
Abstract
Purpose
Research during the past 10–20 years shows that positional therapy (PT) has a significant influence on the apnea–hypopnea index. These studies are predominantly performed as case series on a comparably small number of patients. Still, results have not found their way into the daily diagnostic and treatment routine. An average of 56 % of patients with obstructive sleep apnea (OSA) have position-dependent OSA (POSA), commonly defined as a difference of 50 % or more in apnea index between supine and non-supine positions. A great deal could be gained in treating patients with POSA with PT. The aim of this paper was to perform a thorough review of the literature on positional sleep apnea and its therapy.
Methods
A broad search strategy was run electronically in the MEDLINE and EMBASE databases using synonyms for position and sleep apnea.
Results
Sixteen studies were found which examined the effect of PT on OSA. In this literature review, we discuss the various techniques, results, and compliance rates.
Conclusion
Long-term compliance for PT remains an issue, and although remarkable results have been shown using innovative treatment concepts for PT, there is room for both technical improvement of the devices and for further research.
Similar content being viewed by others


Introduction
Snoring and obstructive sleep apnea (OSA) are the most prevalent sleep-disordered breathing problems. OSA affects 2–26 % of the general population, depending on gender, age, and definition of the criteria used [1, 2]. OSA is associated with significant morbidity, such as excessive daytime sleepiness, socially unacceptable snoring, and impaired quality of life. Patients are at higher risk of developing cardiovascular diseases [3, 4]. If the apnea–hypopnea index (AHI) is >40, the risk of being involved in a traffic accident increases [5, 6].
Adequate treatment is of key importance. Continuous positive airway pressure (CPAP) is regarded as the gold standard treatment of OSA, with mandibular advancement device (MAD) therapy or surgery in reserve for CPAP failures [7]. Unfortunately, 29–83 % of patients prescribed CPAP are non-adherent and use their CPAP less than 4 h per night [8, 9]. In cases of CPAP failure, treatment remains indicated. MADs and a variety of surgical interventions are then available [10–15]. All these treatment modalities have their specific downsides.
Conservative treatment of OSA can be just as crucial: lifestyle alterations such as weight reduction, abstinence of alcohol and sedatives, and avoidance of supine sleeping position, where appropriate. Significant improvement and even remission was recorded in obese patients diagnosed with OSA undergoing BS [16]. The latter should be considered as a treatment option for patients with severe OSA and obesity alongside CPAP.
A number of papers have been published on the role of supine position on OSA and methods to avoid supine position. In 1948, in a “plea for more serious consideration of snoring,” Robin [17] stated that “sleeping on one’s back is considered a common cause of snoring.” It is likely that spouses of (apneic or non-apneic) snorers were the first to identify the role of body position on the severity of the snoring or apnea of their bed partner. In 1984, Chest published a letter written by a patient’s wife [18]. She had cured her husband’s sleep apnea snoring problem by “having sewn a pocket into the back of a T-shirt and having inserted a hollow, lightweight plastic ball to prevent her husband sleeping on his back.” During the American War of Independence (1775–1783) and later during World War I (1914–1918), soldiers were advised to wear their rucksacks (filled with a bulky mass) while sleeping in order to avoid sleeping on their backs and reduce snoring so as to avoid making their position known to the enemy.
PT, in whichever form, has been found to have a significant influence on snoring and OSA severity [7]. Still, results have not found their way into the daily OSA diagnostic and treatment routine, even though approximately 56 % of patients with OSA have position-dependent OSA [19–22]. Why is PT unfashionable?
By means of a thorough review of the literature on positional sleep apnea and its therapy, this study aims to provide an overview of the various PT techniques and their success and compliance rates.
Method
A broad search strategy was run electronically in the MEDLINE and EMBASE databases on 5 October 2011 by one researcher (M.R.): (“Position” OR “position dependent“ OR “positional” OR “posture”) AND (“apnea” OR “apnoea” OR “OSA” OR “OSAS” OR snor*). In addition, the reference lists of included articles were screened for additional relevant citations. Studies were evaluated according to the Oxford Centre for Evidence-Based Medicine levels of evidence (Table 1).
Diagnosis
Current definition of OSA and POSA
The recommended objective diagnostic criteria for OSA include an AHI of 5 or more and evidence of daytime sleepiness. The AHI is defined as the mean number of apneas and hypopneas per hour during sleep, an apnea is a period of 10 s or more with a reduction of oronasal airflow of >90 %. A hypopnea is defined as an episode of more than 30 % airflow reduction of the baseline (calculated from the preceding period of 100 s) during at least 10 s. Suggested AHI thresholds are 5, 15, and 30 events per hour for mild, moderate, and severe levels of OSA, respectively [23, 24].
Cartwright [25] was the first to describe the arbitrary cutoff point of a difference of 50 % or more in apnea index between supine and non-supine positions. This is the most common definition for positional obstructive sleep apnea (POSA) used today, but many question Cartwright’s criteria and apply adapted versions.
Both Mador’s and Permut’s groups defined POSA as follows: “an AHI of fewer than 5 events per hour while in the non-supine position as well as a decrease in the AHI by more than 50 %” [26, 27]. In 1998, Marklund et al. [28] defined supine-dependent sleep apnea as follows: a supine apnea–hypopnea index ≥10, together with a lateral apnea–hypopnea index <10. In the study of Bignold et al. [29], when patients met the following criteria, they were deemed position-dependent: “overall AHI ≥15/h, supine AHI ≥ twice the non-supine AHI; ≥20 min of sleep in supine and non-supine postures and non-supine AHI <15.”
Sleep study with sleep position assessment and separate assessment for head and trunk
Sleep studies exist in many varieties, from very simple to very detailed. In order to determine whether a patient is position-dependent, it is clear that assessment of the sleep position is mandatory. In every OSA patient, the role of sleep position should be investigated. The role of sleep studies without sleep positional recording is therefore very limited. Ideally, both the mean AHI as well as the separate AHIs in supine, left, right, and prone sleep positions should be recorded. In the hypnogram, this is reflected by a clustering of respiratory events correlated with the change in body position.
Commonly, position sensors are attached to the elastic bands around either the chest or abdomen. Our group recently confirmed the hypothesis that the occurrence of OSA may also be dependent on the position of the head [30]. Study subjects underwent overnight polysomnography with two position sensors: one on the trunk and one in the mid-forehead. Overnight results based on the two different sensor positions show that the AHI calculated over the total sleep period with the head lying supine was frequently higher than the AHI calculated over the total period with the trunk in supine position. Over the time period when lying on the back with the head also supine, the AHI was significantly higher than during the time period with the head turned sideways. The use of dual position sensors could have major clinical and research implications [31]. In patients with a suspicion of position-dependent OSA, sleep recording with dual position sensors placed on both trunk and head should be considered.
Prevalence of position-dependent OSA and snoring
A considerable amount of literature exits on the role of sleep position in OSA [19–22, 25, 26, 30–37]. In studies from Israel and the Netherlands, a remarkable steady 56 % of patients with OSA have a difference of 50 % or more in the apnea index between the supine and non-supine positions [19–22]. An additional 30 % of patients have a higher AHI in the supine position than in the other positions, but not twice as high. On average, patients with POSA have a lower BMI and are younger than non-positional OSA patients [19, 22].
Reports have suggested that snoring is aggravated by a supine sleeping position [25, 38]. Nakano et al. [39] described the effect of position on snoring in 21 non-apneic (AHI < 15) and 51 apneic patients (AHI > 15). They conclude that “Snoring time as well as snoring intensity was lower in the lateral position than in the supine position in the non-apneic patients whilst in the apneic group neither snoring time nor intensity had statistical differences.” In non-apneic patients, the snoring time was 17.5 % and 6.4 % and the intensity 101.6 and 98.3 dB in the supine and non-supine positions, respectively. In the apneic group, the snoring time was 16.9 % and 15.4 % and the intensity 102.9 and 103.5 dB in the supine and non-supine positions, respectively.
Choi et al. [40] defined a position-dependent snorer as “one who has a greater than 50 % reduction of snoring rate in the lateral position compared to that in the supine position.” To our best knowledge, the prevalence of position-dependent snoring is yet to be reported.
Positional therapy
Positional therapy
PT can be defined as preventing patients to sleep in the worst sleeping position. The worst sleeping position is usually, but not always, the supine position [35]. Various techniques are described to prevent patients from assuming the supine position such as positional alarms, verbal instructions, tennis balls (TBT), vests, “shark fins,” or special pillows [7, 27, 29, 40–53].
The effect of positional therapy on snoring
Rationale
In 1948, Robin [17] stated that “many persons snore only when on their backs” and suggested that on some occasions, sewing a cotton reel into the back of a pyjama can be effective, albeit rather uncomfortable. The effect of PT on snoring can be measured from various angles: intensity (decibels), frequency (snores/hour), snoring rate (% TST), or duration (seconds or milliseconds).
Overview of evidence
Two studies specifically studied the effect of PT on snoring. In five studies evaluating the effect of PT on POSA, the result on snoring was also mentioned.
Braver and Block [54] reported that PT (foam rubber wedges both behind and in front of subject) was not effective in reducing snoring in 20 patients. The number of snores remained 356/hour both with and without PT.
Choi et al. [40] evaluated the efficacy of PT (vest with two inflatable chambers) to treat snoring in 17 positional-dependent snorers, defined as one who has a >50 % reduction of snoring rate in the lateral position compared with that in the supine position. The snoring rate decreased from 36.7 % to 15.7 % without subjective or objective adverse effects.
Maurer et al. [41] found an overall decrease in snoring time from 180 to 110 min in 12 apneic patients treated with PT (vest with semi-rigid foam in its dorsal part), but an increase was observed in 30 % of the patients. A statistically significant decrease in snoring was reported by Zuberi et al. [42] in 22 patients with POSA treated with PT (triangular pillow), whilst Wenzel et al. [43] reported a decrease in snoring rate from 15.4 % to 9.8 % in 14 patients with POSA treated with PT (vest). Loord and Hultcrantz [44] reported that half of the patients (n = 18) treated with PT (soft vest attached to a board with pillow) snored more frequently; specifically, six snored less frequently, nine snored more frequently, and for two, there was no difference. A recent study by Bignold et al. [29] reporting on the efficacy of the position monitoring and supine alarm device on 15 patients with supine-dependent OSA found no improvement in snoring. There was a trend for an overall reduction in snoring frequency, but this was not statistically significant. Furthermore, there was no difference in mean snore duration.
Conclusion
In non-apneic patients, snoring decreased when a patient adopted a non-supine position. In apneic patients, in the majority of studies, PT does not result in an improvement in snoring.
The effect of positional therapy on OSA
Overview of the evidence
A number of studies have examined the effect of PT on OSA [7]. Of the 23 relevant articles found, seven studies were excluded from the overview. Two studies did not provide information on the effect of PT on OSA parameters and were omitted from the overview [46, 47]. Five studies evaluated the effect on OSA of an array of devices resulting in an elevated posture and head extension [55–59]. As these devices did not prevent the patient from assuming the supine position, we did not include these studies in our review. An overview of the 16 included articles is presented in Table 2.
Various techniques are described to prevent patients from assuming the supine position, such as an upright sleep posture, positional alarms, verbal instructions, TBT, vests, “shark fins,” or special pillows [7, 27, 29, 40–53].
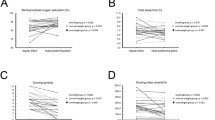
In an attempt to decrease discomfort and improve compliance, our group developed a new treatment concept: a small neck-worn vibrating device which prevents patients from applying a supine sleeping position [53]. When wearing the device, adopting a supine position triggers a vibration which increases in intensity until a new position is adopted, without significantly reducing total sleep time or disrupting sleep. Thirty patients with positional sleep apnea were included in a pilot study. No side effects were reported. The mean AHI dropped from 27.7 ± 2.4 to 12.8 ± 2.2. Seven patients developed an overall AHI below 5 when using the device in ON modus. Although the results are encouraging, several items remain to be addressed with this device, and there is room for improvement. The long-term effect remains to be studied.
Bignold et al. [29] evaluated the efficacy of a similar device in 15 patients fulfilling the following criteria: overall AHI ≥15 per hour, supine AHI twice or greater than the non-supine AHI; ≥20 min of sleep in supine and non-supine postures and non-supine AHI < 15. Subjects were assigned to receive the active PT or the inactive PT in a random order for a week followed by a 1-week washout before commencing the alternative treatment. The device consists of a position-monitoring and supine alarm device fastened to the chest. The mean baseline AHI (24.1) was reduced in the order of 45 % with active treatment.
Three publications studied the effect of PT compared to CPAP in a randomized crossover study setup. Jokic et al. [48] included 13 patients who were randomized to 2 weeks of treatment with nasal continuous positive pressure (nCPAP) or PT (backpack with softball) followed by a crossover to the other modality. They found “PT to be highly effective in reducing time spent in a supine position.” And although both treatment modalities were found to improve OSA severity, nCPAP was found to be more effective in reducing the AHI (17.9 to 3.4 on nCPAP, to 9.5 with PT).
Skinner et al. [51] included 20 patients in a randomized crossover comparing the efficacy of a thoracic anti-supine band (TASB) with nCPAP. Subjects were randomly assigned to receive the TASB or nCPAP for the first month followed by a 1-week washout before commencing the alternative treatment. The baseline AHI was 22.7 and was decreased to 12.0 with TASB and 4.9 with nCPAP. A successful treatment outcome was defined as an AHI < 10, which was achieved in 13 of 18 subjects when using TASB and in 16 of 18 subjects when using nCPAP. Once again, they found that the self-reported compliance was significantly better with TASB than with nCPAP. Nineteen of 20 patients reported a 7-h nightly use of the TASB, while only 9 of 20 patients managed to use their nCPAP at least 4 h per night.
The recent study by Permut et al. [27] showed that PT (a bulky mass strapped to the back) was equal to CPAP in normalizing the AHI in patients with a mild to moderate POSA. Only patients with a non-supine AHI of <5 were included. The long-term effect was not reported.
Conclusion
All studies report a positive effect of PT on the AHI. PT compliance is better than CPAP compliance, but the latter is a more effective treatment.
Positional therapy compliance
Even the most effective medical devices are only effective when they are used. Both CPAP and, to a lesser extent, MAD therapy are hampered by compliance issues [60–62].
Overview of the evidence
Skinner et al. [51] included 20 patients in a randomized crossover comparing the efficacy of TASB with nCPAP. Subjects were randomly assigned to receive TASB or nCPAP for the first month followed by a 1-week washout before commencing the alternative treatment. The self-reported compliance was significantly better with TASB than with nCPAP. Nineteen of 20 patients reported a 7-h nightly use with the TASB. In contrast, only 9 of 20 subjects met the 4-h per night CPAP compliance criteria.
Next to the efficacy study of PT (vest with semi-rigid foam on dorsal part) by Wenzel et al. [43], the group contacted the patients approximately 13.7 months later by telephone to assess PT compliance. Only 4 of the 14 patients were still using PT (on average for 7.3 h and 6.4 nights); their ESS was reduced from 8.5 to 6.5. The remaining 10 patients had stopped using PT due to the following reasons: discomfort and tightness of the vest, frequent awakenings, restless sleep, increased sweating during the night, and prevention of preferred sleeping position.
Oksenberg et al. [49] assessed the use of PT (TBT) during a 6-month period in 78 consecutive POSA patients. Of the 50 patients who returned the questionnaire, 38 % were still using PT, 24 % no longer used PT as they claimed to have learned to avoid the supine position, and 38 % no longer used PT, but had not learned to avoid the supine position.
Bignold et al. [50] studied the compliance of 67 patients, who had been prescribed PT (TBT) 2.5 ± 1 years earlier, using a follow-up questionnaire. Six percent were still using PT, 13.4 % no longer used PT as they claimed to have learned to avoid the supine position, and a staggering 80.6 % no longer used PT, but had not learned to avoid the supine position. Reasons to abort the PT included ineffectiveness, backache, discomfort, and no improvement in sleep quality or daytime alertness.
Of the nine patients randomized to PT (triangular pillow), in a study performed by Svatikova et al. [52], 3 months post-stroke, the self-reported adherence was: 3 (33 %) all nights, 1 (11 %) most nights, 2 (22 %) some nights, and 3 (33 %) no nights.
In a second study performed by Bignold et al. [29], patients were assigned with PT for 3 weeks (a position monitoring device and supine alarm device). The device was active for one of the 3 weeks. Patients used the device 85 % of nights over the full 3 weeks, with an average of 6.8 h of use per night.
It has been suggested that patients may learn to avoid the supine position following PT and therefore do not need to use PT on a regular basis [45]. Others may need PT either periodically to reinforce training or consistently.
Conclusion
Ineffectiveness, backache, discomfort, and no improvement in sleep quality or daytime alertness have been responsible for poor compliance and the subsequent disappointing long-term results of PT.
Can the effect of positional therapy be predicted from the sleep study?
Many different forms of sleep study are available, some simple and some more extensive. Some take sleep position into account; others do not. Most provide information on sleep position, time spent per position, and the AHI distribution per position. Some polysomnographies (PSGs) calculate the non-supine AHI; if not, the following formula can be used:
It remains to be studied what the predictive value of the non-supine AHI is. Can it be used to indicate when PT may be successful or to measure the expected effect of PT? Both Mador’s and Permut’s groups only included patients with an AHI of fewer than five events per hour while in the non-supine position [26, 27].
Sleep position and positional therapy in combination with sleep surgery
Rationale
As early as 1948, Robin [17] wrote: “sleeping on one’s back is considered a common cause of snoring, as the tongue falls back more readily.” He reasoned that “by changing the position of the head the tongue will be prevented from falling back,” Harper and Sauerland [63] suggested that “when sleep apnea patients sleep in supine position, the tongue tends to fall backward against the pharyngeal wall, due to gravity.” Our group recently reported that visualization of a base of tongue obstruction or epiglottis obstruction during DISE was more common in patients with POSA in comparison to patients with OSA (p = 0.058) [64].
These results suggest a trend: patients with POSA may require base of tongue level surgery more often than patients without positional dependence. Is this an overlooked cause of surgery failures?
Overview of the evidence
To our best knowledge, three papers have been written on the effect of sleep position on treatment outcomes of sleep surgery, the uvulopalatopharyngoplasty (UPPP).
Katsantonis et al. [65] studied the effect of UPPP on sleep posture and differences in UPPP results in various sleep positions in a small series of 17 patients. They found that following UPPP, the AHI significantly improved in the lateral position. They also found that during sleep in a supine position, the AHI did not show a significant improvement. They conclude that “UPPP enhances the position effect on OSA because it readily eliminates obstructive events in the lateral sleep position.” In other words, the difference in AHI in the supine and non-supine positions is more pronounced postoperatively. They are of the opinion “that additional PT could significantly improve response to treatment with UPPP.”
Lee et al. [66] studied the effect of sleep position on surgical outcomes as well. They studied 69 consecutive patients who underwent a UPPP. After categorizing the patients into four groups according to the change in AHI after surgery, they found that the failure group had a higher proportion of supine position dependency than any other group.
In a second paper published by the same group, the results show that UPPP is a successful treatment for obstructive events occurring in the lateral sleep position, especially in patients without positional dependency [67]. The suggestion is made that “patients who have become position dependent may benefit from PT after UPPP.”
A Korean study evaluated the changes of sleep positions before and after pharyngeal (UPPP or uvulopalatal flap or tonsillectomy) and/or nasal surgery (endoscopic sinus surgery and/or septoplasty and/or turbinoplasty) in 52 OSA patients with no response to surgery (n = 25) and with response to surgery (n = 28) [68]. Response was defined as a >50 % decrease in postoperative AHI. They concluded that “the frequency of positional changes was significantly decreased with the improvement of respiratory disturbances and arousals in the response group after surgery.”
Conclusion
All three papers conclude that UPPP is most successful in decreasing the AHI in the lateral position. In the supine position, following UPPP, the AHI shows no significant improvement. As the difference in AHI in the supine and non-supine positions is more pronounced postoperatively, UPPP enhances the position effect on OSA; therefore, additional PT could significantly improve response to treatment.
Sleep position and positional therapy in combination with an oral device
Overview of the evidence
Four papers were found which studied the treatment outcome of MAD therapy specifically in positional and non-positional OSA patients.
Cartwright [69] investigated factors associated with the effectiveness of an MAD on OSA in 16 male patients. Patients with position-dependent OSA were more responsive to MAD therapy than patients with non-position-dependent OSA. The presence of an increased severity of apneas in the supine posture was the strongest predictor of success.
Yoshida [70] studied the effect of an MAD in 72 patients according to sleep position. Forty-four patients exhibited apneas most frequently in the supine position, 15 in the lateral position, and 13 in the prone position. The baseline AHI was significantly lower in the prone group than in the lateral group or the supine group. In the supine group, the treatment was successful (defined as an AHI < 10) in 61.4 % of the patients, none in the lateral group, and 84.6 % in the prone group. Yoshida concluded that the effectiveness of an oral appliance is greatly influenced by sleep posture.
Marklund et al. [28], in a small series, found treatment success to be related to supine-dependent sleep apnea. Supine-dependent sleep apnea was defined when the supine apnea–hypopnea index was ≥10, in combination with a lateral apnea–hypopnea index of <10. In 12 patients with supine-dependent sleep apnea, an MAD reduced the supine apnea–hypopnea index from a median of 41 to 5.9. In 14 patients with non-supine-dependent sleep apnea, the treatment reduced the supine apnea–hypopnea index from 44 to 21 and the lateral apnea–hypopnea index from 21 to 4.5. The adjusted odds ratio for a successful apnea reduction to an apnea–hypopnea index of <10 in both the supine and the lateral positions was 30 for supine-dependent sleep apnea.
Chung et al. [71] studied 72 consecutive patients (42 patients with and 30 without position-dependent sleep apnea when applying Cartwright’s POSA criteria) who underwent a sleep study before and after the insertion of an MAD. They found that “patients with positional OSA had substantially better treatment outcomes than patients with non-positional OSA.” Both the decrease in overall and supine AHI was significantly greater in the positional OSA group.
The role of combination therapy—MAD with PT—remains to be further elucidated, but seems promising. Cartwright [46] showed that the “combined effect of PT and a tongue retaining device was better than one of the treatment modalities alone.” Sixty patients with an AHI of at least 12.5 were randomly assigned to either (1) MAD, (2) PT (positional alarm), or (3) combination therapy (MAD and PT). The AHI was reduced from 27.4 to 11.4 in group 1, from 33.3 to 20.8 in group 2, and from 30.7 to 7.9 in group 3.
Conclusion
In brief, they all conclude that MADs are more effective in patients with positional OSA than in patients without positional OSA. The role of combination therapy remains to be further elucidated.
Sleep position and positional therapy in combination with CPAP
As mentioned, CPAP compliance is often poor. One of the many reasons for CPAP failure and non-compliance is high CPAP pressure.
Overview of the literature
In a retrospective study by Pevernagie and Shephard [72], patients diagnosed with OSAS returned for a second overnight sleep study, during which nCPAP was titrated up to a level that eliminated SDB events and snoring in the supine position. Thirty-one patients who had sufficient sleep time in NREM and REM sleep in both supine and non-supine sleep postures were included. They found that “patients with positional sleep apnea required less positive airway pressure, than non-positionals, as well as a tendency to avoid sleeping on the back in direct proportion to the severity of their OSA in that position.”
In contrast, in a small-scale study, Sériès and Marc [73] concluded that CPAP compliance improved with auto-CPAP therapy in patients with sleep stage- and/or body position-dependent nocturnal breathing disorders compared to fixed CPAP. The effective pressure/time index was significantly lower in sleep stage- and body position-dependent patients treated with fixed CPAP than in the other patients.
Oksenberg et al. [74] concluded in a retrospective study of 83 consecutive patients undergoing nCPAP titration that the optimal nCPAP level was significantly higher in the supine position than it was in the lateral position.
Body position and sleep stage have been shown to significantly influence the positive pressure level needed to treat obstructive breathing abnormalities. Pressure level requirements may vary over time due to several factors such as weight loss or gain, medication and alcohol use, nasal congestion, changes in jaw position (due to an MAD for example), duration of CPAP therapy (CPAP is thought to play a role in reducing edema resulting from snoring-associated vibration and apnea-induced suction of the upper airway), the cyclic alternating pattern of sleep stages, or body position [60, 72–74].
Conclusion
Most studies suggest that patients’ positive pressure needed in the supine position is greater than that needed in the non-supine position. Therefore, patients benefit from auto-CPAP, with a consequent increase in compliance.
PT could theoretically be of value. The treatment of OSA is a stepwise approach. If a patient with supine-dependent OSA can avoid the supine position, the consequent decrease in AHI and positive pressure requirements results in less aggressive treatment, improving tolerance and compliance [75].
Sleep position and nasal expiratory device
One study was found to have examined the effect of sleep position on the efficacy of the novel treatment: the nasal expiratory resistor device (nEPAP) [76]. Twenty subjects with OSA were included in the study who underwent PSG while wearing the therapy. The results suggest that patients with position-dependent SDB (defined as a supine AHI greater than the lateral AHI) were more likely to have an acceptable therapeutic response to nEPAP, although the results did not reach statistical significance.
Discussion and future perspectives
Unfortunately, research on the effect of PT on POSA lacks good clinical trials, a miss in OSA research in general. Not all articles included in this paper specify definitions and cutoff values used to rule in OSA. In 1999, the American Academy of Sleep Medicine Task Force introduced evidence-based standardized scoring guidelines and cutoff values for OSA. Studies discussed in this paper may have applied different definitions, especially if performed before 1999 [23].
At present, evidence of PT effectiveness is based on small-scale case series and a few randomized trials. Little is known about the long-term compliance of PT and the actual ability of patients to learn to avoid the supine position following PT treatment.
There is room for technical improvement of the devices to reduce discomfort and consequent disruption of sleep architecture as to improve compliance.
POSA is commonly defined as a difference of 50 % or more in apnea index between supine and non-supine positions, but many question Cartwright’s criteria and apply adapted versions. Similar issues have faced CPAP compliance criteria and surgical and MAD success definitions [60]. CPAP therapy is regarded as successful if the AHI drops below 5 when CPAP is used. Current trends define compliance as 4 h per night as an average over all nights observed [61].
Surgical success was originally defined by Sher et al. [77] as an AHI reduction of at least 50 % and an AHI reduction to below 20.
Others have later proposed to tighten surgical success criteria to a postoperative AHI below 15 (regarded as “clinically relevant” OSA), below 10, and, recently, even below 5 [78]. Patients in whom the AHI is reduced by 20–50 % are classified as responders [12].
PT of OSA now commonly aims to arouse the patient when lying on the back so the subject rotates the body on his/her side to alleviate respiratory obstructions. In head position-aggravated trunk supine position-dependent OSA, it may be sufficient to stimulate the subject to rotate only the head sideways based on a position sensor monitoring the orientation of the head. It can be expected that this would have a much less profound negative effect on sleep quality.
Conclusion
Research performed in the past 10–20 years show that PT has a significant influence on AHI. These studies are predominantly performed as case series on a comparably small number of patients. Still, results have not found their way into the daily diagnostic and treatment routine. An approximate 56 % of patients with OSA have position-dependent OSA commonly defined as a difference of 50 % or more in apnea index between supine and non-supine positions. A great deal is to be gained from treating patients with POSA with PT. PT, often simple and inexpensive, shows promise as a stand-alone treatment or as an additional measure to increase the success rate of other established treatment methods. Treating body position should receive more attention in the treatment of sleep apnea. Long-term compliance for PT remains an issue, and although remarkable results have been shown using innovative treatment concepts for PT, there is room for both technical improvement of the devices used and for further research.
Abbreviations
- AHI:
-
Apnea–hypopnea index
- AI:
-
Apnea index
- BMI:
-
Body mass index
- BS:
-
Bariatric surgery
- OSA:
-
Obstructive sleep apnea
- CPAP:
-
Continuous positive pressure
- DISE:
-
Drug-induced sleep endoscopy
- ESS:
-
Epworth Sleepiness Scale
- nCPAP:
-
Nasal continuous positive pressure
- MAD:
-
Mandibular advancement device
- POSA:
-
Positional obstructive sleep apnea
- PSG:
-
Polysomnography
- PT:
-
Positional therapy
- SaO2 :
-
Oxygen saturation
- TBT:
-
Tennis ball technique
- UPPP:
-
Uvulopalatopharyngoplasty
References
Kryger MH (2000) Diagnosis and management of sleep apnea syndrome. Clin Cornerstone 2:39–47
Young T, Hutton R, Finn L, Baddr S, Palta M (1996) The gender basis in sleep apnea diagnosis: are women missed because they have different symptoms? Arch Intern Med 156:2445–2451
Young T, Finn L, Peppard PE, Szklo-Coxe M, Austin D, Nieto FJ, Stubbs R, Hla KM (2008) Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 31:1071–1078
Redline S, Yenokyan G, Gottlieb DJ, Shahar E, O’Connor GT, Resnick HE, Diener-West M, Sanders MH, Wolf PA, Geraghty EM, Ali T, Lebowitz M, Punjabi NM (2010) Obstructive sleep apnea–hypopnea and incident stroke: the Sleep Heart Health Study. Am J Respir Crit Care Med 182:269–277
Findley LJ, Weiss JW, Jabour ER (1991) Drivers with untreated sleep apnea. A cause of death and serious injury. Arch Intern Med 151:1451–1452
Smolensky MH, Di Milia L, Ohayon MM, Philip P (2011) Sleep disorders, medical conditions, and road accident risk. Accid Anal Prev 43:533–548
Randerath WJ, Verbraecken J, Andreas S, Bettega G, Boudewyns A, Hamans E, Jalbert F, Paoli JR, Sanner B, Smith I, Stuck BA, Lacassagne L, Marklund M, Maurer JT, Pepin JL, Valipour A, Verse T, Fietze I (2011) European Respiratory Society task force on non-CPAP therapies in sleep apnoea. Non-CPAP therapies in obstructive sleep apnoea. Eur Respir J 37:1000–1028
Weaver TE, Grunstein RR (2008) Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc 5:173–178
Richard W, Venker J, den Herder C, Kox D, van den Berg B, Laman M, van Tinteren H, de Vries N (2007) Acceptance and long-term compliance of nCPAP in obstructive sleep apnea. Eur Arch Otorhinolaryngol 264:1081–1086
Woodson BT (2008) Structural effectiveness of pharyngeal sleep apnea surgery. Sleep Med Rev 12:463–479
Kezirian EJ, Goldberg AN (2006) Hypopharyngeal surgery in obstructive sleep apnea: an evidence-based medicine review. Arch Otolaryngol Head Neck Surg 132:206–213
Richard W, Kox D, den Herder C, van Tinteren H, de Vries N (2007) One stage multilevel surgery (uvulopalatopharyngoplasty, hyoid suspension, radiofrequent ablation of the tongue base with/without genioglossus advancement), in obstructive sleep apnea syndrome. Eur Arch Otorhinolaryngol 264:439–444
Benazzo M, Pagella F, Matti E, Zorzi S, Campanini A, Frassineti S, Montevecchi F, Tinelli C, Vicini C (2008) Hyoidthyroidpexia as a treatment in multilevel surgery for obstructive sleep apnea. Acta Otolaryngol 128:680–684
Van den Broek E, Richard W, van Tinteren H, de Vries N (2008) UPPP combined with radiofrequency thermotherapy of the tongue base for the treatment of obstructive sleep apnea syndrome. Eur Arch Otorhinolaryngol 265:1361–1365
Yi HL, Sun XQ, Chen B, Zhang YJ, Guan J, Wu HM, Meng LL, Yin SK (2011) Z-palatopharyngoplasty plus genioglossus advancement and hyoid suspension for obstructive sleep apnea hypopnea syndrome. Otolaryngol Head Neck Surg 144:469–473
Greenburg Lettieri CJ, Eliasson AH (2009) Effects of surgical weight loss on measures of obstructive sleep apnea: a meta-analysis. Am J Med 122:535–542
Robin I (1948) Snoring. Proc R Soc Med 41:151–153
Editor’s note (1984) Patient’s wife cures his snoring. Chest 85:582
Oksenberg A, Silverberg DS, Arons E, Radwan H (1997) Positional vs nonpositional obstructive sleep apnea patients. Chest 112:629–639
Oksenberg A, Khamaysi I, Silverberg DS, Tarasiuk A (2000) Association of body position with severity of apneic events in patients with severe nonpositional obstructive sleep apnea. Chest 118:1018–1024
Oksenberg A, Arons E, Greenberg-Dotan S, Nasser K, Radwan H (2009) The significance of body posture on breathing abnormalities during sleep: data analysis of 2077 obstructive sleep apnea patients. Harefuah 148:304–309
Richard W, Kox D, den Herder C, Laman M, van Tinteren H, de Vries N (2006) The role of sleeping position in obstructive sleep apnea. Eur Arch Otorhinolaryngol 263:946–950
American Academy of Sleep Medicine Task Force (1999) Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American. Sleep 22:667–689
American Academy of Sleep Medicine (2005) The international classification of sleep disorders: diagnostic and coding manual, 2nd edn. American Academy of Sleep Medicine, Westchester
Cartwright RD (1984) Effect of sleep position on sleep apnea severity. Sleep 7:110–114
Mador MJ, Kufel TJ, Magalang UJ, Rajesh SK, WatweV GBJB (2005) Prevalence of positional sleep apnea in patients undergoing polysomnography. Chest 128:2130–2137
Permut I, Diaz-Abad M, Chatila W, Crocetti J, Gaughan JP, D’Alonzo GE, Krachman SL (2010) Comparison of positional therapy to CPAP in patients with positional obstructive sleep apnea. J Clin Sleep Med 6:238–243
Marklund M, Persson M, Franklin KA (1998) Treatment success with an mandibular advancement device is related to supine-dependent sleep apnea. Chest 114:1630–1635
Bignold JJ, Mercer JD, Antic NA, McEvoy RD, Catcheside PG (2011) Accurate position monitoring and improved supine-dependent obstructive sleep apnea with a new position recording and supine avoidance device. J Clin Sleep Med 7:376–383
Van Kesteren ER, van Maanen JP, Hilgevoord AA, Laman DM, de Vries N (2011) Quantitative effects of trunk and head position on the apnea hypopnea index in obstructive sleep apnea. Sleep 34:1075–1081
Schwab R (2011) A quantum advance in PSG recordings: the importance of head position in mediating the AHI. Sleep 34(8):985–986
Kavey NB, Blitzer A, Gidro-Frank S, Korstanje K (1985) Sleeping position and sleep apnea syndrome. Am J Otolaryngol 6:373–377
Chaudhary BA, Chaudhary TK, Kolbeck RC, Harmon JD, Speir WA (1986) Therapeutic effect of posture in sleep apnea. South Med J 79:1061–1062
George CF, Millar TW, Kryger MH (1988) Sleep apnea and body position during sleep. Sleep 11:90–99
Cartwright RD, Diaz F, Lloyd S (1991) The effect of sleep posture and sleep stage on apnea frequency. Sleep 14:351–353
Itasaka Y, Miyazaki S, Ishikawa K, Togawa K (2000) The influence of sleep position and obesity on sleep apnea. Psychiatry Clin Neurosci 54:340–341
Akita Y, Kawakatsu K, Hattori C, Hattori H, Suzuki K, Nishimura T (2003) Posture of patients with sleep apnea during sleep. Acta Otolaryngol Suppl 550:41–45
Hoffstein V (1996) Snoring. Chest 109:201–222
Nakano H, Ikeda T, Hayashi M, Ohshima E, Onizuka A (2003) Effects of body position on snoring in apneic and nonapneic snorers. Sleep 26:169–172
Choi JH, Park TY, Hong JH, Kim SJ, Park DS, Miyazaki S, Lee SH, Shin C, Lee J (2009) Efficacy study of a vest-type device for positional therapy in position dependent snorers. Sleep Biol Rythms 7:181–187
Maurer JT, Stuck BA, Hein G, Verse T, Hörmann K (2003) Schlafapnoetherapie mit einer neuartigen rückenlage-verhinderungs-weste. Dtsch Med Wochenschr v128:71–75
Zuberi NA, Rekab K, Nguyen HV (2004) Sleep apnea avoidance pillow effects on obstructive sleep apnea syndrome and snoring. Sleep Breath 8:201–207
Wenzel S, Smith E, Leiacker R, Fischer Y (2007) Efficacy and long-term compliance of the vest preventing the supine position in patients with obstructive sleep apnea. Laryngorhinootologie 86:579–583
Loord H, Hultcrantz E (2007) Positioner—a method for preventing sleep apnea. Acta Otolaryngol 127:861–868
Cartwright RD, Lloyd S, Lilie J, Kravtiz H (1985) Sleep position training as treatment for sleep apnea syndrome: a preliminary study. Sleep 8:87–94
Cartwright RD, Ristanovic R, Diaz F, Caldarelli D, Alder G (1991) A comparative study of treatments for positional sleep apnea. Sleep 14:546–552
Berger M, Oksenberg A, Silverberg DS, Arons E, Radwan H, Iaina A (1997) Avoiding the supine position during sleep lowers 24 h blood pressure in obstructive sleep apnea (OSA) patients. J Hum Hypertens 11:657–664
Jokic R, Klimaszewski A, Crossley M, Sridhar G, Fitzpatrick MF (1999) Positional treatment vs continuous positive airway pressure in patients with positional obstructive sleep apnea syndrome. Chest 115:771–781
Oksenberg A, Silverberg D, Offenbach D, Arons E (2006) Positional therapy for obstructive sleep apnea patients: a 6-month follow-up study. Laryngoscope 116:1995–2000
Bignold JJ, Deans-Costi G, Goldsworthy MR, Robertson CA, McEvoy D, Catcheside PG, Mercer JD (2009) Poor long-term patient compliance with the tennis ball technique for treating positional obstructive sleep apnea. J Clin Sleep Med 5:428–430
Skinner MA, Kingshott RN, Filsell S, Taylor R (2009) Efficacy of the ‘tennis ball technique’ versus nCPAP in the management of position-dependent obstructive sleep apnoea syndrome. Respirology 13:708–715
Svatikova A, Chervin RD, Wing JJ, Sanchez BN, Migda EM, Brown DL (2011) Positional therapy in ischemic stroke patients with obstructive sleep apnea. Sleep Med 12:262–266
Van Maanen JP, Richard W, van Kesteren ER, Ravesloot MJL, Laman DM, Hilgevoord AAJ, de Vries N (2011) Evaluation of a new simple treatment for positional sleep apnea patients. J Sleep Res. doi:10.1111/j.1365-2869.2011.00974.x
Braver HM, Block J (1994) Effect of nasal spray, positional therapy, and the combination thereof in the asymptomatic snorer. Sleep 17:516–521
McEvoy RD, Sharp DJ, Thornton AT (1986) The effects of posture on obstructive sleep apnea. Am Rev Respir Dis 133:662–666
Kushida CA, Rao S, Guilleminault C, Giraudo S, Hsieh J, Hyde P, Dement WC (1999) Cervical positional effects on snoring and apneas. Sleep Res Online 2:7–10
Kushida CA, Sherrill CM, Hong SC, Palombini L, Hyde P, Dement WC (2001) Cervical positioning for reduction of sleep-disordered breathing in mild-to-moderate OSAS. Sleep Breath 5:71–78
Skinner MA, Kingshott RN, Jones DR, Taylor DR (2004) Lack of efficacy for a cervicomandibular support collar in the management of obstructive sleep apnea. Chest 125:118–126
Skinner MA, Kingshott RN, Jones DR, Homan SD, Taylor DR (2004) Elevated posture for the management of obstructive sleep apnea. Sleep Breath 8:193–200
Ravesloot MJL, de Vries N (2011) Reliable calculation of the efficacy of non-surgical and surgical treatment of obstructive sleep apnea revisited. Sleep 34:105–110
Kribbs NB, Pack AI, Kline LR, Smith PL, Schwartz AR, Schubert NM, Redline S, Henry JN, Getsy JE, Dinges DF (1993) Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am J Respir Crit Care Med 147:887–895
Petit F, Pepin J, Bettega G, Sadek H, Raphael B, Levy P (2002) Mandibular advancement devices: rate of contraindications in 100 consecutive obstructive sleep apnea patients. Am J Respir Crit Care Med 166:274–278
Harper R, Sauerland E (1978) The role of the tongue in sleep apnea. In: Guilleminault C, Dement W (eds) Sleep apnea syndromes. Alan R. Liss, New York, pp 219–234
Ravesloot MJL, de Vries N (2011) 100 consecutive patients undergoing drug-induced sleep endoscopy—results and evaluation. Laryngoscope 121:2710–2716
Katsantonis GP, Miyazaki S, Walsh J (1990) Effects of uvulopalatopharyngoplasty on sleep architecture and patterns of obstructed breathing. Laryngoscope 10:1068–1072
Lee CH, Shin HW, Han DH, Mo JH, Yoon IY, Chung S, Choi HG, Kim JW (2009) The implication of sleep position in the evaluation of surgical outcomes in obstructive sleep apnea. Otol Head Neck Surg 140:531–535
Lee CH, Kim SW, Han K, Shin JM, Hong SL, Lee JE, Rhee CS, Kim JW (2011) Effect of uvulopalatopharyngoplasty on positional dependency in obstructive sleep apnea. Arch Otolaryngol Head Neck Surg 137:675–679
Choi JH, Kim EJ, Choi J, Kwon SY, Lee HM, Kim TH, Lee SH, Shin C, Lee SH (2011) Effect of successful surgical treatment on changes of position during sleep in adults with obstructive sleep apnea syndrome. Ann Otol Rhinol Laryngol 120:104–109
Cartwright RD (1985) Predicting response to the tongue retaining device for sleep apnea syndrome. Arch Otolaryngol 111:385–388
Yoshida K (2001) Influence of sleep posture on response to oral appliance therapy for sleep apnea syndrome. Sleep 24:538–544
Chung JW, Enciso R, Levendowski DJ, Morgan TD, Westbrook PR, Clark GT (2010) Treatment outcomes of mandibular advancement devices in positional and nonpositional OSA patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 109:724–731
Pevernagie DJ, Shepard JW (1992) Relations between sleep stage, posture and effective nasal CPAP levels in OSA. Sleep 15:162–167
Sériès F, Marc I (2001) Importance of sleep stage- and body position-dependence of sleep apnoea in determining benefits to auto-CPAP therapy. Eur Respir J 18:170–175
Oksenberg A, Silverberg DS, Arons E, Radwan H (1999) The sleep supine position has a major effect on optimal nasal continuous positive airway pressure. Chest 116:1000–1006
Lankford AD, Proctor CD, Richard R (2005) Continuous positive airway pressure changes in bariatric surgery patients undergoing rapid weight loss. Obes Surg 15:336–341
Patel AV, Hwang D, Masdeu MJ, Chen GM, Rapoport DM, Ayappa I (2011) Predictors of response to a nasal expiratory resistor device and its potential mechanisms of action for treatment of obstructive sleep apnea. J Clin Sleep Med 7:13–22
Sher AE, Schechtman KB, Piccirillo JF (1996) The efficacy of surgical modifications of the upper airway in adults with obstructive sleep apnea syndrome. Sleep 19:156–177
Elshaug AG, Moss JR, Southcott AM, Hiller JE (2007) Redefining success in airway surgery for obstructive sleep apnea: a meta analysis and synthesis of the evidence. Sleep 30:461–467
Conflict of interest statement
None of the authors have any conflict of interest regarding the material discussed in this manuscript.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Ravesloot, M.J.L., van Maanen, J.P., Dun, L. et al. The undervalued potential of positional therapy in position-dependent snoring and obstructive sleep apnea—a review of the literature. Sleep Breath 17, 39–49 (2013). https://doi.org/10.1007/s11325-012-0683-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-012-0683-5