
Abstract
Purpose
Adenosine infusion during atrial fibrillation ablation is often used to evaluate for dormant pulmonary vein (PV) conduction. Several physiologic effects of adenosine may be seen during infusion, including atrioventricular (AV) block, hypotension, sinus tachycardia (as a reflex mechanism), and sinus bradycardia. However, hypotension and sinus tachycardia may be seen in the absence of AV block. Whether the dose required to achieve AV block versus any physiologic effect (e.g., hypotension) is relevant when evaluating for PV reconnection is unclear.
Methods
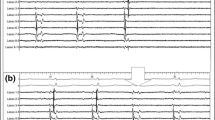
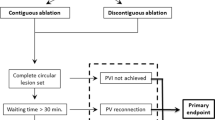
In consecutive patients undergoing first-time atrial fibrillation radiofrequency ablation for persistent or paroxysmal atrial fibrillation, adenosine testing was performed 30 min after successful PV isolation. When testing each PV after isolation, a circular mapping catheter was placed at the ostium and a 12-mg bolus of adenosine was given via peripheral line. The presence of some physiologic effect (e.g., sinus tachycardia or hypotension) versus AV block was recorded as was PV reconnection. If no AV block and no PV reconnection were seen, the dose was escalated by 6-mg increments to assess for PV reconnection until AV block or PV reconnection was achieved.
Results
Among 50 patients, there were 3 to 5 PVs isolated (median 4; mean 4.4). In 35 patients, a 12-mg bolus resulted in AV block and 16/155 (10 %) veins exhibited reconnection requiring additional ablation. In all other patients, sinus tachycardia and hypotension were seen in response to 12-mg infusion but no AV block and no PV reconnection was seen. No sinus bradycardia was seen in any patients. In 10/15 patients without AV block with 12 mg, 18 mg of adenosine was sufficient to achieve AV block and 5/43 (12 %) PVs exhibited reconnection. Among the remaining 5 patients, 3 patients required a dose of 24 mg to achieve AV block, and PV reconnection was seen in 1/14 (7 %) PVs. The remaining two patients required a dose of 30 mg to achieve AV block, but no PV reconnection was seen. There was no difference in symptomatic recurrence rate between those who exhibited adenosine-induced reconnection and those who did not after 1-year follow-up.
Conclusion
A fixed dose of adenosine may be insufficient to assess for PV reconnection. Furthermore, the presence of a physiologic effect (e.g., sinus tachycardia or hypotension) in the absence of AV block may reflect an insufficient dose. The dose needed may vary between patients, and AV block may reflect a minimal requirement when administering adenosine to assess for PV reconnection.


Similar content being viewed by others

References
January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association task force on practice guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014;64:e1–e76.
Sauer WH, McKernan ML, Lin D, Gerstenfeld EP, Callans DJ, Marchlinski FE. Clinical predictors and outcomes associated with acute return of pulmonary vein conduction during pulmonary vein isolation for treatment of atrial fibrillation. Heart Rhythm. 2006;3:1024–8.
Lin D, Santangeli P, Zado ES, Bala R, Hutchinson MD, Riley MP, et al. Electrophysiologic findings and long-term outcomes in patients undergoing third or more catheter ablation procedures for atrial fibrillation. J Cardiovasc Electrophysiol. 2015;26:371–7.
Arujuna A, Karim R, Caulfield D, Knowles B, Rhode K, Schaeffter T, et al. Acute pulmonary vein isolation is achieved by a combination of reversible and irreversible atrial injury after catheter ablation: evidence from magnetic resonance imaging. Circ Arrhythm Electrophysiol. 2012;5:691–700.
Kowalski M, Grimes MM, Perez FJ, Kenigsberg DN, Koneru J, Kasirajan V, et al. Histopathologic characterization of chronic radiofrequency ablation lesions for pulmonary vein isolation. J Am Coll Cardiol. 2012;59:930–8.
Macle L, Khairy P, Weerasooriya R, Novak P, Verma A, Willems S, et al. Adenosine-guided pulmonary vein isolation for the treatment of paroxysmal atrial fibrillation: an international, multicenter, randomized superiority trial. Lancet. 2015;386:672–9.
Kumar N, Dinh T, Phan K, Timmermans C, Philippens S, Dassen W, et al. Adenosine testing after second-generation cryoballoon ablation (ATSCA) study improves clinical success rate for atrial fibrillation. Europace. 2015;17:871–6.
Ghanbari H, Jani R, Hussain-Amin A, Al-Assad W, Huether E, Ansari S, et al. Role of adenosine after antral pulmonary vein isolation of paroxysmal atrial fibrillation: a randomized controlled trial. Heart Rhythm. 2016;13:407–15.
Kobori A, Shizuta S, Inoue K, Kaitani K, Morimoto T, Nazakawa Y, et al. Adenosine triphosphate-guided pulmonary vein isolation for atrial fibrillation: the unmasking dormant electrical reconduction by adenosine triphosphate (UNDER-ATP) trial. Eur Heart J. 2015;36:3276–87.
Drury AN, Szent-Gyorgyi A. The physiological activity of adenine compounds with especial reference to their action upon the mammalian heart. J Physiol. 1929;68:213–37.
Watt AH, Routledge PA. Transient bradycardia and subsequent sinus tachycardia produced by intravenous adenosine in healthy adult subjects. Br J Clin Pharmacol. 1986;21:533–6.
DiMarco JP, Sellers TD, Berne RM, West GA, Belardinelli L. Adenosine: electrophysiologic effects and therapeutic use for terminating paroxysmal supraventricular tachycardia. Circulation. 1983;6:1254–63.
Spotnitz MD, Markowitz SM, Liu CF, Thomas G, Ip JE, Liez J, et al. Mechanisms and clinical significance of adenosine-induced dormant accessory pathway conduction after catheter ablation. Circ Arrhythm Electrophysiol. 2014;7:1136–43.
Kogawa R, Okumura Y, Watanabe I, Sonoda K, Sasaki N, Takahashi K, et al. Difference between dormant conduction sites revealed by adenosine triphosphate provocation and unipolar pace-capture sites along the ablation line after pulmonary vein isolation. Int Heart J. 2016;57:25–9.
Squara F, Liuba I, Chik W, Santangeli P, Maeda S, Zado ES, et al. Electrical connection between ipsilateral pulmonary veins: prevalence and implications for ablation and adenosine testing. Heart Rhythm. 2015;12:275–82.
Kim J, Desai S, Jadonath R, Beldner SJ. The importance of bidirectional block during pulmonary vein isolation. Pacing Clin Electrophysiol. 2013;36:e143–5.
Matsushita T, Chun S, Liem LB, Friday KJ, Sung RJ. Unidirectional conduction block at cavotricuspid isthmus created by radiofrequency catheter ablation in patients with typical atrial flutter. J Cardiovasc Electrophysiol. 2002;13:1098–102.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kapa, S., Killu, A., Deshmukh, A. et al. Dose-dependent pulmonary vein reconnection in response to adenosine: relevance of atrioventricular block during infusion. J Interv Card Electrophysiol 47, 117–123 (2016). https://doi.org/10.1007/s10840-016-0149-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-016-0149-y