capable of interfering with biological systems at different levels. One of the known harmful effects of environmental pollutants is that they are able to modulate the functions of the human immune system. Exposure of laboratory animals to immunotoxic chemicals at early developmental stages may result in more severe effects on the immune system than exposure during adult life (reviewed in Holladay 1999). Also in humans, exposure in utero and in the first years of life is of special concern since the developing immune system of fetuses and young children is highly vulnerable to toxicant exposure (Holsapple et al. 2004).
Persistent organic pollutants (POPs) are a diverse group of organic compounds including dioxins, polychlorinated biphenyls (PCBs), pesticides, and certain brominated flame-retardants. Exposure to POPs may contribute to the development of autoimmunity, such as systemic lupus erythematosus (Cooper et al. 2008; Holladay 1999). Per- and polyfluorinated substances (PFAS) own attractive water and oil repellent characteristics and have been used in a variety of consumer and industrial applications since the 1950s (Lau et al. 2007). Perfluorooctanoic acid (PFOA) and perfluorooctane sulfonate (PFOS) are the most well-known PFAS. Both have been implicated to have immunotoxic properties (Corsini et al. 2014). Exposure to PFAS has been associated with reduced immune responses to routine childhood immunizations (Grandjean et al. 2012; Granum et al. 2013) and with an increase in the incidence of childhood asthma (Dong et al. 2011). Early life exposure to PFAS occurs both via placental transfer (Apelberg et al. 2007) and breastfeeding (Thomsen et al. 2010).
The possibility that environmental chemicals are involved in the pathogenesis of type 1 diabetes has been debated but has not so far been adequately addressed (Bodin et al. 2015; Howard and Lee 2012). Results from epidemiological studies focusing on a possible link between type 1 diabetes and exposure to POPs are contradictory. Pregnant women with type 1 diabetes had 30% higher levels of serum PCBs than controls (Longnecker and Daniels 2001). In contrast, elevated levels of PCB-153 and dichlorodiphenyldichloroethylene (p,p′-DDE) in maternal serum did not correlate with the development of type 1 diabetes in the offspring in a Swedish cohort (Rignell-Hydbom et al. 2010). In support of PCB effects on autoimmunity, the prevalence of GADA was four times higher in employees in a factory producing PCBs compared to controls (Langer et al. 2002). Several modes of action to trigger or accelerate type 1 diabetes development by chemicals have been implicated. In addition to immunomodulation, chemicals may have direct toxic effects on β-cells, may alter hormone levels, affect the microbiota, or alter intestinal permeability (Bodin et al. 2015).
There is definitely a need for studies analyzing the potential association between early life exposure to environmental chemicals and development of type 1 diabetes. Our hypothesis is that early life exposure to environmental chemicals plays a role in the development and/or progression to type 1 diabetes. In this study, we set out to investigate the association between prenatal and postnatal exposure to environmental chemicals (POPs including PFASs) and the development of β-cell autoimmunity and clinical diabetes.
Materials and methods
Study design
The role of prenatal and early life exposure to environmental chemicals in the development of β-cell autoimmunity was studied in children participating in the FINDIA pilot study (the Finnish Dietary Intervention Trial for the Prevention of Type 1 Diabetes) (Vaarala et al. 2012). Exposure to environmental chemicals in young children was studied from plasma samples from 4-year-old participants in the DIABIMMUNE study (Peet et al. 2012).
Study subjects
In the FINDIA and DIABIMMUNE studies, children with HLA genotypes conferring susceptibility to type 1 diabetes were monitored for the appearance of disease-associated autoantibodies. Cases were selected from children who developed at least one diabetes-associated biochemical autoantibody during the follow-up period (from birth to 6 years of age in FINDIA and from 3 to 5 years of age in DIABIMMUNE). For each case child, from one to four autoantibody-negative control, children matched for age, gender, diabetes-related HLA-risk, delivery hospital, and dietary intervention group (baby milk formula, in FINDIA only) were selected. With these strict matching criteria, we identified 40 cases with plasma samples taken at birth (cord blood), 36 cases with plasma samples taken at 12 months of age, and 30 cases with plasma samples taken at 4 years of age (Table 1). The cord blood samples were obtained between May 2002 and November 2005 and the 12-month samples between May 2003 and November 2006 in three pediatric hospitals in Finland as described earlier (Vaarala et al. 2012). Blood samples from 4-year-old children were drawn between October 2010 and August 2011 in pediatric hospitals of Tartu, Estonia, and Espoo, Finland (12 and 18 case-control pairs, respectively).
The local Ethical Committees approved both the FINDIA and the DIABIMMUNE studies, and the parents gave their written informed consent prior to their child’s participation in these studies.
Diabetes-associated autoantibodies
In the FINDIA study, blood samples were obtained at the follow-up visits when the children were 3, 6, and 12 months of age and thereafter annually up to the age of 6 years. In the DIABIMMUNE study, blood samples were drawn at 36, 48, and 60 months of age. Plasma samples were collected from fresh heparinized blood samples and stored at − 70 °C until analyzed. Plasma samples from both studies were screened for IAA, GADA, and IA-2A with specific radiobinding assays as previously described (Knip et al. 2010). In addition, DIABIMMUNE samples were also analyzed for ZnT8A (Knip et al. 2010). The cutoff level for autoantibody positivity was 2.80 relative units (RU) for IAA, 5.36 RU for GADA, 0.78 RU for IA-2A, and 0.61 RU for ZnT8A, representing the 99th percentiles in more than 350 Finnish non-diabetic children.
HLA genotyping
HLA typing of major risk DR-DQ haplotypes for type 1 diabetes was performed with a PCR-based lanthanide-labeled hybridization method using time-resolved fluorometry for detection as described before (Hermann et al. 2003). HLA genotyping in the FINDIA and DIABIMMUNE studies has been described in detail earlier (Peet et al. 2012; Vaarala et al. 2012).
Chemical analysis
Plasma concentrations of 13 POP compounds including PCBs 118, 138, 153, 156, 170, and 180, pesticides hexachlorobenzene (HCB), β-hexachlorocyclohexane (β-HCH), oxychlordane, trans-nonachlor, dichlorodiphenyltrichloroethane (p,p′-DDT), p,p′-DDE, and brominated diphenyl ether BDE-47 and 14 PFAS compounds including perfluorohexanesulfonic acid (PFHxS), perfluoroheptanesulfonic acid (PFHpS), perfluorooctanosulfonic acid (PFOS), perfluorononanosulfonic acid (PFNS), perfluorodecanesulfonic acid (PFDS), perfluorohexanoic acid (PFHxA), perfluoroheptanoic acid (PFHpA), perfluorooctanoic acid (PFOA), perfluorononanoic acid (PFNA), perfluorodecanoic acid (PFDA), perfluoroundecanoic acid (PFUnA), perfluorododecanoic acid (PFDoA), perfluorotridecanoic acid (PFTrA), and perfluorotetradecanoic acid (PFTeA) were analyzed. Details of sample pretreatment, instrumental analysis, and method performance have been described elsewhere (Koponen et al. 2013). In brief, the compounds were extracted from 25 to 200 μL plasma using a two-stage liquid-liquid extraction after spiking with isotope-labeled internal standards. In case of the POP measurements, the case-control pairs were reduced from 39 to 34 at 12 months of age and from 30 to 29 at 48 months of age due to insufficient sample volumes. The POP extract was further purified with a miniaturized silica column. Quantification of the POPs and PFASs was performed by GC-MS/MS and LC-MS/MS, respectively. If the concentration of any chemical was below the limit of quantification (LOQ), then the sample was given the value of the LOQ/2 in the statistical analyses.
Statistics
Conditional logistic regression was used to estimate the hazard ratios (HR) and 95% confidence intervals (CI) for the association between plasma chemical concentration and the risk of emergence of diabetes-related autoantibodies. Unadjusted analyses and analyses adjusted for the duration of the breastfeeding period were performed. When the concentration of a given chemical was below the LOQ in more than 40% of the samples analyzed, the comparisons between groups were performed using categorized values (below the LOQ vs. above the LOQ). No correction for multiple comparisons was applied; instead, multiplicity issues were taken into account by cautious interpretation of the results. The statistical analyses were done using SPSS 22 package.
Results
Plasma concentrations of the various chemicals in the FINDIA and DIABIMMUNE children, who did not show any signs of type 1 diabetes progression, i.e., remained negative for diabetes-associated autoantibodies without any type 1 diabetes diagnosis, are presented in Table 2.
A case: control conditional logistic regression model was built to establish associations between plasma chemical concentrations and the emergence of diabetes-related autoantibodies. Cases and controls were matched for age, gender, HLA risk genotype, and delivery hospital and in the FINDIA study cohort also for the milk formula given to the child.
Unadjusted plasma concentrations of the chemicals analyzed showed no association with the emergence of autoantibodies, HR values being close to 1.0 (Table 3). The only exception was that the group having PFDA above LOQ at 48 months showed an association with the appearance of autoantibodies (HR, 4.1; 95% Cl, 1.1–14.3; P = 0.028). The PFDA concentrations were below the detection limit in 46% of the 48-month samples, and therefore, the PFDA results were analyzed as categorized variables, below the LOQ or above the LOQ.
The duration of the breastfeeding period based on maternal questionnaires was available for 92.5% of children in the FINDIA study and for 84.9% of children in the DIABIMMUNE study. Breastfeeding alone did not associate with the appearance of autoantibodies in either study cohort. As expected, the duration of the breastfeeding period correlated directly with the plasma chemical concentrations (Supplemental Table S1). We performed conditional logistic regression analysis adjusted for the duration of the breastfeeding period (Table 3). Breastfeeding period was categorized into four groups, namely, 0–4, 4–8, 8–12, and more than 12 months of breastfeeding. The only significant finding in the conditional logistic regression analyses adjusted for the duration of breastfeeding was the observation that low plasma HCB concentrations in 12-month-old children were associated with the appearance of diabetes-associated autoantibodies (HR, 0.989; 95% Cl, 0.978–1.000; P = 0.048).
For both study cohorts, the type 1 diabetes diagnoses were updated as of November 2017 (Table 1). Almost all children with type 1 diabetes were derived from the group of autoantibody positive cases, and accordingly, it was possible to establish a matched type 1 diabetes case: control set for conditional logistic regression as well. The follow-up for type 1 diabetes was much longer than the follow-up for autoantibodies, and some children who were initially classified as autoantibody negative controls were later diagnosed with type 1 diabetes. These children were excluded from the control groups and included in the type 1 diabetes case group. When defining children diagnosed with overt type 1 diabetes as a case, no associations with plasma chemical concentrations were observed. That was the true both for unadjusted and adjusted analyses.
Matching factors
Among the matching factors, only the HLA risk genotype did not associate with plasma chemical concentrations.
Gender
Cord blood plasma PFOS concentrations were higher in boys (4.2 ± 3.3 ng/mL; mean ± SD) than those in girls (3.1 ± 1.6 ng/mL; P = 0.001, Mann-Whitney U test). No other gender-related differences were observed.
= 0.028. The PFDA concentrations were below the detection limit in 46% of the 48-month samples, and therefore, the PFDA results were analyzed as categorized variables, below the LOQ or above the LOQ
Geographic location
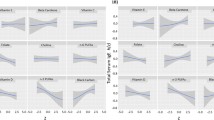
Geographic location affected the circulating concentrations of environmental chemicals. Statistically significant findings are presented for FINDIA in Table 4 and for DIABIMMUNE in Table 5. In the FINDIA study, three Finnish regions were compared. The infants residing in the capital region of Helsinki had higher concentrations of p,p′-DDE, PCB-153, PCB-138, PFOA, and PFOS in cord blood plasma than children residing in smaller cities (Jyväskylä and Kuopio; Table 4) or their surroundings. The same phenomenon was observed for the plasma concentrations of PFNA, PFDA, and PFHxS in 12-month-old infants (Table 4).
In the DIABIMMUNE study, the 48-month-old children living in the Estonian city of Tartu and its adjacent areas had higher plasma levels of HCB, β-HCH, p,p′-DDE, PCB-118, and PCB-138 than children living in the city of Espoo, Finland (Table 5). In contrast, children residing in Espoo had higher concentrations of plasma PFOA than children residing in Tartu.
Milk formula group
In the FINDIA study, the participants were randomized to be weaned to three different milk formulas. One of the milk formulas was offered to each participant, and breastfeeding was encouraged. A fourth study group comprised children who used no milk formula and relied solely on breastfeeding as his/her milk intake. Plasma chemical concentrations did not differ between the three milk formula groups at the age of 12 months. However, solely breastfed children had higher concentrations of eight POP and five PFAS compounds when combined with pooled milk formula groups (Supplemental Table S2).
Conclusions
In our study, we analyzed the circulating concentrations of a multitude of environmental pollutants in two matched case-control series. We could not observe any definite associations between increased exposure to chemical pollutants at birth, at 12 or at 48 months of age, and risk of β-cell autoimmunity. The current work indicates that prenatal or early childhood exposure to POPs, including PFASs, is not an apparent risk factor for later β-cell autoimmunity. To our knowledge, this is the first report based on HLA-matched case-control series where exposure to environmental pollutants and the development of β-cell autoimmunity and type 1 diabetes have been studied.
In 48-month-old children, PFDA was above the LOQ in 34% of the autoantibody-negative children, in 63% of the autoantibody-positive children, and in 88% of the children diagnosed with type 1 diabetes. PFDA has been demonstrated to interfere with the function of thyroid hormones in in vitro studies (Long et al. 2013), and endocrine disruption is an interesting mode of action of PFDA in biological systems. It has been shown that PFDA, at concentrations of 100 ng/mL and above, can impair LPS-induced release of TNF-α in peripheral blood leukocytes and prevent LPS-induced I-κB degradation (Corsini et al. 2012). However, it should be mentioned that since PFDA was present at very low concentrations (less than 1 ng/mL) in the current study, the results do not really support any association between elevated circulating concentrations of PFDA and β-cell autoimmunity and/or emergence of type 1 diabetes.
Plasma HCB concentrations at the age of 12 months were actually decreased in case children who developed diabetes-associated autoantibodies by the age of 6 years when compared to children who remained autoantibody-negative, but only after adjustment for breastfeeding. It is of interest that an inverse association has been reported earlier between HCB and circulating concentrations of IFN-γ, indicating that exposure to HCB may downregulate Th1 immunity (Daniel et al. 2001), which has been implicated to be involved in immune-mediated β-cell destruction. Although the present study could be interpreted as indicating slower progression to β-cell destruction in children with increased HCB concentrations, which is to some extent supported by existing literature, there are also arguments against such a view. First, the decrease in plasma levels of HCB in affected children was present only in plasma samples taken at 12 months of age. No changes in plasma levels of HCB were seen in samples taken at birth or at 48 months of age. Second, this finding should be interpreted cautiously since the comparisons were not corrected for multiple comparisons. Third, the higher circulating concentrations of chemicals in children without any signs of β-cell autoimmunity may be explained by other factors protecting against diabetes, e.g., their nutritional pattern. It is known that long-chain fatty acids from fish, the main source of POPs, may protect from β-cell autoimmunity (Rignell-Hydbom et al. 2010). As a conclusion, without further investigations, it is too early to make the statement that increased exposure to HCB protects from β-cell autoimmunity or from type 1 diabetes. Merely, the current work indicates that exposure to HCB, at current concentrations, is not harmful in relation to the development of type 1 diabetes.
The present study was designed to investigate whether early exposure to environmental chemicals associates with β-cell destruction. Although the number of cases, especially for type 1 diabetes cases, is rather low, the value of the present study lays in powerful matching of pairs that were included in the statistical analysis. The confounding factors introduced by age, gender, geographical location, and milk formula groups could be eliminated and further, the effect of the duration of the breastfeeding period could be adjusted for in conditional logistic regression analyses.
We found higher PFOS concentrations in cord blood plasma in boys than in girls, which is in line with earlier studies (Wang et al. 2011). The circulating concentrations of several POPs were higher in Estonian children than those in Finnish children. These are mainly chemicals used in the industry and agriculture before their global restrictions, the usage history of which may well explain the current findings. However, the incidence of type 1 diabetes is substantially lower in Estonia than in the less exposed Finnish population (Harjutsalo et al. 2013; Teeaar et al. 2010) suggesting that exposure to these POPs is not involved in the disease process resulting in type 1 diabetes.
The current study is in line with earlier observations that breastfeeding is an important route of certain persistent chemicals (Kiviranta et al. 1999). Although the current study does not support the protective role of breastfeeding, it should be mentioned that some surveys have shown that breastfeeding may protect against type 1 diabetes (Pereira et al. 2014).
The duration of breastfeeding and geographical location were found to be associated with plasma concentrations of several persistent organic pollutants and per- and polyfluorinated substances in early life. This is in line with previous studies. Taken together, our results suggest that exposure to persistent organic pollutants and per- and polyfluorinated substances, at current levels, does not have any effect on the induction of β-cell autoimmunity or progression from β-cell autoimmunity to clinical type 1 diabetes.
References
Apelberg BJ, Witter FR, Herbstman JB, Calafat AM, Halden RU, Needham LL, Goldman LR (2007) Cord serum concentrations of perfluorooctane sulfonate (PFOS) and perfluorooctanoate (PFOA) in relation to weight and size at birth. Environ Health Perspect 115:1670–1676. https://doi.org/10.1289/ehp.10334
Bodin J, Stene LC, Nygaard UC (2015) Can exposure to environmental chemicals increase the risk of diabetes type 1 development? Biomed Res Int 2015:208947. https://doi.org/10.1155/2015/208947
Bottazzo GF, Florin-Christensen A, Doniach D (1974) Islet-cell antibodies in diabetes mellitus with autoimmune polyendocrine deficiencies. Lancet 2:1279–1283
Cooper GS, Gilbert KM, Greidinger EL, James JA, Pfau JC, Reinlib L, Richardson BC, Rose NR (2008) Recent advances and opportunities in research on lupus: environmental influences and mechanisms of disease. Environ Health Perspect 116:695–702. https://doi.org/10.1289/ehp.11092
Corsini E, Sangiovanni E, Avogadro A, Galbiati V, Viviani B, Marinovich M, Galli CL, Dell’Agli M, Germolec DR (2012) In vitro characterization of the immunotoxic potential of several perfluorinated compounds (PCFs). Toxicol Appl Pharmacol 258:248–255
Corsini E, Luebke RW, Germolec DR, DeWitt JC (2014) Perfluorinated compounds: emerging POPs with potential immunotoxicity. Toxicol Lett 230:263–270. https://doi.org/10.1016/j.toxlet.2014.01.038
Daniel V, Huber W, Bauer K, Suesal C, Conradt C, Opelz G (2001) Associations of blood levels of PCB, HCHs, and HCB with numbers of lymphocyte subpopulations, in vitro lymphocyte response, plasma cytokine levels, and immunoglobulin autoantibodies. Environ Health Perspect 109:173–178. https://doi.org/10.2307/3434772
Dong GH, Liu MM, Wang D, Zheng L, Liang ZF, Jin YH (2011) Sub-chronic effect of perfluorooctanesulfonate (PFOS) on the balance of type 1 and type 2 cytokine in adult C57BL6 mice. Arch Toxicol 85:1235–1244. https://doi.org/10.1007/s00204-011-0661-x
Foulis AK, Mcgill M, Farquharson MA (1991) Insulitis in Type-1 (insulin-dependent) diabetes-mellitus in man - macrophages, lymphocytes, and interferon-gamma containing cells. J Pathol 165:97–103. https://doi.org/10.1002/path.1711650203
Grandjean P, Andersen EW, Budtz-Jorgensen E, Nielsen F, Molbak K, Weihe P, Heilmann C (2012) Serum vaccine antibody concentrations in children exposed to perfluorinated compounds. JAMA 307:391–397. https://doi.org/10.1001/jama.2011.2034
Granum B, Haug LS, Namork E, Stølevik SB, Thomsen C, Aaberge IS, van Loveren H, Løvik M, Nygaard UC (2013) Pre-natal exposure to perfluoroalkyl substances may be associated with altered vaccine antibody levels and immune-related health outcomes in early childhood. J Immunotoxicol 10:373–379. https://doi.org/10.3109/1547691X.2012.755580
Harjutsalo V, Sund R, Knip M, Groop PH (2013) Incidence of type 1 diabetes in Finland. JAMA 310:427–428. https://doi.org/10.1001/jama.2013.8399
Hermann R et al (2003) HLA DR-DQ-encoded genetic determinants of childhood-onset type 1 diabetes in Finland: an analysis of 622 nuclear families. Tissue Antigens 62:162–169
Holladay SD (1999) Prenatal immunotoxicant exposure and postnatal autoimmune disease. Environ Health Perspect 107:687–691. https://doi.org/10.2307/3434328
Holsapple MP, Paustenbach DJ, Charnley G, West LJ, Luster MI, Dietert RR, Burns-Naas LA (2004) Symposium summary: children’s health risk—what’s so special about the developing immune system? Toxicol Appl Pharmacol 199:61–70. https://doi.org/10.1016/j.taap.2004.03.003
Honkanen J, Nieminen JK, Gao R, Luopajarvi K, Salo HM, Ilonen J, Knip M, Otonkoski T, Vaarala O (2010) IL-17 immunity in human type 1 diabetes. J Immunol 185:1959–1967. https://doi.org/10.4049/jimmunol.1000788
Howard SG, Lee DH (2012) What is the role of human contamination by environmental chemicals in the development of type 1 diabetes? J Epidemiol Community Health 66:479–481
Kallmann BA, Huther M, Tubes M, Feldkamp J, Bertrams J, Gries FA, Lampeter EF, Kolb H (1997) Systemic bias of cytokine production toward cell-mediated immune regulation in IDDM and toward humoral immunity in Graves’ disease. Diabetes 46:237–243
Kiviranta H, Purkunen R, Vartiainen T (1999) Levels and trends of PCDD/Fs and PCBs in human milk in Finland. Chemosphere 38:311–323
Knip M, Virtanen SM, Seppä K, Ilonen J, Savilahti E, Vaarala O, Reunanen A, Teramo K, Hämäläinen AM, Paronen J, Dosch HM, Hakulinen T, Akerblom HK, Finnish TRIGR Study Group (2010) Dietary intervention in infancy and later signs of beta-cell autoimmunity. N Engl J Med 363:1900–1908. https://doi.org/10.1056/NEJMoa1004809
Koponen J, Rantakokko P, Airaksinen R, Kiviranta H (2013) Determination of selected perfluorinated alkyl acids and persistent organic pollutants from a small volume human serum sample relevant for epidemiological studies. J Chromatogr A 1309:48–55. https://doi.org/10.1016/j.chroma.2013.07.064
Langer P, Tajtáková M, Guretzki HJ, Kočan A, Petrík J, Chovancová J, Drobná B, Jursa S, Pavúk M, Trnovec T, Šeböková E, Klimeš I (2002) High prevalence of anti-glutamic acid decarboxylase (anti-GAD) antibodies in employees at a polychlorinated biphenyl production factory. Arch Environ Health 57:412–415
Lau C, Anitole K, Hodes C, Lai D, Pfahles-Hutchens A, Seed J (2007) Perfluoroalkyl acids: a review of monitoring and toxicological findings. Toxicol Sci 99:366–394. https://doi.org/10.1093/toxsci/kfm128
Lindley S, Dayan CM, Bishop A, Roep BO, Peakman M, Tree TI (2005) Defective suppressor function in CD4(+)CD25(+) T-cells from patients with type 1 diabetes. Diabetes 54:92–99
Long M, Ghisari M, Bonefeld-Jorgensen EC (2013) Effects of perfluoroalkyl acids on the function of the thyroid hormone and the aryl hydrocarbon receptor. Environ Sci Pollut Res Int 20:8045–8056. https://doi.org/10.1007/s11356-013-1628-7
Longnecker MP, Daniels JL (2001) Environmental contaminants as etiologic factors for diabetes. Environ Health Perspect 109:871–876. https://doi.org/10.2307/3454649
Nieminen JK, Vakkila J, Salo HM, Ekstrom N, Harkonen T, Ilonen J, Knip M, Vaarala O (2012) Altered phenotype of peripheral blood dendritic cells in pediatric type 1 diabetes. Diabetes Care 35:2303–2310. https://doi.org/10.2337/dc11-2460
Onkamo P, Vaananen S, Karvonen M, Tuomilehto J (1999) Worldwide increase in incidence of type I diabetes--the analysis of the data on published incidence trends. Diabetologia 42:1395–1403. https://doi.org/10.1007/s001250051309
Peet A, Kool P, Ilonen J, Knip M, Tillmann V, Group DS (2012) Birth weight in newborn infants with different diabetes-associated HLA genotypes in three neighbouring countries: Finland, Estonia and Russian Karelia. Diabetes Metab Res Rev 28:455–461. https://doi.org/10.1002/dmrr.2303
Pereira PF, Alfenas Rde C, Araujo RM (2014) Does breastfeeding influence the risk of developing diabetes mellitus in children? A review of current evidence. J Pediatr 90:7–15. https://doi.org/10.1016/j.jped.2013.02.024
Pietropaolo M, Towns R, Eisenbarth GS (2012) Humoral autoimmunity in type 1 diabetes: prediction, significance, and detection of distinct disease subtypes. Cold Spring Harb Perspect Med 2:1–18. https://doi.org/10.1101/cshperspect.a012831
Putnam AL, Brusko TM, Lee MR, Liu W, Szot GL, Ghosh T, Atkinson MA, Bluestone JA (2009) Expansion of human regulatory T-cells from patients with type 1 diabetes. Diabetes 58:652–662. https://doi.org/10.2337/db08-1168
Rignell-Hydbom A, Elfving M, Ivarsson SA, Lindh C, Jonsson BA, Olofsson P, Rylander L (2010) A nested case-control study of intrauterine exposure to persistent organochlorine pollutants in relation to risk of type 1 diabetes. PLoS One 5:e11281. https://doi.org/10.1371/journal.pone.0011281
Teeaar T et al (2010) Increasing incidence of childhood-onset type 1 diabetes mellitus among Estonian children in 1999-2006. Time trend analysis 1983-2006. Pediatr Diabetes 11:107–110. https://doi.org/10.1111/j.1399-5448.2009.00535.x
Thomsen C, Haug LS, Stigum H, Froshaug M, Broadwell SL, Becher G (2010) Changes in concentrations of perfluorinated compounds, polybrominated diphenyl ethers, and polychlorinated biphenyls in Norwegian breast-milk during twelve months of lactation. Environ Sci Technol 44:9550–9556. https://doi.org/10.1021/es1021922
Vaarala O, Ilonen J, Ruohtula T, Pesola J, Virtanen SM, Härkönen T, Koski M, Kallioinen H, Tossavainen O, Poussa T, Järvenpää AL, Komulainen J, Lounamaa R, Åkerblom HK, Knip M (2012) Removal of bovine insulin from cow’s milk formula and early initiation of beta-cell autoimmunity in the FINDIA pilot study. Arch Pediatr Adolesc Med 166:608–614. https://doi.org/10.1001/archpediatrics.2011.1559
Wang IJ, Hsieh WS, Chen CY, Fletcher T, Lien GW, Chiang HL, Chiang CF, Wu TN, Chen PC (2011) The effect of prenatal perfluorinated chemicals exposures on pediatric atopy. Environ Res 111:785–791. https://doi.org/10.1016/j.envres.2011.04.006
Acknowledgments
Open access funding provided by University of Helsinki including Helsinki University Central Hospital. We are grateful to Tuula Rissanen for excellent assistance in plasma chemical analyses of POP substances. We thank Berta Davydova, Sinikka Helander, Juho Hämäläinen, Mevlida Kararic, Markku Latva-Koivisto, Tiina Nurmi, and Iiris Ollila for technical assistance with the autoantibody assays. Matti Koski is acknowledged for assistance in the database work. We also thank all the local study nurses and participating families for their commitment to the FINDIA or DIABIMMUNE studies.
Members of the DIABIMMUNE Study Group: Mikael Knip, PI (Children’s Hospital, University of Helsinki), Katriina Koski, Coordinator (Clinicum, University of Helsinki), Matti Koski (IT Manager, Clinicum, University of Helsinki), Taina Härkönen (Children’s Hospital, University of Helsinki), Samppa Ryhänen (Children’s Hospital, University of Helsinki), Anu-Maaria Hämäläinen (Jorvi Hospital, Helsinki University Hospital), Anne Ormisson (Children’s Clinic, Tartu University Hospital), Aleksandr Peet (Department of Pediatrics, Tartu University Hospital), Vallo Tillmann (Department of Pediatrics, Tartu University Hospital), Valentina Ulich (Ministry of Health and Social Development, Karelian Republic of the Russian Federation), Elena Kuzmicheva (Ministry of Health and Social Development, Karelian Republic of the Russian Federation), Sergei Mokurov (Ministry of Health and Social Development, Karelian Republic of the Russian Federation), Svetlana Markova (Children’s Republic Hospital, Karelian Republic of the Russian Federation), Svetlana Pylova (Children’s Republic Hospital, Karelian Republic of the Russian Federation), Marina Isakova (Perinatal Center, Karelian Republic of the Russian Federation), Elena Shakurova (Perinatal Center, Karelian Republic of the Russian Federation), Vladimir Petrov (Maternity Hospital N° 1, Petrozavodsk), Natalya V. Dorshakova (Petrozavodsk State University), Tatyana Karapetyan (Petrozavodsk State University), Tatyana Varlamova (Petrozavodsk State University), Jorma Ilonen (Immunogenetics Laboratory, University of Turku and Turku University Hospital), Minna Kiviniemi (Immunogenetics Laboratory, University of Turku), Kristi Alnek (Department of Immunology, University of Tartu), Helis Janson (Department of Immunology, University of Tartu) Raivo Uibo (Department of Immunology, University of Tartu), Tiit Salum (OÜ Immunotron, Tartu), Erika von Mutius (Children’s Hospital, Ludwig Maximilians Universität, Munchen), Juliane Weber (Children’s Hospital, Ludwig Maximilians Universität, Munchen), Helena Ahlfors (Turku Centre of Biotechnology, University of Turku and Åbo Akademi), Henna Kallionpää, (Turku Centre of Biotechnology, University of Turku and Åbo Akademi), Essi Laajala (Turku Centre of Biotechnology, University of Turku and Åbo Akademi), Riitta Lahesmaa (Turku Centre of Biotechnology, University of Turku and Åbo Akademi), Harri Lähdesmäki (Turku Centre of Biotechnology, University of Turku and Åbo Akademi), Robert Molder (Turku Centre of Biotechnology, University of Turku and Åbo Akademi), Janne Nieminen (Department of Neurology, Helsinki University Hospital), Terhi Ruohtula (Clinicum, University of Helsinki) Outi Vaarala (Clinicum, University of Helsinki), Hanna Honkanen (Department of Virology, University of Tampere), Heikki Hyöty (Department of Virology, University of Tampere and Tampere University Hospital), Anita Kondrashova (Department of Virology, University of Tampere), Sami Oikarinen (Department of Virology, University of Tampere), Hermie J.M. Harmsen (University Medical Center Groningen), Marcus C. De Goffau (University Medical Center Groningen), Gjalt Welling (University Medical Center Groningen), Kirsi Alahuhta (Department for Welfare and Health Promotion, National Institute for Health and Welfare, Helsinki), Suvi M. Virtanen (Department for Health, National Institute for Health and Welfare, Helsinki).
Funding
This work was supported by the European Union Seventh Framework Program (FP7/2007–2013) under Grant 202063 and the Academy of Finland (to O.V. and Centre of Excellence in Molecular Systems Immunology and Physiology Research [2012–2017], Decision 250114 to M.K.), as well as by the Sigrid Juselius Foundation and the Finnish Diabetes Research Foundation.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
The local Ethical Committees approved both the FINDIA and the DIABIMMUNE studies, and the parents gave their written informed consent prior to their child’s participation in these studies.
Duality of interest
Dr. Outi Vaarala is an employee of Astra Zeneca as of August 1, 2014. No other potential conflicts of interest relevant to this article were reported.
Additional information
Responsible editor: Philippe Garrigues
Electronic supplementary material
ESM 1
(DOCX 16 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Salo, H.M., Koponen, J., Kiviranta, H. et al. No evidence of the role of early chemical exposure in the development of β-cell autoimmunity. Environ Sci Pollut Res 26, 1370–1378 (2019). https://doi.org/10.1007/s11356-018-3659-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-018-3659-6