
Abstract
Purpose
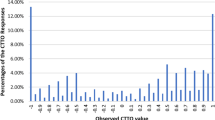
The EuroQol Valuation Technology (EQ-VT) uses traditional time trade-off (tTTO) for health states better than dead and lead-time TTO (LT-TTO) for states worse than dead to elicit a value (−1.0 to +1.0) for each health state. In the Canadian EQ-5D-5L Valuation study which used the EQVT platform, we observed an unexpected peak in frequency of “0” values and few negative values, particularly in the range of 0 to −0.5. To better understand this finding, we sought to explore respondents’ thought processes while valuing a health state, and their understanding of the tTTO and LT-TTO exercises.
Methods
Qualitative semi-structured interviews were conducted with EQVT task respondents. Questions focused on valuations of health states as: (a) Same as dead in tTTO, (b) Worse than dead in tTTO but changed to same as dead in LT-TTO, (c) Worse than dead in LT-TTO, and (d) Worse than dead in LT-TTO with trading off all 10 years. Data were analyzed using content and thematic analysis.
Results
Mean age of participants (N = 70) was 40 ± 18.1 years, 60 % female, and 76 % Caucasian. Participants provided similar reasons for valuing a health state same as or worse than dead. Many participants expressed confusion about worse than dead valuations, distinction between same as and worse than dead, and the transition from tTTO to LT-TTO. A few indicated that the addition of 10 years of full health in the LT-TTO influenced their valuations.
Conclusions
The transition from tTTO to LT-TTO in the EQVT was confusing to participants, whereby some health state valuations around this transition appeared to be arbitrary.

Similar content being viewed by others


References
Torrance, G. W. (1986). Measurement of health state utilities for economic appraisal: A review. Journal of Health Economics, 5, 1–30.
Devlin, N. J., Tsuchiya, A., Buckingham, K., & Tilling, C. (2011). A uniform time trade off method for states better and worse than dead: Feasibility study of the ‘lead time’ approach. Health Economics, 20(3), 348–361.
Attema, A. E., Versteegh, M. M., Oppe, M., Brouwer, W. B., & Stolk, E. A. (2013). Lead time TTO: Leading to better health state valuations? Health Economics, 22(4), 376–392.
Augustovski, F., Rey-Ares, L., Irazola, V., Oppe, M., & Devlin, N. J. (2013). Lead versus lag-time trade-off variants: Does it make any difference? The European Journal of Health Economics, 14(Suppl 1), S25–S31.
Tilling, C., Devlin, N., Tsuchiya, A., & Buckingham, K. (2010). Protocols for time tradeoff valuations of health states worse than dead: A literature review. Medical Decision Making, 30(5), 610–619.
Xie, F., Pullenayegum, E., Gaebel, K., Bansback, N., Bryan, B., Ohinmaa, A., et al. A time trade-off-derived value set of EQ-5D-5L for Canada. Medical Care (in press).
Oppe, M., Devlin, N. J., van Hout, B., Krabbe, P. F. M., & de Charro, F. (2014). A programme of methodological research to arrive at the new international EQ-5D-5L valuation protocol. Value Health, 17(4), 445–453.
Dolan, P., & Roberts, J. (2002). To what extent can we explain time trade-off values from other information about respondents. Social Science and Medicine, 54, 919–929.
San Miguel, F., Ryan, M., & Amaya-Amaya, M. (2005). ‘Irrational’ stated preferences: A quantitative and qualitative investigation. Health Economics, 14, 307–322.
Mulhern, B., Tsuchiya, A., Brazier, J., & Rowen, D. (2012). How do respondents perceive health state valuation exercises? A ‘think aloud’ study investigating time trade off and discrete choice experiments. Paper for presentation at EuroQol Plenary 2012.
Jansen, S. J., Stiggelbout, A. M., Wakker, P, P., Nooij, M. A., Noordijk, E. M., & Kievit, J. (2000). Unstable preferences: A shift in valuation or an effect of the elicitation procedure. Medical Decision Making, 20(1), 62–71.
Macran, S., & Kind, P. (2001). “Death” and the valuation of health-related quality of life. Medical Care, 39(3), 217–227.
Mulhern, B., Longworth, L., Brazier, J., Rowen, D., Bansback, N., Devlin, N., et al. (2013). Binary choice health state valuation and mode of administration: head-to-head comparison of online and CAPI. Value Health, 16(1), 104–113.
Edelaar-Peeters, Stiggelbout, A. M., & Van Den Hout, W. B. (2014). Qualitative and quantitative analysis of interviewer help answering the time tradeoff. Medical Decision Making, 34(5), 655–665.
Devlin, N. J., Hansen, P., & Selai, C. (2004). Understanding health state valuations: A qualitative analysis of respondents’ comments. Quality of Life Research, 13(7), 1265–1277.
Stalmeier, P. F., Busschbach, J. J., Lamers, L. M., & Krabbe, P. F. (2005). The gap effect: Discontinuities of preferences around dead. Health Economics, 14(7), 679–685.
Xie, F., Pullenayegum, E., Li, H., Al Sayah, F., Gaebel, K., Ohinmaa, A., et al. Too easy to be reliable? Test-retest reliability of the TTO and DCE tasks in the EuroQol Group Valuation Technology (under review).
Herdman, M., Gudex, C., Lloyd, A., Janssen, M., Kind, P., Parkin, D., et al. (2011). Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality of Life Research, 20(10), 1727–1736.
Janssen, B. M., Oppe, M., Versteegh, M. M., & Stolk, E. A. (2013). Introducing the composite time trade-off: A test of feasibility and face validity. The European Journal of Health Economics, 14(Suppl 1), S5–S13.
Hsieh, H. F., & Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qualitative Health Research, 15(9), 1277–1288.
Fereday, J., & Muir-Cochrane, E. (2005). Demonstrating rigor using thematic analysis: A hybrid approach of inductive and deductive coding and theme development. International Journal of Qualitative Methods, 5(1), 81–92.
QSR International Pty Ltd. NVivo qualitative data analysis software. 10 ed2012.
Ryan, M., Watson, V., & Entwistle, V. (2009). Rationalising the ‘irrational’: A think aloud study of discrete choice experiment responses. Health Economics, 18(3), 321–336.
Luo, N., Li, M., Stolk, E. A., & Devlin, N. J. (2013). The effects of lead time and visual aids in TTO valuation: A study of the EQ-VT framework. The European Journal of Health Economics, 14(Suppl 1), S15–S24.
Acknowledgments
We thank the EuroQol Research Foundation and the Valuation Task force of the EuroQol group for their support throughout conducting this study.
Funding
This study was funded by a research grant from the EuroQol Research Foundation. Feng Xie is supported through CIHR New Investigator Award (2012–2017). Jeffrey Johnson is a Senior Health Scholar with Alberta Innovates Health Solutions (2009–2016).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
FX and JAJ are members of the EuroQol Group. JAJ is a member of the Board of the EuroQol Research Foundation.
Appendix: Interview guide
Appendix: Interview guide
General questions for all participants:
-
1.
Did you find it hard to imagine the health states shown to you during the tasks you just completed? Why did you (or did you not) have difficulty imagining the health states?
-
2.
What was going through your mind while you were making your choices? (Did you imagine what your life would be like living in the health states or how it would affect your family/friends, etc.)
-
3.
Were you thinking about all the dimensions together or did one or two dimensions drive your decisions? Why?
-
4.
Did you find it difficult to trade off years of life for better quality of life? Why did you (did you not) have difficulty making those trade-offs?
-
5.
Do you believe there is some situation or condition that could be perceived as worse than dead? Can you describe to me a situation that you feel is “worse than dead”?
Specific questions based on participants’ responses:
-
For participants that did not trade any years for any health states other than the very mild ones: The health state seems worse than full health. Why were you not willing to trade off any years of live in order to live in full health?
-
For participants that were willing to trade a few years (0 < n < 10 years) to avoid a 10 year life with the health state: You were willing to trade years of life to avoid living 10 years in the health state. What are you thinking about when you were making your decision?
-
For participants that chose “the same” at 0 years (health state is the same as being dead): When you think Health State A at 0 year is about the same as Health State B at 10 years, did you realize that would mean Health State B is equal to being dead? What about the health state that made you think it is the same as being dead?
-
For participants that choose the WTD option but then did not trade anymore time (final score at 0): You chose Health State A at 0 year instead of living in Health State B for 10 years, indicating that you think Health State B is worse than being dead (show the screenshot below to the participant). Then the screen was changed to attach a 10-year in full health before living in these two health states (show the screenshot below to the participant). After you saw this screen, you chose the Health States A and B are about the same, meaning that Health State B is equal to being dead (your previous answer was that Health State B is worse than being dead). What made you change your response about Health State B?
-
For participants who traded years under the WTD scenario: The health state is so bad in your opinion that you are willing to trade 15 years of a 20 year life to avoid living with the health state? What are you thinking about when you were making your decision?
-
For participants that traded all of the 20 years away: The health state is so bad in your opinion that you are willing to trade all 20 years of life to avoid living with the health state? What are you thinking about when you were making your decision? Would you still be willing to trade off more years, if available, to avoid living in this bad health state?
Rights and permissions
About this article

Cite this article
Al Sayah, F., Mladenovic, A., Gaebel, K. et al. How dead is dead? Qualitative findings from participants of combined traditional and lead-time time trade-off valuations. Qual Life Res 25, 35–43 (2016). https://doi.org/10.1007/s11136-015-1073-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-015-1073-9