
Abstract
This systematic review describes a set of practices that have evidence of positive effects with autistic children and youth. This is the third iteration of a review of the intervention literature (Odom et al. in J Autism Dev Disorders 40(4):425–436, 2010a; Prevent School Fail 54(4):275–282, 2010b; Wong et al. in https://autismpdc.fpg.unc.edu/sites/autismpdc.fpg.unc.edu/files/imce/documents/2014-EBP-Report.pdf; J Autism Dev Disorders 45(7):1951–1966, 2015), extending coverage to articles published between 1990 and 2017. A search initially yielded 31,779 articles, and the subsequent screening and evaluation process found 567 studies to include. Combined with the previous review, 972 articles were synthesized, from which the authors found 28 focused intervention practices that met the criteria for evidence-based practice (EBP). Former EBPs were recategorized and some manualized interventions were distinguished as meeting EBP criteria. The authors discuss implications for current practices and future research.
Similar content being viewed by others


Autism is currently one of the most visible and widely discussed human conditions. Its increased prevalence has brought it to the attention of society in the United States, with world-wide recognition (Lord et al. 2020). Much discussion surrounds the conceptualization of autism as a disability or as a set of unique skills that can be viewed as strengths (Urbanowicz et al. 2019). Although there is truth in both, there is also much verification that the life course for many individuals with autism, from infancy and into adulthood, is challenging for them and their families (Shattuck et al. 2018). In efforts to have a positive impact on this life trajectory, personnel in early intervention, schools, clinics, and other human service programs search for practices that could be most effective when working with children and youth with autism (Lai et al. 2020). The increased prevalence of autism (Maenner et al. 2020) has also intensified the demand for effective educational and therapeutic services, and intervention science is providing mounting evidence about practices that positively impact outcomes. The purpose of this study was to identify a set of focused intervention practices that have clear scientific evidence of positive effects with autisticFootnote 1 children and youth (i.e., evidence-based practices). For this paper, we define scientific evidence as reports in a peer-reviewed journal of an experimental study of acceptable methodological quality that addresses the efficacy of a focused intervention practice.
The imperative for establishing and continuing to update information about evidence-based practices (EBPs) is because the knowledge about the demographics, key ability features, and intervention science related to autism continues to advance. At the same time, there is also a purveyance of interventions that have little or no evidence of effectiveness and yet are described as “cutting edge” (Siri and Lyons 2014). For example, Paynter et al. (2020) recently noted that the Autism Research website operated by the National Autism Society in the U.K. (http://www.researchautism.net/autism-interventions/alphabetic-list-interventions) catalogued over 1000 interventions, and many of which lacked evidence. Lack of evidence does not mean that interventions are ineffective, as studies may not yet have been conducted. However, current human services policies in the U.S. requires that intervention practices have research evidence of their effectiveness (e.g., Individuals with Disabilities Education Act, Medicaid waiver provisions, insurance coverage regulations).
The contemporary focus on EBPs for children and youth with autism can be tracked back to Cochrane’s (1972) proposition that health and medical services be based on empirical, scientific evidence of its efficacy. The movement to base health practices on scientific evidence gained further traction through Sackett’s and colleagues’ (1996) advocacy of evidence-based medicine. An important contribution of the evidence-based medicine movement, which Cochrane also suggested, was that such identification and verification of evidence-based practice is just the first step. The selection and application of such scientifically based practices depends on the skills and wisdom of the health care worker in selecting appropriate practices for the individual and applying them with fidelity. This multi-step process of blending information about scientifically identified, efficacious practices with practitioners’ knowledge and skill has been adopted in the evidence-based movements in education (Davies 1999; Odom et al. 2005), psychology (American Psychological Association 2006) and other human services (American Speech and Hearing Association 2004).
A conceptualization of the multi-step process for moving from applied intervention research studies to a practitioner’s use of the science in their work with individual autistic children or youth appears in Fig. 1. Conducting individual intervention research studies and publishing them in peer review journals are the initial steps. Systematic reviews that identify EBPs, such as the review reported in this article, are a central step in the process. Translation of the information generated by the systematic review of EBPs into user-friendly information and supporting the use of that information through professional development and implementation science strategies (e.g., coaching, leadership, etc.) are subsequent necessary steps. The latter step would build practitioner’s knowledge and skill in selecting and implementing practices (Guldberg 2017). Any broken links in this process chain reduces the probability that the knowledge generated by research studies will be utilized in practice.

Research to practice process, with the current review reflecting the third step in the process
Evidence-Based Intervention Approaches
Focused intervention practices and comprehensive program models (i.e., previously identified as comprehensive treatment models and modified because of the potentially ableist language implied) are two broad classes of interventions that appear in the research literature (Smith 2013). Focused intervention practices are designed to address a single skill or goal of a student with autism (Odom et al. 2010a, b). These practices are operationally defined and address specific learner outcomes. Teachers, clinicians, or other practitioners select and use the practices (e.g., prompting, reinforcement, time delay) in interventions or instruction that addresses a learners individual learning goal. Focused intervention practices could be considered the building blocks of educational programs for children and youth with autism.
In contrast, comprehensive program models consist of a set of practices designed to achieve a broad learning or developmental impact on the core deficits of autism (Odom et al. 2010a, b). Comprehensive programs are organized around a conceptual framework, procedurally manualized, focus on a breadth of outcomes, and are implemented with a substantial number of hours per week across one or more years (Odom et al. 2014). Examples of such programs are the early intensive behavior intervention program based on the UCLA Young Autism Project (Smith et al. 2000), the LEAP preschool model (Strain and Bovey 2011), and the Early Start Denver Model (Dawson et al. 2012). Teachers or other professionals adopting comprehensive program models must commit to being trained and implementing the entire model that might replace a current program or in addition a current program. Because of the differences between the two classes of interventions, and to need to specify a clearly articulated and practical focus for the review, comprehensive program models were not included in this review.
Previous Literature Reviews of EBPs for Children and Youth with Autism
Before the mid-2000s, the identification of EBPs for children and youth with autism was accomplished through narrative reviews by an individual or set of authors or organizations (e.g., Simpson 2005), which were useful, but did not follow a stringent review process. Many traditional systematic review processes, such as the Cochrane Collaborative (https://www.cochrane.org/) or Project AIM (Sandbank et al. 2020), have only included studies that employed a randomized experimental group design (i.e., randomized control trial or RCT) and have excluded single case experimental design (SCD) studies. By excluding SCD studies, such reviews omit a vital experimental research methodology recognized as a valid scientific approach (What Works Clearinghouse 2020).
It is important to note that SCDs are often excluded in more traditional systematic reviews and meta-analyses, in part because such designs are thought to not be sufficiently scientific or rigorous. For example, on the previously noted Autism Research website (http://www.researchautism.net/autism-interventions/other-aspects-autism-interventions/process-for-evaluating-studies/our-ratings-system), the National Autism Society describes SCD studies as “Grade C” methodology (i.e., contrasted with Grade A and B studies which are group designs). Other reviews have excluded SCD studies entirely (Sandbank et al. 2020). While an individual SCD study provides limited evidence of efficacy, multiple replication studies by different research groups build the strength of evidence. Systematic reviews that minimize or exclude SCD studies ignore the largest body of scientific findings about focused intervention practices. When excluding SCD research, researchers are ignoring the admonition by Sackett et al. (1996): “… if no randomised trial has been carried out for our patient's predicament, we must follow the trail to the next best external evidence and work from there (p. 72).”
Many systematic reviews of interventions for autistic children and youth now appear in the research literature. Such reviews are useful in their focus on individual practices like functional communication training (Gregori et al. 2020), intervention for autistic children/youth of a certain age (Sandbank et al. 2020), or interventions occurring in certain locations such as schools (Martinez et al. 2016), and allow for more in depth review of contextual factors impacting the intervention or outcomes. They do not, however, provide a comprehensive critical summary of evidence across practices, ages, and outcomes. To date, only the National Professional Development Center on ASD (NPDC) and National Standards Project (NSP) have conducted comprehensive reviews of focused intervention practices for children and youth with autism and included both group and SCD studies.
The NSP published their comprehensive review in two phases. In Phase 1, their search process accessed articles from the early years of experimental intervention research for autistic children and youth from 1957 through September 2007 (National Autism Center, 2009). Peer-reviewed journal articles were included if the intervention/treatments were implemented in school, home, community, vocational, clinic settings and included children with autism who did not have significant co-occurring conditions. In Phase 2, the NSP investigators followed the same process as occurred in Phase 1 (National Autism Center, 2015) adding articles published from 2007 to 2012. Their analyses generated 14 practices for children and youth with autism that met their criteria for evidence-based.
The NPDC investigators also conducted two iterations of reviews of the intervention literature. The first review included articles published over the 10-year period from 1997 to 2007 (Odom et al. 2010a, b) and used the research design quality indicator criteria established by the CEC-Division for Research (Gersten et al. 2005; Horner et al. 2005) to evaluate articles for inclusion or exclusion from the review. In the second review, the NPDC team (Wong et al. 2014, 2015) used a more comprehensive search strategy, extended the coverage of the literature to include 22 years of studies (1990–2011), revised their methodological review criteria and process to include current criteria established by What Works Clearinghouse. Using a standard review protocol, they trained a national panel of 159 reviewers to evaluate the methodological quality of the journal articles. From the articles meeting quality criteria, the NPDC team identified 27 EBPs in the second review.
The purpose of this study, now being conducted by the National Clearinghouse for Autism Evidence and Practice (NCAEP), was to update the Wong et al. (2015) review, incorporating autism intervention literature from 2012 to the end of 2017. The questions addressed by this review were: What focused intervention practices are evidence-based? What outcomes areas did evidence-based focused intervention practices address? What are the characteristics of the research designs, participants, and intervention implementation?
Method
As noted, the previous review (Wong et al. 2015) included articles from 1990 to 2011. In the current review, the methods from the previous review were followed as closely as possible to access and incorporate acceptable articles published from 2012 to 2017. The two groups of articles were then combined for the re-analysis that resulted in the identification of evidence-based practices. The systematic review included five phases: search, screening, quality appraisal, data extraction and synthesis, following the PICO conceptual framework originated by Richardson et al. (1995) and followed by the Cochrane Collaboration. The methods are described in the subsequent sections and more detail about each step of the process can be found in the freely available report on the NCAEP website (https://ncaep.fpg.unc.edu/).
Search Process
The NCAEP research team and a research librarian from the University of North Carolina at Chapel Hill developed and refined the literature search plan. The databases utilized in the search were: Academic Search Premier, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Excerpta Medica Database (EMBASE), Educational Resource Information Center (ERIC), PsycINFO, Social Work Abstracts, PubMed, Thomson Reuters (ISI) Web of Science, and Sociological Abstracts. Search terms were intentionally broad to be as inclusive as possible and included terms related to diagnosis (autism OR autistic OR Asperger OR ASD OR ASC [autism spectrum condition] OR pervasive developmental disorder OR PDD/PDD-NOS) and practice (intervention OR treatment OR practice OR strategy OR therapy OR program OR procedure OR approach OR methods OR education OR curriculum). The only filters used were peer-reviewed, language (English) and publication date (2012–2017). Deduplication was used to eliminate duplicate articles from the initial search prior to screening.
Screening Process
Prior to the title/abstract and full-text phases of the screening process, NCAEP team members participated in trainings to review the inclusion and exclusion criteria (see subsequent sections) and screening procedures. For the title/abstract screening, the NCAEP team reviewed the title and abstract of the article and indicated if the article should be excluded or further reviewed in a full-text screening. Following the title/abstract screening, the team gathered the full-text version of all articles that were not excluded. During the full-text screening, team members indicated if an article should be included or excluded, and for excluded articles indicated a reason for exclusion. Both steps were completed internally by single reviewers.
Inclusion/Exclusion Criteria for Studies in the Review
Articles included in this review were published in peer-reviewed, English language journals between 1990 and 2017. The study inclusion criteria are described in the subsequent sections and summarized in Table 1.
Population/Participants
A study had to have participants whose ages were between birth and 22 years of age and were identified as having autism spectrum disorder (ASD), autism, Asperger syndrome, pervasive developmental disorder, pervasive developmental disorder-not otherwise specified, or high-functioning autism. Studies varied on the description of the autism diagnosis- some had ADOS or ADIR data, others reported clinical diagnoses by psychiatrists or physicians, while others used diagnoses provided by public school evaluations. Participants with autism who also had co-occurring conditions (e.g., intellectual disability, genetic syndrome, mental health conditions) were included in this review. Studies with participants identified as “at risk for autism” were not included in the review.
Interventions
The focused intervention practices examined in a study had to be behavioral, developmental, and/or educational in nature. Studies in which the independent variables were only medications or nutritional supplements/special diets (e.g., melatonin, gluten-casein free, vitamins) were excluded from the review. In addition, only interventions that could be practically implemented in typical educational, clinical, home, or community settings were included. As such, intervention practices requiring highly specialized materials, equipment, or locations unlikely to be available in most educational, clinic, community, or home settings were excluded (e.g., dolphin therapy, hippotherapy, hyperbaric chambers). Interventions requiring the supervision of trained medical personnel were excluded (e.g., chelation, neurofeedback, or acupuncture/acupressure).
Outcomes
Studies had to generate behavioral, developmental, academic, vocational, or mental health outcomes (i.e., dependent variables). Outcome data could be discrete behaviors (e.g., social initiations, stereotypies) assessed observationally, ratings of behavior or student performance (e.g., parent/teacher questionnaires), standardized assessments (e.g., nonverbal IQ tests, developmental assessments), and/or informal assessment of student academic performances (e.g., percentage of correct answers for instructional task). Studies only reporting physical health outcomes were excluded. Studies that targeted only caregiver and/or staff outcomes or only examined how those outcomes mediated student outcomes were excluded.
Study Designs
Studies included in the review had to employ a group design or SCD to test the efficacy of focused intervention practices. Adequate group designs included randomized control trials, sequential multiple assignment randomized trials, quasi- experimental designs, or regression discontinuity designs that compared an experimental/intervention group receiving the intervention to a control or comparison group that did not receive the intervention or received another intervention (Shadish et al. 2002). SCDs had to demonstrate the functional relationships between the intervention (or independent variable) and the autistic child/youth outcomes (Kazdin 2011). Acceptable SCDs for this review were withdrawal of treatment (ABAB), concurrent multiple baseline, multiple probe, alternating treatment, and changing criterion designs (Horner and Odom 2014), as well as SCDs that included hybrid designs (e.g., an ABAB set of phases in an multiple baseline design). Studies that were solely descriptive, examined only predictors, reviewed existing literature, or were meta-analyses were excluded. In addition, non-concurrent multiple baseline studies and component analyses without a baseline condition were also excluded.
Quality Appraisals
Protocols for reviewing group design and SCD studies used to determine methodological acceptability were developed in the Wong et al. (2015) review and appear in the supplemental materials for this article. The protocols drew from the methodological quality indicators developed by Gersten and colleagues (2005) for group design and Horner et al. (2005) for SCD, as well as the review guidelines established by the WWC. In addition, the last item on each protocol asked reviewers to make a judgement about whether the study reported positive effects for the intervention. Protocols went through two iterations of pilot testing within the research group and then were reviewed by two national leaders in research methodology and intervention research, with expertise in SCD and group design, respectively for finalization. Only minor updates were made in the current review (e.g., include SMART design as a design option).
National Board of Reviewers
To assist in quality appraisals, external reviewers were recruited through professional organizations (e.g., Association for Behavior Analysis International, Council for Exceptional Children), professional contacts, social media, the NCAEP website, and solicitation to reviewers from the previous review. The criteria for qualifying for the subsequent training was that the individual had to have a graduate degree or be a current Ph.D. student, had to have finished coursework in experimental group design and/or single case design research, and had to have had coursework related to and/or experience working with individuals with autism. The reviewers self-identified their methodological expertise and interests as group, SCD, or both. Reviewers completed an online training process described fully in the project report (http://go.unc.edu/Hk72T). Following training, they coded a “master-file” article (i.e., an article in which correct review answers had been established by our team) that employed the respective design. For the review of the master-file study, reviewers had to meet an 80% inter-rater agreement criterion for study elements. If potential reviewers did not meet the criteria, they were allowed to review the training materials and complete the task a second time (i.e., with a different master-file article for the article review).
Two hundred and twenty-one reviewers completed the training and met inter-rater agreement criteria with the master code files; 55% completed requirements for single case design articles (n = 122), 10% completed requirements for group design articles (n = 21), and 35% completed requirements for both design types (n = 78). Most reviewers received their degrees in the area of special education or applied behavior analysis and were faculty, graduate students, or practitioners. Reviewers were acknowledged in the report and BCBA/BCaBA reviewers received continuing education credit if requested.
Ten articles were randomly assigned to each reviewer, with the exception that a check was conducted after assignment to make sure that reviewers had not been assigned an article for which they were an author. They first completed a set of screening questions about the articles (e.g., type of study design) followed by the methodological review items for SCD or group design. If an article met all individual methodological items on the protocol, reviewers noted whether the study had positive effects for autistic participants on at least one outcome variable and listed the variables with positive effects. Last, reviewers described the key features of the study (e.g., participant characteristics) and the intervention procedures. Each article was independently reviewed by two external reviewers. Once both reviews for a given article were complete, the NCAEP team identified any disagreements between the reviewers related to methodological quality and effects. If needed, an NCAEP team member was assigned to complete a third review and make a final determination about quality and/or effects. A third review was required for 42% of the articles, including 27% that were reviewed for quality and effects and 15% that were reviewed for effects only.
Inter-rater Agreement
The NCAEP team collected inter-rater agreement on quality appraisals for 1,085 articles. The formula for inter-rater agreement was rating agreements divided by agreements plus disagreements multiplied by 100%. Agreement was calculated for (a) methodological quality review items on the review protocol, (b) summative evaluation of whether a study met or did not meet quality criteria, and (c) evaluation of whether or not studies that met quality criteria had positive effects for autistic participants on at least one outcome variable. Mean inter-rater agreement on the individual items for quality review was 85% (range = 55–97%) for group design articles and 93% (range = 87–97%) for SCD articles, generating a total mean item agreement of 90%. Mean inter-rater agreement for summary decisions about article inclusion was 65% for group design articles and 80% for SCD articles, generating a total agreement of 73%. This agreement percentage was lower because if a single reviewer rated even a single item as negative, it led to exclusion of the article from the study. As noted, when a disagreement between reviewers occurred, a third internal review was conducted by an NCAEP staff member, which led to a consensus decision about inclusion or exclusion of the article. Of the included articles, there was 86% agreement for group design articles and 74% agreement for SCD articles on the presence of positive effects, yielding a total agreement of 80% (i.e., between the respective reviewers who agreed on the previous inclusion decision). When disagreement occurred on the positive effects report, internal NCAEP staff conducted another review just focusing on the decision about positive effects to yield a consensus judgment.
Data Extraction
The NCAEP Team followed a three-step data extraction process. First, team members compared external reviewers reports of participant characteristics (e.g., diagnosis, age) and outcomes (i.e., dependent variables), and made final determinations for this information. Second, team members thoroughly reviewed each article to identify primary interventions. In this identification step, the reviewer could: assign an article to one or more of the 27 practice categories identified in the previous review (Wong et al. 2014); assign the article to a practice category that had been identified as having some evidence in the previous review; and/or identify a new possible category of practices represented in the article. Third, different team members reviewed each article assigned to a given practice in the previous step to confirm that it fit within the practice description. During this step of data extraction, team members also identified manualized interventions that fit within a practice. Manualized interventions shared procedural features that were similar to other interventions in the category but had unique features that distinguished them as a salient model and had an identifiable title. For example, Social Stories™ is a trademarked intervention by Carol Gray and Garand (1993), that fits within Social Narratives practice description, but is also distinct as a particular type of Social Narrative. Also, during the data extraction phase of the review, our team identified additional articles that were removed for not meeting eligibility requirements and/or quality standards, which may have been missed in the original quality review. These decisions were confirmed by a second team member. Then, the data were compiled for analysis and synthesis.
Synthesis and Identification of EBPs
When all included articles were assembled into categories, the team made a final determination about whether a practice met the level of evidence necessary to be classified as an EBP using criteria for evidence established by the previous NPDC team. The NPDC’s criteria were drawn from the work of Nathan and Gorman (2007), Rogers and Vismara (2008), Horner and colleagues (2005), and Gersten and colleagues (2005), as well as the earlier work by the APA Division 12 (Chambless and Hollon 1998). Its rationale is based on the necessity of having a sufficient number of empirical demonstrations of efficacy through high quality, peer-reviewed journal articles and replications of those demonstrations by independent research groups.
Different criteria were established for group and single case design evidence. To be identified as evidence-based, a category of practice had to contain (a) two high quality group design studies conducted by two different research groups, (b) five high quality single case design studies conducted by three different research groups and involving a total of 20 participants across studies, or (c) a combination of one high quality group design study and three high quality single case design studies with the combination being conducted by two independent research groups. Independence of research groups was defined as the research being located in different settings and the key constituent members of the authorship of published articles being different from other research groups.
Results
Search Results
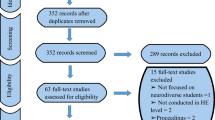
The search update incorporated results from the nine databases which generated an initial total of 61,147 articles and 31,779 after duplicates were removed. Following the title/abstract and full-text screening, quality appraisal, and a final review during data extraction, 567 articles met the established criteria for evidence and showed positive effects for at least one relevant outcome. Figure 2 is the PRISMA chart that shows the articles excluded and included at each of the steps for both the previous (1990–2011) and current (2012–2017) review periods.

PRISMA flow charts
The NCAEP team reviewed the remaining 567 articles with positive effects and determined that 545 of the articles were primary studies (i.e., not secondary data analysis or follow-up analysis of a primary study in the review). These 545 studies were combined with 427 studies from the previous review, yielding a total of 972 acceptable articles. The number of articles by year of publication appears in Fig. 3, demonstrating a clear acceleration in acceptable articles from 1990 to 2017.

Increase in accepted articles across time
Participant Characteristics
Paricipants were described by diagnosis, age, sex, and race/ethnicity/nationality.
Diagnosis and Co-morbid Conditions
Autism was the most frequently reported diagnosis in studies, with 64% of studies indicating at least one participant with autism (a given study could include multiple diagnostic or co-occurring conditions categories). There was, however, a drop in the use of “autism” as a descriptor from the 1990–2011 period (83%) to the 2012–2017 period (48%). There was a large increase in reporting of “ASD” as a diagnosis, moving from 12% (1990–2011) to 55% (2012–2017). The reports of participants with “Asperger” or “High Functioning Autism” (HFA) and “PDD” or “PDD-NOS” were relatively low (10% and 14%) and stayed fairly stable across review periods. Although 55% of the studies failed to report any information on co-occurring conditions, when reported, the most frequent co-occurring condition was intellectual disability (21%).
Age
Participants’ ages were classified into six categories and multiple age categories could be selected for each study. The majority of studies were conducted with preschool (43%) and elementary-aged children (57%). When comparing the 1990–2011 and 2012–2017 review periods, there were substantial increases in the percentages of studies conducted with 12–14-year-olds (17% and 27% respectively) and 15–18-year-olds (10% and 17% respectively). The youngest age category, birth-35 months, had a slight increase (6% to 9%) and the oldest age category, 19–22 years, remained stable across review periods at 5%.
Gender/Sex
In the previous review, data on gender and sex were not extracted so these data only reflect the 2012–2017 review period. Data on the gender or sex of the participants were reported in 93% of studies. Although “non-binary” and “other” were included as options during the data extraction, no studies reported these categories. In studies that reported the number of participants in the gender or sex categories, 84% of participants were male.
Race/Ethnicity/Nationality
Data on race/ethnicity/nationality were also not extracted in the 1990–2011 studies, so these data reflect the 2012–2017 review period. Thirty percent of the studies reported data on race/ethnicity/nationality. For studies that reported numbers of participants by categories, 59% of the participants were White, 10% were Black, 9% were Asian, and 8% were Hispanic/Latino. All other groups had less than 5% representation among participants in studies reporting this information.
Study Design Types
Across the studies for both review periods, single case design studies made up 83% of the articles and group design made up 17%. The primary group design employed was a randomized control design (14% of total), followed by quasi-experimental design (3%), and one sequential multiple assignment randomized trials design. For single case designs, the multiple baseline (31%) and multiple probe designs were the most frequently used (14%) followed by withdrawal of treatment (12%). One notable change is that 23% were group designs for the 2012–2017 set of studies, compared to only 9% of the studies in the previous review period.
Implementation Characteristics
Data on implementation characteristics were only extracted from the 2012–2017 review period. Research staff implemented (i.e., directly provided) interventions in 52% of the studies and were coaches in 10% of studies. Educators and related service providers were each identified as implementers in 20% of studies, and parents were noted as implementers in 10% of studies. In 48% of studies the intervention took place in educational settings. The other intervention locations were university clinic/research lab settings (20% of studies), home settings (18%), and community clinic settings (13%). On occasion, studies took place in more than one setting so multiple locations could be selected for a single study. Seventy-nine percent of the studies were conducted in individual sessions (i.e., one-on- one), and 14% were conducted in small group settings with 3–6 total participants. All other group sizes occurred in less than 6% of the studies.
Evidence-Based Practices
Twenty-eight practices met the criteria for being evidence-based. The 28 EBPs, their abbreviated definitions, the number of articles from each review period, and the number of articles from each study type (i.e., SCD, group) that contributed to the evidence base are included in Table 2. The specific studies supporting the practice are listed in the original report (Steinbrenner et al. 2020). There are five new EBP categories in this review: Behavior Momentum Intervention, Direct Instruction, Music-Mediated Intervention, Sensory Integration (i.e., explicitly the model developed by Ayres 2005), and Augmentative and Alternative Communication (AAC; includes practices previously in other categories).
The inclusion of the new literature from 2012 to 2017 led to some recategorization and reconceptualization of EBPs from the previous review. PECS® was merged with AAC, Pivotal Response Training (PRT) was merged into Naturalistic Interventions, Scripting was merged into Visual Supports. Also, Peer-Mediated Intervention and Instruction and Structured Play Groups were merged into the new category of Peer-based Intervention and Instruction. Exercise was broadened to Exercise and Movement, and Cognitive Behavioral Intervention was broadened to Cognitive Behavioral/Instructional Strategies.
Manualized Interventions Meeting Criteria for EBPs
Emerging from the current review were interventions that clearly fit the EBP categorical definitions but had themselves enough evidence to be classified as an EBP. The NCAEP team identified these practices as Manualized Interventions Meeting Criteria (MIMCs) and grouped them within established EBP categories. The rationale for this classification was to provide conceptual clarity of the EBP organization but also to highlight the particular approach. In addition to having sufficient evidence, MIMCs had to have clearly established manualized procedures or software. In total, there were 10 MIMCs classified within six of the EBP categories. These MIMCs appear in Table 3. More detail about the reclassification process may be found in the full report (Steinbrenner et al. 2020).
Outcomes
The child/youth outcomes addressed by studies in this review appear in Table 4, along with the number of studies supporting each reported in the earlier and current review. Communication, social, and challenging/interfering behavior were outcomes addressed most often. Outcomes with increased number of studies from the previous to current review were academic, mental health, and vocational. Self-determination was added as an outcome. Outcomes for which there were fewer articles in the most recent review update (2012–2017) as compared to the previous review were challenging behavior, joint attention, play, and school readiness.
A matrix that displays the outcomes identified for each EBP, also sorted by age group within the EBP can be found in Fig. 4. The filled cells indicate that at least one study generated the indicated outcome for an age group (from the column) for a specific intervention (from the row). Most of the EBPs have at least some evidence of impact across a wide variety of ages (three or more age groups). In general, EBPs tend to address a wide variety of outcome categories, ranging from four to 11 outcomes. Notably, 23 EBPs have been shown to impact seven or more outcome categories and 16 EBPs have been shown to impact nine or more.

Matrix of evidence-based practices, outcomes, and age categories
Discussion
The current report updates and extends the work on evidence-based, focused intervention practices begun with an initial review of the literature from 1997 to 2007 (Odom et al. 2010a, b) and extended through a second report that covered the literature from 1990 to 2011 (Wong et al. 2015); extending this systematic review through 2017 added 567 articles to the review. As the intervention literature has provided more empirical information and as practices have evolved, some of the classifications required reconceptualization and revision of previous definitions. In an active research area, knowledge does not stand still, and in fact identification of EBPs should be dynamic, reflecting the growth of knowledge across time (Biglan and Ogden 2019).
The five new practices in this review are Augmentative and Alternative Communication (AAC), Behavior Momentum Intervention, Direct Instruction, Music-Mediated Intervention, and Sensory Integration. It is important to note that Sensory Integration refers explicitly to the classical sensory integration model developed by Jean Ayres (2005) and not to a variety of interventions that address sensory issues but have been found to be unsupported (Case-Smith et al. 2015; Watling and Hauer 2015). Also, several EBP categories from previous reviews were reclassified into other EBP categories (i.e., Scripting into Visual Supports, Peer-Mediated Intervention and Instruction and Structured Play Groups into Peer-Based Intervention and Instruction).
The growth of the published empirical literature led to a new classification of interventions noted above as MIMC. These interventions were developed by individual research groups and had sufficient evidence to meet the criteria as an EBP. However, the procedural features overlapped directly with established EBP categories. As such, MIMC could be considered “EBPs within broader EBP categories.” Ten interventions met the criteria for MIMC and have sufficient evidence to meet the EBP criteria. In addition, these interventions have clearly established manualized procedures or software, often including training protocols, which may better facilitate their uptake and implementation (Kasari and Smith 2013). Two interventions, PECS® (Frost and Bondy 2002) and PRT (Koegel and Koegel 2006; Stahmer et al. 2011), previously identified as EBP categories were reclassified under AAC and Naturalistic Intervention, respectively. The MIMC classification does not convey in any way that the interventions are less strong or efficacious than previously indicated, because they both have an extensive set of research that supports their efficacy. Also, some MIMCs have features that cross EBP categories. For example, Project ImPACT (Ingersoll and Dvortcsak 2019) was classified within the Parent-Implemented EBP but it also shares some characteristics with Naturalistic Intervention.
Because this review included articles for two time periods, it was possible to examine trends across time. In our analysis, SCD remained the primary methodology employed, constituting 85% of the acceptable studies. Multiple baseline and multiple probe designs were more frequently used in the more current set of articles as compared to the earlier review, perhaps because they do not require a treatment to be withdrawn in order to demonstrate an experimental effect of the intervention (i.e., as is necessary in ABAB designs). Although group designs were only 17% of the studies included overall, there was a dramatic increase in the number of RCT studies included between the review periods, which may reflect greater access to the number of participants with autism needed to establish power for RCT analyses and/or priorities of funding agencies.
Information on the intervention setting, implementer, and group size was available from the 2012–2017 review period. Commenting on the earlier research literature, Parsons and Kasari (2013) lamented the fact that most intervention research was not occurring in the educational settings where many children and youth with autism spend a great part of their life. In the current review, nearly 50% of the research was conducted in education settings, the largest of any setting reported. While an important step in the right direction, the majority of the research was still being conducted in individual sessions by research staff members. Certainly, directions for the future would be to examine more often the efficacy of interventions when implemented in “authentic” educational settings by practitioners such as teachers, speech language pathologists, psychologists, and other service providers.
Outcomes for intervention participants shifted somewhat from the 1990–2011 to the 2012–2017 review period. As noted, communication, social, and behavior outcomes occurred most frequently across both review periods, as would be expected given that these are the challenges that define autism. There were notable increases in studies that targeted academic skills, vocational skills, and mental health, although the number of studies addressing these outcomes remains low relative to the number of studies. These outcomes are important, especially for adolescents and young adults with autism, and their low frequency document needed areas for research in the future.
For this review, outcomes were coded by domain and individual dependent variables were not coded. For focused intervention practices, researchers tend to address individual skills or behaviors. Also, for SCD studies, researchers employ dependent measures that can be used repeatedly across time to monitor changes in student performance (Kazdin 2011). A safe assumption is that for SCD studies, the outcome assessments employed observational or rating scale data. For group design studies, these methodologies may also be used, but researchers also would have more frequently employed standardized, norm-referenced measures. Describing specific assessment methodology of EBP studies would certainly be a feature of future research.
A number of demographic findings have implications for future research as well. As in the earlier review, the majority of the 2012–2017 studies were conducted with preschool and elementary-aged children with autism, indicating an important need for increased research with infants/toddlers, adolescents, and young adults with autism. Also, although it fits the overall demographic of autism, most studies were conducted with male participants, and information about differential effects for female participants with autism continues to be under-examined. Finally, there are gaps related to the reporting, inclusion, and analysis of participants with co-occurring conditions, which should be addressed in future studies.
In the 2012–2017 review period, information was collected about whether researchers reported the race/ethnicity/nationality of autistic participants, which did not happen in the previous review. However, West and colleagues (2016) recoded the earlier set of articles to retrieve those data, which can serve as a point of comparison. West et al. found that only 17.9% of the articles from 1990 to 2011 reported race/ethnicity, while in the 2012–2017 review period, 30% of the reviewed articles reported these data. In both sets of studies, Black and Hispanic/Latino were the most frequent nonwhite racial/ethnic categories reported. The number of participants from nonwhite racial and ethnic groups in the subset of studies that reported these data was strikingly low compared to what would be expected based on community demographics. For example, only 8% of research participants were Hispanic/Latino, while in the United States alone, 26% of the school age population identifies as Hispanic (U.S. Department of Education 2017). Also, differential treatment outcomes related to race/ethnicity/nationality were not examined, which is similar to findings by Pierce et al. (2014) in an analysis of studies published between 2000 and 2010. Last, socioeconomic class (SES) of participants is rarely described for autistic participants in research studies, so the possibility of determining how SES affects treatment outcomes is largely not possible.
Limitations
Several limitations exist for this review. As noted, the review included only studies published from 1990 to 2017. Two limitations exist regarding this timeframe. First, studies that occurred before 1990 were not included, although one might expect early (i.e., pre-1990) studies of important and effective practices to have been replicated in publications over subsequent years. Second, because of the time required to conduct a review of a very large database and involve a national self-selected set of reviewers, there was a lag between the end date for a literature review (i.e., 2017) and the date which the review is published. Certainly, studies have been published in the interim that could have impacted the EBP classifications.
Regarding the methodology of the review, this was clearly a systematic review of the literature and not a meta-analysis. So, the magnitude of effect size was not examined. Also, the review only contained peer-reviewed journal articles and not grey literature, as sometimes occurs in meta-analyses (McAuley et al. 2000). In addition, studies with null findings were not included. In fact, experimental studies are rarely set up to prospectively test for null findings, although there are methodological procedures for addressing such a question (Greene et al. 2007). Research studies with a hypothesis of treatment condition differences that instead “prove the null hypothesis” run the greater risk of Type II error. Last, although methodological quality indicators were drawn from recognized authoritative sources in the field, it is possible that a more detailed analysis of methodology than was practical for this review could have influenced the studies included in this review.
Implications and Conclusions
The current review, as noted previously, is an important link in the research to practice process. When translated into useable and accessible information for practitioners (Sam et al. 2020a, b) and supported through professional development and implementation science (Sam et al. 2020a, b), these practices can be essential components of effective programs for autistic children and youth. That is, practitioners may match EBPs to specific learning goals for autistic children and youth (Cox and Sam n.d.) analogous to the way medical practitioners match specific treatments to the health needs and characteristics of their patients in personalized medicine. By assembling multiple EBPs to address specific learning needs, practitioners can build a technical eclectic program for children and youth with autism (Lazarus and Beutler 1993). In such an approach, practitioners establish programs with strong program quality as a foundation, develop individualized and clearly articulated goals for children/youth, select and implement practices that may have different theoretical bases but also have demonstrated efficacy (Odom et al. 2012). In a recent study, Sam et al. (2020a, b) employed such a program in 59 elementary schools and found significantly positive effects for program quality, teachers use of EBP with fidelity, and autistic children goal attainment.
In conclusion, the current study provided an updated review of the empirical evidence supporting focused intervention practices. In this review, nearly 1,000 studies were identified, with over half being published between 2012 and 2017. The updated review led to a revised set of 28 primary EBPs and also 10 interventions that classified as MIMCs. Examination of trends from the earlier review and current update suggest that SCD studies continue to be the modal form of research although RCT are being used more often. This analysis suggests that important directions for future research include intervention effects related to race, ethnicity, and gender as well as increased research for both infants/toddlers and adolescents/young adults with autism.
Change history
20 January 2022
A Correction to this paper has been published: https://doi.org/10.1007/s10803-022-05438-w
Notes
In this document, we will use a mixture of terminology when referring to autism and persons identified as autistic. A common form of description has been called “person-first”, in which the person (e.g., child) appears before the condition (e.g., autism), such as child with autism. Many autistic self-advocates and advocacy groups now prefer an identify-first form, such as autistic child (Brown 2011; Kenny et al. 2016). In addition, autistic advocates have spoken about the desirability of using the term “autism” rather than autism spectrum disorder (Brown, 2011). At the time of this writing, terminological issues have not been settled. To honor the advocates and professionals in the field, as well as other groups of individuals with disabilities who prefer the person-first term, we will be mixing terminology throughout the manuscript, using both person-first and identity-first terminology with the primary descriptor being autism or autistic.
References
American Psychological Association. (2006). APA Presidential Task Force on Evidence-Based Practice. Evidence-based practice in psychology. American Psychologist., 61(4), 271–285. https://doi.org/10.1037/0003-066X.61.4.271.
American Speech-Language-Hearing Association. (2004). Evidence-based practice in communication disorders: an introduction [Technical Report]. www.asha.org/policy.
Ayres, A. J. (2005). Sensory integration and the child: Understanding hidden sensory challenges. Los Angeles: Western Psychological Services.
Biglan, A., & Ogden, T. (2019). The evolution of evidence-based practices. European Journal of Behavior Analysis, 9(1), 81–95. https://doi.org/10.1080/15021149.2008.11434297.
Brown, L. (2011). Identity and hypocrisy: a second argument against person-first language, November 28. Available at http://www.autistichoya.com/2011/11/identity-and-hypoc-risy-second-argument.html (accessed March 15, 2020).
Case-Smith, J., Weaver, L. L., & Fristad, M. A. (2015). A systematic review of sensory processing interventions for children with autism spectrum disorders. Autism, 19(2), 133–148.
Chambless, D. L., & Hollon, S. D. (1998). Defining empirically supported therapies. Journal of Consulting and Clinical Psychology, 66(1), 7–18. https://doi.org/10.1037/0022-006X.66.1.7.
Cochrane, A. L. (1972). Effectiveness and efficiency: Random reflections of health services. London: Nuffield Provincial Hospitals Trust.
Cox, A., & Sam, A. (n. d.). Selecting an evidence-based practices. Autism Focused Intervention Resources and Materials. https://afirm.fpg.unc.edu/selecting-ebp
Davies, P. (1999). What is evidence-based education? British Journal of Education, 47(2), 108–121. https://doi.org/10.1111/1467-8527.00106.
Dawson, G., Rogers, S., Munson, J., Smith, M., Winter, J., Greenson, J., et al. (2012). Randomized, controlled trial of an intervention for toddlers with autism: The Early Start Denver Model. Pediatrics, 125(1), e17–e23. https://doi.org/10.1542/peds.2009-0958.
Frost, L., & Bondy, A. (2002). The picture exchange communication system training manual (2nd ed.). Pyramid Educational Products: Newark.
Gersten, R., Fuchs, L. S., Compton, D., Coyne, M., Greenwood, C. R., & Innocenti, M. S. (2005). Quality indicators for group experimental and quasi-experimental research in special education. Exceptional Children, 71(2), 149–164. https://doi.org/10.1177/001440290507100202.
Golan, O., & Baron-Cohen, S. (2006). Systemizing empathy: Teaching adults with Asperger syndrome or high-functioning autism to recognize complex emotions using interactive multimedia. Development and Psychopathology, 18(2), 591–617. https://doi.org/10.1017/S0954579406060305.
Gray, C. (2000). The new social story book. Future Horizons: Arlington.
Gray, C. A., & Garand, J. D. (1993). Social stories: Improving responses of students with autism with accurate social information. Focus on Autistic Behavior, 8(1), 1–10. https://doi.org/10.1177/108835769300800101.
Greene, C. J., Morland, L. A., Durkalski, V. L., & Frueh, B. C. (2007). Noninferiority and equivalence designs: Issues and implications for mental health research. Journal of Traumatic Stress, 21(5), 433–439. https://doi.org/10.1002/jts.20367.
Gregori, E., Wendt, O., Gerow, S., Peltier, C., Genc-Toursun, D., Lory, C., & Gold, Z. S. (2020). Functional communication training for adults with autism spectrum disorder: A systematic review and quality appraisal. Journal of Behavioral Education, 29(1), 42–63. https://doi.org/10.1007/s10864-019-09339-4.
Guldberg, K. (2017). Evidence-based practice in autism educational research: Can we bridge the research and practice gap? Oxford Review of Education, 43(2), 149–161. https://doi.org/10.1080/03054985.2016.1248818.
Hopkins, I. M., Gower, M. W., Perez, T. A., Smith, D. S., Amthor, F. R., Wimsatt, F. C., & Biasini, F. J. (2011). Avatar assistant: Improving social skills in students with an ASD through a computer-based intervention. Journal of Autism and Developmental Disorders, 41(11), 1543–1555. https://doi.org/10.1007/s10803-011-1179-z.
Horner, R. H., Carr, E. G., Halle, J., McGee, G., Odom, S., & Wolery, M. (2005). The use of single subject research to identify evidence-based practice in special education. Exceptional Children, 71(2), 165–180. https://doi.org/10.1177/001440290507100203.
Horner, R. H., & Odom, S. L. (2014). Constructing single-case research designs: Logic and options. In T. R. Kratochwill & J. R. Levin (Eds.), Single-case intervention research: Methodological and data-analysis advances (pp. 27–52). Washington: American Psychological Association.
Ingersoll, B., & Dvortcsak, A. (2019). The Project ImPACT manual for parents. New York: Guilford.
Kaiser, A. P., & Roberts, M. Y. (2013). Parent-implemented enhanced milieu teaching with preschool children who have intellectual disabilities. Journal of Speech, Language, and Hearing Research, 56(1), 295–309. https://doi.org/10.1044/1092-4388(2012/11-0231.
Kasari, C., Kaiser, A., Goods, K., Nietfeld, J., Mathy, P., Landa, R., et al. (2014). Communication interventions for minimally verbal children with autism: A sequential multiple assignment randomized trial. Journal of the American Academy of Child and Adolescent Psychiatry, 53(6), 635–646. https://doi.org/10.1016/j.jaac.2014.01.019.
Kasari, C., & Smith, T. (2013). Interventions in schools for children with autism spectrum disorder: Methods and recommendations. Autism, 17(3), 254–267. https://doi.org/10.1177/1362361312470496.
Kazdin, A. E. (2011). Single-case research designs: Methods for clinical and applied settings (2nd ed.). Oxford University Press: Oxford.
Kenny, L., Hattersley, C., Molins, B., Buckley, C., Povey, C., & Pellicano, E. (2016). Which terms should be used to describe autism? Perspectives from the UK autism community. Autism, 20(4), 442–462. https://doi.org/10.1177/1362361315588200.
Koegel, R. L., & Koegel, L. K. (2006). Pivotal response treatments for autism: Communication, social, and academic development. Brookes: Paul H.
Lai, M., Anagnostou, E., Wiznitzer, M., Allison, C., & Baron-Cohen, S. (2020). Evidence-based support for autistic people across the lifespan: Maximising potential, minimising barriers, and optimising the person–environment fit. Lancet Neurology, 19, 434–451. https://doi.org/10.1016/S1474-4422(20)30034-X.
Laugeson, E. A., & Frankel, F. (2010). Social skills for teenagers with developmental and autism spectrum disorders: The PEERS treatment manual. Routledge.
Lazarus, A. A., & Beutler, L. E. (1993). On technical eclecticism. Journal of Counseling & Development, 71(4), 381–385. https://doi.org/10.1002/j.1556-6676.1993.tb02652.x.
Lord, C., Traolach, T. S., Charman, T., Cusack, J., Dumas, G., Frazier, T., et al. (2020). Autism spectrum disorder. Nature Reviews, 6(5), 1–23. https://doi.org/10.1038/s41572-019-0138-4.
Maenner, M. J., Shaw, K. A., Baio, J., Washington, A., Patrick, M., DiRienzo, M., Christensen, D. L., Wiggins, L. D., Pettygrove, S., Andrews, J. G., Lopez, M., Hudson, A., Baroud, T., Schwenk, Y., White, T., Rosenberg, C.R., Lee, L.-C., Harrington, R. A., Huston, M., … Dietz, P. M. (2020). Prevalence of autism spectrum disorder among children aged 8 years—Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2016. MMWR Surveillance Summary, 69(4), 1–12. https://doi.org/10.15585/mmwr.ss6904a1
Martinez, C. K., Betz, A. M., Liddon, C. J., & Werle, R. L. (2016). A progression to transfer RIRD to the natural environment. Behavioral Interventions, 31(2), 144–162. https://doi.org/10.1002/bin.1444.
McAuley, L., Pham, B., Tugwell, P., & Moher, D. (2000). Does the inclusion of grey literature influence estimates of intervention effectiveness reported in meta-analyses?. Lancet, 135, 1228–1231. https://doi.org/10.1016/S0140-6736(00)02786-0.
Nathan, P. E., & Gorman, J. M. (Eds.). (2007). A guide to treatments that work (3rd ed.). OxfordUniversity Press. https://doi.org/10.1093/med:psych/9780195304145.001.0001
National Autism Center. (2009). National standards report. Randolph, MA: Author https://www.nationalautismcenter.org/reports/
National Autism Center. (2015). Findings and conclusions: National standards project, phase 2. Randolph, MA: Author. https://www.nationalautismcenter.org/national-standards-project/results-reports/
Odom, S. L., Boyd, B. A., Hall, L. J., & Hume, K. (2010a). Evaluation of comprehensive treatment models for individuals with autism spectrum disorders. Journal of Autism and Developmental Disorders, 40(4), 425–436. https://doi.org/10.1007/s10803-009-0825-1.
Odom, S. L., Brantlinger, E., Gersten, R., Horner, R., Thompson, B., & Harris, K. (2005). Research in special education: Scientific methods and evidence-based practices. Exceptional Children, 71, 137–148. https://doi.org/10.1177/001440290507100201.
Odom, S. L., Boyd, B., Hall, L., & Hume, K. A. (2014). Comprehensive treatment models for children and youth with autism spectrum disorders. In F. Volkmar, R. Paul, S. Rogers, & K. Pelphrey (Eds.), Handbook of autism and pervasive developmental disorders (4th ed., Vol. 2, pp. 770–778). Wiley. https://doi.org/10.1002/9781118911389.hautc42
Odom, S. L., Collet-Klingenberg, L., Rogers, S. J., & Hatton, D. D. (2010b). Evidence-based practices for children and youth with autism spectrum disorders. Preventing School Failure: Alternative Education for Children and Youth, 54(4), 275–282. https://doi.org/10.1080/10459881003785506.
Odom, S., Hume, K., Boyd, B., & Stabel, A. (2012). Moving beyond the intensive behavior treatment versus eclectic dichotomy: Evidence-based and individualized programs for learners with ASD. Behavior Modification, 36(3), 270–297. https://doi.org/10.1177/0145445512444595.
Parsons, S., & Karsari, C. (2013). Schools at the centre of educational research in autism: Possibilities, practices and promises. Autism, 17(3), 251–253. https://doi.org/10.1177/1362361313483624.
Paynter, J., Luskin-Saxby, S., Keen, D., Fordyce, K., Frost, G., Immus, C., et al. (2020). Brief report: Perceived evidence and use of autism intervention strategies in early intervention providers. Journal of Autism and Developmental Disorders, 50(10), 1088–1094. https://doi.org/10.1007/s10803-019-04332-2.
Pierce, N. P., O’Reilly, M. F., Sorrells, A. M., Fragale, C. L., White, P. J., Aguilar, J. M., & Cole, H. A. (2014). Ethnicity reporting practices for empirical research in three autism-related journals. Journal of Autism and Developmental Disorders, 44(7), 1507–1519. https://doi.org/10.1007/s10803-014-2041-x.
Richardson, W. S., Wilson, M. C., Nishikawa, J., & Hayward, R. S. A. (1995). The well-built clinical question: A key to evidence-based decisions. ACP Journal Club, 123, A12-13. https://doi.org/10.7326/ACPJC-1995-123-3-A12.
Rogers, S. J., & Vismara, L. A. (2008). Evidence-based comprehensive treatments for early autism. Journal of Clinical Child & Adolescent Psychology, 37(1), 8–38. https://doi.org/10.1080/15374410701817808.
Sackett, D. L., Rosenberg, W. M. C., Muir Gray, J. A., Haynes, R. B., & Richardson, W. S. (1996). Evidence based medicine: What it is and what it isn’t. British Medical Journal, 312(7023), 71–72. https://doi.org/10.1136/bmj.312.7023.71.
Sam, A. M., Cox, A. W., Savage, M. N., Waters, V., & Odom, S. L. (2020a). Disseminating information on evidence-based practices for children and youth with autism spectrum disorder: AFIRM. Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s10803-019-03945-x.
Sam, A.M., Odom, S.L., Tomaszewski, B., Perkins, Y., & Cox, A. W. (2020). Employing evidence-based practices for children with autism in elementary schools. Journal of Autism and Developmental Disorders, (2020). Online prepublication. https://doi.org/10.1007/s10803-020-04706-x
Sandbank, M., Bottema-Beutel, K., Crowley, S., Cassidy, M., Dunham, K., Feldman, J. I., et al. (2020). Project AIM: Autism intervention meta-analysis for studies of young children. Psychological Bulletin, 146(1), 1–29. https://doi.org/10.1037/bul0000215.
Shadish, W. R., Cook, T. D., & Campbell, D. T. (2002). Experimental and quasi-experimental designs for generalized causal inference. Houghton Mifflin.
Shattuck, P. T., Rast, J. E., Roux, A. M., Anderson, K. A., Benevides, T., Garfield, T., McGhee, G., Hassrick, E., & Kuo, A. (2018). National autism indicators report: High school students on the autism spectrum. Life Course Outcomes Program, A.J. Drexel Autism Institute, Drexel University. https://drexel.edu/autismoutcomes/publications-and-reports/publications/National-Autism-Indicators-Report-High-School-Students-on-the-Autism-Spectrum/
Simpson, R. L. (2005). Evidence-based practices and students with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 20(3), 140–149. https://doi.org/10.1177/10883576050200030201.
Siri, K., & Lyons, T. (2014). Cutting edge therapies for autism (4th ed.). Skyhorse Publishing.
Smith, T. (2013). What is evidence-based behavior analysis? The Behavior Analyst, 36(1), 7–33. https://doi.org/10.1007/bf03392290.
Smith, T., Groen, A. D., & Wynn, J. W. (2000). Randomized trial of intensive early intervention for children with pervasive developmental disorder. American Journal on Mental Retardation, 105(4), 269–285. https://doi.org/10.1352/0895-8017(2000)105%3c0269:RTOIEI%3e2.0.CO;2.
Stahmer, A. C., Suhrheinrich, J., Reed, S., Schreibman, L., & Bolduc, C. (2011). Classroom pivotal response teaching for children with autism. New York: Guilford Press.
Steinbrenner, J. R., Hume, K., Odom, S. L., Morin, K. L., Nowell, S. W., Tomaszewski, B., Szendrey, S., McIntyre, N. S., Yucesoy-Ozkan, S., & Savage, M. N. (2020). Evidence-based practices for children, youth, and young adults with Autism. The University of North Carolina at Chapel Hill, Frank Porter Graham Child Development Institute, National Clearinghouse on Autism Evidence and Practice Review Team. https://ncaep.fpg.unc.edu/sites/ncaep.fpg.unc.edu/files/imce/documents/EBP%20Report%202020.pdf
Strain, P. S., & Bovey, E. H. (2011). Randomized, controlled trial of the LEAP model of early intervention for young children with autism spectrum disorders. Topics in Early Childhood Special Education, 31(3), 133–154. https://doi.org/10.1177/0271121411408740.
Turner, K. M., Markie-Dadds, C., & Sanders, M. R. (2010). Practitioner’s manual for primary care triple P. Triple P International Pty. https://www.triplep.net/glo-en/the-triple-p-system-at-work/training-and-delivery/resources/
Urbanowicz, A., Nicolaidis, C., den Houting, J., Shore, S. M., Gaudion, K., Girdler, S., & Savarese, R. J. (2019). An expert discussion on strengths-based approaches in autism. Autism in Adulthood, 1(2), 82–89. https://doi.org/10.1089/aut.2019.29002.aju.
U.S. Department of Education, National Center for Education Statistics, Common Core of Data (CCD), State Nonfiscal Survey of Public Elementary and Secondary Education,”2000–01 and 2015–16. https://nces.ed.gov/programs/coe/indicator_cge.asp#info
Watling, R., & Hauer, S. (2015). Effectiveness of Ayres Sensory IntegrationR and sensory-based interventions for people with autism spectrum disorder: A systematic review. American Journal of Occupational Therapy, 69(5), 6905180030p.1–11. https://doi.org/10.5014/ajot.2015.018051
West, E. A., Travers, J. C., Kemper, T. D., Liberty, L. M., Cote, D. L., McCollow, M. M., & Brusnahan, L. L. (2016). Racial and ethnic diversity of participants in research supporting evidence-based practices for learners with autism spectrum disorder. Journal of Special Education, 50(3), 151–163. https://doi.org/10.1177/0022466916632495
What Works Clearinghouse. (2020). What Works Clearinghouse standards handbook, version 4.1. U.S. Department of Education, Institute of Education Sciences, National Center for Education Evaluation and Regional Assistance. https://ies.ed.gov/ncee/wwc/Docs/referenceresources/WWC-Standards-Handbook-v4-1-508.pdf
Wong, C., Odom, S. L., Hume, K. A., Cox, A. W., Fettig, A., Kucharczyk, S., Brock, M. E., Plavnick, J. B., Fleury, V. P., & Schultz, T. R. (2014). Evidence-based practices for children, youth, and young adults with autism spectrum disorder. The University of North Carolina, Frank Porter Graham Child Development Institute, Autism Evidence-Based Practice Review Group. https://autismpdc.fpg.unc.edu/sites/autismpdc.fpg.unc.edu/files/imce/documents/2014-EBP-Report.pdf
Wong, C., Odom, S. L., Hume, K. A., Cox, A. W., Fettig, A., Kucharczyk, S., et al. (2015). Evidence-based practices for children, youth, and young adults with autism spectrum disorder: A comprehensive review. Journal of Autism and Developmental Disorders, 45(7), 1951–1966. https://doi.org/10.1007/s10803-014-2351-z.
Acknowledgments
Support for this project was provided by the Institute of Education Sciences, U.S. Department of Education through Grant R324B160038 (Postdoctoral Training Program on Special Education Research) awarded to University of North Carolina at Chapel Hill and the U.S. National Institutes of Health, Grant T32HD040127. The opinions expressed represent those of the authors and do not represent the U.S. Department of Education or the U.S. National Institutes of Health. Funding for this work was also provided by the Ireland Foundation, Mr. John E. Rucker, and the Frank Porter Graham Child Development Institute. The authors wish to acknowledge the support of the following individuals at the University of North Carolina and the Frank Porter Graham Child Development Institute who provided assistance, feedback, and technical support during the course of the project: Amelia Gibson, Kathleen Thomas, Ann Sam, Victoria Waters, Jeff Alpi, Andrea Ross, Stephanie Ridley, Luke Hayek, Lindsay Rentschler, Tara Regan, Coral Morrow, Crisma Emmanuel, Benjamin Carter, Juliet Alegria, Mary Tran, and Ashley Freuler.
Author information
Authors and Affiliations
Contributions
KH, JD, and SO designed and directed the study. All authors participated in the systematic review process and contributed to data analysis. KH, JD, and SO wrote the manuscript with the support of and review by the full author team.
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hume, K., Steinbrenner, J.R., Odom, S.L. et al. Evidence-Based Practices for Children, Youth, and Young Adults with Autism: Third Generation Review. J Autism Dev Disord 51, 4013–4032 (2021). https://doi.org/10.1007/s10803-020-04844-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-020-04844-2