
Abstract
Objective
To identify what matters to clinicians and patients when discussing cancer medicines’ impact on health-related quality of life (HRQoL).
Methods
A framework of HRQoL domain/domain elements was developed, informed by analysis of published patient reported outcome measures (PROMs), applicable to prostate cancer. Using mixed methods (eDelphi, Nominal Group Technique and questionnaire), prostate cancer clinicians and patients attending prostate cancer clinics and support groups were asked which domains/domain elements would be important to them when discussing the impact prostate cancer medicines have on their HRQoL.
Results
Twenty-one clinicians and 71 patients participated from the West of Scotland. Clinicians and patients identified 53/62 domain elements across seven domains as important, of which 32 (60%) were common to both groups. Clinicians placed more importance than patients on Mood & Emotion; in contrast, patients placed importance on a broader range of Symptoms & Side Effects, being informed about their care, and having effective healthcare professional collaboration.
Conclusion
This study provides insight into the similarities and differences between what clinicians and patients think is important when discussing the impact of cancer medicines on HRQoL. Future research should involve exploring the potential for consistency of medicines PROMs across different cancer types to support patient-clinician communication and drive improvements in care.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cancer is the second leading cause of death globally [1]. Prostate cancer is the most common cancer among men in Europe, accounting for 24% of all newly diagnosed cancers in 2018 with an estimated 450,000 new diagnoses [2]. While incidence is rising — partly based on more widespread access to testing — survival across Europe has increased [3], mainly due to an increased availability of systemic anticancer therapies (SACT) [4, 5].
As survival rates improve and more patients are living with cancer, a shift away from solely offering supportive palliative care at the end of life [5] has resulted in an interest in assessing Quality of Life (QoL) among cancer patients throughout their journey [6], in addition to standard clinical outcomes such as overall survival. Measurement of health-related quality of life (HRQoL), referring to the impact of health, illness, and treatment on QoL [7], is recognised as important at both the patient and population level. At a patient level, the ability to monitor treatment impact on a patient’s well-being can support patient/clinician decision-making about treatment and care, and may improve outcomes [8]; at the population level, HRQoL is increasingly being considered as part of the assessment of overall clinical effectiveness and the value of cancer medicines [9, 10].
Although assessing patients’ experiences of treatment is a central component of healthcare and, in 2005, Ferrans et al. proposed a model for measuring HRQoL that comprised elements of biological function, symptoms, functionality, general health perceptions, and overall quality of life [7], there is a lack of agreement regarding the method of measuring HRQoL, or what elements should indeed be included as part of a full package of patient care [11,12,13,14,15,16,17]. Research within the field focuses on the use of patient reported outcome measures (PROMs) — a common means of measuring and comparing HRQoL. While PROM tools are frequently and successfully used in clinical trials [18, 19], widespread application of PROMs is uncommon in routine clinical practice. Key barriers regarding their routine use in clinical practice range from misconceptions about the value of PROMs to technical difficulties with integrating suitable tools into clinical workflows, a prerequisite for implementation at scale; furthermore, successful implementation requires frequent and consistent interaction with both healthcare staff as well as patients and their carers, since engaging stakeholders and sustaining the completion of PROMs tools can be challenging [20]. These problems are compounded by the large number of different PROMs tools already available, and the differences in their relevance and applicability depending on context. As the relevance of PROM tools is a factor not only affecting their potential usefulness for clinicians but also the retention of patients engaging with them, the variability of tools available — and the wide range of specific topics covered — poses questions of suitability of individual tools, with implications for future decisions about which tool(s) to choose going forward [10, 21, 22].
Nevertheless, regular collection of PROMs could offer clinicians a more systematically assessed view of how patients are tolerating treatment; support discussions with patients; and facilitate more informed collaborative decision-making with regard to their cancer treatment [8, 21, 23, 24]. Engaging patients, clinicians, other healthcare staff, academics, and policy makers in the design and development of HRQoL PROMs strategies ensures that they meet stakeholder needs and focus on the importance, relevance, and completeness of content of PROMs tools used to support care [21, 25].
The continually evolving prostate cancer treatment landscape comprises a broad range of cancer medicines, which are appropriate for use at different stages of disease [26, 27]. PROMs research in prostate cancer has focused mainly on the impact of the disease on HRQoL and on measuring acute toxicity from systematic anticancer treatments (SACT) [28,29,30]. Less is known about the impact of cancer medicines more generally on a patient’s wellbeing and their supportive care needs.
In line with the Scottish National Cancer Strategy [31], the Cancer Medicines Outcomes Programme (CMOP) is funded by the Scottish Government to test the feasibility of collecting HRQoL data from clinical practice to support clinical decision-making, with a focus on understanding what PROMs data could be collected and utilised as part of routine care, and how best to accomplish this. The aim of this study was to identify what matters to prostate cancer patients and clinicians when discussing the impact of cancer medicines on HRQoL to better understand the care needs of these patients, and inform future PROMs data collection.
Methods
There is an extensive body of work regarding PROMs tools in cancer. However, existing tools being used to assess HRQoL vary in the elements they aim to capture; how well their development is evidenced (including reliability and validity testing); and their overall usefulness. As the landscape of PROMs tools is already vast, it was deemed less useful to design a new PROMs tool for use in cancer medicines. Instead, based on a literature review aimed at identifying available PROMs tools to inform the study material, consensus methods were used to establish which areas of HRQoL represented within existing tools are most important to the study population, with a view to exploring what is valuable in the tools already available. Consensus methods are applied extensively in healthcare research [32,33,34]; a mixed methods approach was adopted in order to accommodate the specific needs of patients and clinicians.
Study material development
PROMs tools relevant for use in a prostate cancer patient population (including generic QoL, health, cancer, and prostate cancer-specific tools) available in English and either reliability and validity tested or endorsed by healthcare organisations were searched for in three databases (PubMed, Science Direct, and Google Scholar). The search terms used were as follows: “PROMs” and its full forms (“patient reported outcome measures”, “patient reported outcomes”); “prostate cancer”; “Quality of Life” and the acronyms “QoL” and “HRQoL”; and “qualitative”. Additional information regarding suitable PROMs tools were provided by members of the research team with experience in cancer PROMs. Literature searches were conducted between December 2016 and May 2017 until no further PROMs tools could be identified, resulting in a total of 30 potentially relevant tools. These were subsequently discussed by the CMOP team — comprising academics as well as clinicians — to ensure relevance to clinical practice; all identified tools were confirmed as relevant.
Using NVivo v11, the 30 identified PROMs tools were coded by one researcher in terms of what each question within these tools addressed. After validation by a second researcher, the coding was used to generate a framework of domains and domain elements; this framework was then validated against published theories and definitions of QoL and HRQoL by conducting a matching exercise, ensuring that all vital elements were captured [7, 35,36,37]. The developed framework, comprising nine domains and 70 domain elements (Fig. 1), was subsequently used to generate the data collection tools used throughout this study (eDelphi questionnaires, NGT workbooks, and Clinic Questionnaires).

List of HRQoL domains (n = 9) and domain elements (n = 70) derived from selected PROMs tools (n = 30)
Identification of study participants
Clinicians — including oncologists, urologists, pharmacists, nurses, dieticians, and physiotherapists — engaged in prostate cancer clinics in hospitals within the West of Scotland Cancer Network (WoSCAN) were eligible to participate and were identified through the CMOP clinical network.
Patients eligible for participation were identified in two ways:
-
Attendance of either one of two prostate cancer support groups hosted in NHS Greater Glasgow & Clyde (NHS GGC); support groups were identified via internet search.
-
Attendance at prostate cancer clinics in two NHS GGC hospitals, and currently or previously on prescribed medicines for prostate cancer treatment; clinics were identified via the CMOP clinical network.
Data collection and analyses
Clinicians
Clinicians were invited via email to participate in an eDelphi, consisting of two rounds and taking place between October and December 2017. All potential participants were provided with electronic participant information sheets (PIS) and consent forms to complete prior to taking part.
The first eDelphi questionnaire asked clinicians to rank the importance of the nine framework domains (Fig. 1) in relation to discussing with patients the impact of medicines on their HRQoL (1 — least important/relevant; to 9 —most important/relevant). Responses were analysed by summing the rank scores and calculating the median/interquartile range (IQR) for each domain; domains with median scores on or above the pre-defined threshold (the mid-point of the scale, i.e. 5) were retained. Domains with median scores below the threshold but with a wide IQR encompassing the threshold were reviewed by the CMOP team [38].
The second eDelphi questionnaire presented the retained domains back to clinicians and asked them to rank each of the domain’s elements from least to most important/relevant. Responses were analysed as per eDelphi 1; domain elements with median scores on or above the pre-defined threshold (the mid-point of the scale, which varied depending on the number of domain elements per domain) were retained, while those below the threshold but with a wide IQR encompassing the threshold were reviewed by the CMOP team.
Patients
Researchers visited prostate cancer support groups on several occasions between February and July 2018. On these days, patients who were present were invited to participate in a group consensus approach called Nominal Group Technique (NGT) [39], and were provided with PIS and consent forms to complete prior to commencement of group activities.
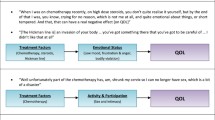
Each NGT focused on a different domain and its associated elements, and lasted 1–1.5 h. Participants were led through a structured process to consider the importance of the domain elements previously identified through eDelphi 1 in relation to the impact of medicines on their HRQoL (Fig. 2). The process involved participants writing their thoughts on each domain element in the NGT workbook; verbalising these thoughts to the group one by one; an open group discussion; individual scoring of each domain element using a Likert scale (1 — not important at all; to 5 — extremely important); collation of scores to generate a ranked list of the domain elements by the researcher; and presenting the established list back to the group for discussion, followed by anonymised voting to indicate group consensus.

Data collection methods applied for clinicians and patients
Additionally, patients attending prostate cancer clinics between June and August 2018 were recruited by the consulting clinicians, who introduced the study to eligible patients. If interested, patients were referred to the researcher’s present in-clinic; the researchers explained the implications of participation and provided PIS and consent forms. Participants then received the Clinic Questionnaire (a revised version of the NGT workbook comprising all domains and domain element as identified through eDelphi 1; Fig. 2). They were informed that completed questionnaires could be deposited into a sealed box placed at the clinic reception; they also received a pre-stamped return envelope in case they preferred completing the questionnaire at home.
Individual patients’ Likert scores from the NGTs and the Clinic Questionnaires were collated and analysed by calculating medians; domain elements with a median Likert score above the pre-defined threshold (the mid-point of the scale, i.e. 3) were retained. The qualitative data from NGT discussions and free text comments in the questionnaires were transcribed, validated, and analysed using NVivo v11 to capture the patients’ voice and provide context as to why specific domain elements were important to the patient population [40].
Results
Participants
Of 146 invited clinicians, 21 participated in eDelphi 1, all of whom progressed to complete eDelphi 2. Clinicians represented various roles (8 oncologists, 4 urologists, 5 nurses, and 4 pharmacists), with experience in their current role ranging from < 1 to 17 years; mean [SD] age was 46.5 [9.6] years, and 57.1% (n = 12) were female.
Thirty unique patients participated in the NGTs; the mean [SD] age was 68.8 [6.6] years, and patients had lived with prostate cancer for a median of 2.75 [IQR 1–9] years. The Clinic Questionnaire was completed by 41 patients with a mean [SD] age of 73.8 [7.5] years.
Framework domains
Six out of the original nine domains received a median rank score above the pre-defined threshold in eDelphi 1, and three domains had a median score below the threshold but with a wide IQR containing the threshold. While the former were retained, two of the latter were removed following review by the CMOP team (“Patients experience of the Healthcare System” and “Spirituality”). The resulting framework therefore comprised seven domains, with a total of 62 domain elements (between 3 and 15 elements in each domain).
Framework domain elements
Following analysis and review of responses obtained through eDelphi 2, 43 domain elements were identified as being important to clinicians; based on analyses of responses from NGTs and Clinic Questionnaires, 42 domain elements were identified as being important to patients. Figure 3 illustrates that 32 domain elements across the seven domains were important to both clinicians and patients, with a further 11 and 10 specific to clinicians and patients, respectively; while clinicians placed more importance on certain elements of “Mood & Emotion”, patients highlighted additional aspects of “Symptoms & Side Effects”, as well as elements around their information and communication needs. Further details can be found in Supplementary file 1.

Health-related quality of life domain elements (n = 53) important to clinicians and patients
Comparing the results obtained through NGTs and Clinic Questionnaires showed that clinic patients were most concerned with issues relating to symptoms and side effects, whereas support group patients focused on aspects of living with cancer and mental health impacts (Supplementary file 2).
Patient voice
The patient voice, which provides context to the physical, emotional, and lifestyle impact of cancer medicines treatment on HRQoL, is represented in Table 1; captured from NGTs and Clinic Questionnaires, quotes are aligned with the domains and domain elements of the developed framework.
Discussion
Key findings
The purpose of this study was to identify what matters to prostate cancer patients and clinicians when discussing cancer medicines’ impact on HRQoL. From an analysis of published PROMs tools applicable to prostate cancer, a HRQoL framework composed of nine domains and 70 domain elements was created. Clinicians and patients identified a total of 53 domain elements across seven domains as important when discussing the impact of their cancer treatment, of which 32 (60%) were common to both groups. Interestingly, clinicians placed more importance than patients on “Mood & Emotion”; in contrast, patients placed more importance on a broader range of “Symptoms & Side Effects”, and prioritised being informed about their care and having effective collaboration across healthcare professionals.
Previous literature has focused on the level of agreement or concordance between clinicians and patients in their assessment of HRQoL, including during active cancer treatment (principally SACT) and in palliative care, and agreement is commonly greater when examining physical, objective symptoms (e.g. vomiting, diarrhoea) rather than subjective/psychological symptoms (e.g. fatigue, anxiety) [11,12,13,14,15,16,17, 41]. In our study, we had good agreement between clinicians and patients across a range of both physical (“Symptoms and Side Effects”, “Functionality & Day to Day Living”) and psychological (“Mood & Emotion”) domains (Fig. 3). Notably, patients identified a broader range of additional “Symptoms & Side Effects” elements as important. This difference might in part be attributable to clinicians underestimating the severity of physical symptoms, as highlighted in other studies [14, 22]. In contrast, clinicians identified a wider range of “Mood & Emotions” elements as important; although patients signalled their need for broad support (e.g. including “Interacting with Others with Cancer”), they may not necessarily expect this solely to be accessed through their clinician, but through signposting to other systems such as support groups.
Interestingly, we observed that patients who completed clinic questionnaires placed greater importance on a wider range of symptoms and side effects in comparison to those who participated in the support group NGTs, whereas patients recruited from support groups also prioritised elements from the following domains: “Functionality & Day to Day Living”; “Relationships and Social Life”; and “Mood and Emotion” (supplementary file 2). This variation in prioritisation of HRQoL domains is in agreement with the wider evidence base that shows patients may have discrete information needs across their cancer journey, influenced by multiple factors including the different treatments available to patients throughout their illness; the life-limiting side effects these treatments can bring; and how they impact on a patient’s support and care needs [42, 43]. Clinicians need to be cognisant of patients’ diverse and changing areas of importance, and more systematic gathering and exchange of information across the patient journey could better support dialogues as part of shared decision-making and supportive care.
Strengths and limitations
To our knowledge, this is the first study to examine specifically clinicians’ and patients’ perspectives of what areas of HRQoL matter and are important to understanding the impact of cancer medicines, rather than the level of agreement or concordance at a point in time when independently assessing HRQoL. We adopted a mixed methods approach, advocated as good practice in health outcomes research [44]. The review of the literature to develop a framework of domains exploited established knowledge and formed the basis of the study materials; we also provided the participants the opportunity to contribute any additional domain/domain elements that they felt were important but were not represented. We did not ask participants to generate their own domains and domain elements, which may be perceived as a study limitation. However, we perceived this as too cognitively demanding, and it may have resulted in a brief, limited list, while not benefitting from the existing evidence base.
We chose to engage with patients from two diverse settings (i.e. patient support group in a non-healthcare setting and a hospital clinic) to understand better any influence on considering HRQoL. Although this required two different methods of data collection in these divergent environments (NGT and clinic questionnaires), both methods contained the same domain/domain elements. NGT participants may have been influenced by their peers’ opinions in the discussion prior to scoring; nevertheless, participants scored each domain element individually, and these data were used in the quantitative analysis (Fig. 3, Supplementary file 1). The NGT also enabled the capture of group discussions, thereby adding a helpful patient voice to the quantitative data interpretation (Table 1).
We did not document where the patients were on their cancer pathway, only that they had received at least one cancer medicine, and acknowledge that this may impact the generalisability of our findings. We also recognise the potential bias in sampling as patients may attend support groups for specific emotional or information-based needs appropriate for this setting, perhaps related to having negative or less favourable experiences of treatment.
Similarly, the overall number of clinicians participating in the first Delphi phase of this project was limited, and participating clinicians may not be a representative sample; this is of particular relevance as results from this first phase informed all subsequent stages. Nevertheless, we do not expect this to have a substantial impact on our findings since participants represented a broad spectrum of experiences, both in terms of profession and years of clinical practice, and it has been acknowledged that the composition of Delphi panels — and its combined expertise in relation to the topic in question — is more important than its size in order to elicit meaningful responses [45].
Future directions for PROMs use in clinical practice
Within the evolving evidence base, there is a rapidly growing interest in how PROMs can be streamlined into routine clinical practice to provide best supportive care. Recent publications discuss the potential benefits of broad PROMs adoption within healthcare systems to support better communication between patients and clinicians and inform improvements in service provision; this is in line with our study findings suggesting that more consistent gathering and exchange of information across the patient journey could support dialogues between patients and their clinicians as part of shared decision-making and supportive care. Ideally, going forward, dynamic PROMs tools — modifiable in order to be adaptive to changing circumstances — should be integrated into routine clinical practice to enable this. For example, this could involve the consistent use of PROMs tools that have questions relevant to the impacts of specific treatments on HRQoL, alongside other PROMs tools depending on the patient’s priorities or care needs.
Future research should consider how findings of this study can support the use and/or adaptation of established PROMs, i.e. how fit for purpose and complete present PROMs tools are to meet identified needs. A programme of work to assess and adopt/adapt PROMs collection and utilisation through co-design with stakeholders (and integration within cancer care pathways) should be progressed. Moving forward, thought should also be given to the potential for consistency of medicines PROMs across different cancer types, with cancer medicines often being used across multiple cancers, to support and inform a national cancer medicines PROMs strategy. Such a strategy could better enable the collection and use of PROMs data as part of routine care, support treatment regimes, aid system integration, improve patient care, and facilitate public health impact evaluation.
In line with the vision in Scotland for a strategic co-ordinated approach to the adoption of PROMs [31, 46], our ongoing work involves matching the study output domains and domain elements prioritised by patients and clinicians to recognised, validated PROMs tools; and co-designing a digital prototype for patients to input PROMs and a clinical dashboard integrated within the clinical health information technology system. Our ambition is to explore further the potential level of standardisation of PROMs in content, layout, and appearance to minimise burden on patients through their cancer journey, and for clinicians as they manage patients across multiple diseases and treatments. This ambition is shared with colleagues nationally and internationally, calling for a more efficient co-ordinated approach to the adoption and assessment of PROMs within health systems if we are to realise the benefits for patients and society [10, 21].
Conclusion
This study provides insight into the similarities and differences between what prostate cancer clinicians and patients wish to discuss regarding the impact cancer medicines have on HRQoL. There was good consensus between clinicians and patients but also some interesting differences were identified, which warrant further research. Such research should also consider exploring the potential for consistency of medicines PROMs across different cancer types to support patient-clinician communication and drive improvements in supportive care.
Data availability
There is no data available.
Code availability
NA.
References
World Health Organisation. Cancer: key facts. 2018 12 September 2018; Available from: https://www.who.int/news-room/fact-sheets/detail/cancer.
Rawla, P., (2019) Epidemiology of prostate cancer. World Journal of Oncology 10(2): p. 63–89. https://doi.org/10.14740/wjon1191
Crocetti, E., (2015) Epidemiology of prostate cancer in Europe [Internet Resource], European Commission. Available from: https://publications.jrc.ec.europa.eu/repository/handle/JRC101382
Penson DF et al (2008) Prostate cancer: epidemiology and health-related quality of life. Urology 72(6):S3-11. https://doi.org/10.1016/j.urology.2008.10.006
Dellis A et al (2019) Management of advanced prostate cancer: a systematic review of existing guidelines and recommendations. Cancer Treat Rev 73:54–61. https://doi.org/10.1016/j.ctrv.2018.11.005
Forgione M et al (2019) Satisfaction with care in men with prostate cancer. Eur J Cancer Care 28(4):e13028. https://doi.org/10.1111/ecc.13028
Ferrans CE et al (2005) Conceptual model of health-related quality of life. J Nurs Scholarsh 37(4):336–342. https://doi.org/10.1111/j.1547-5069.2005.00058.x
Basch E et al (2017) Overall survival results of a trial assessing patient-reported outcomes for symptom monitoring during routine cancer treatment. JAMA 318(2):197–198. https://doi.org/10.1001/jama.2017.7156
Davis C et al (2017) Availability of evidence of benefits on overall survival and quality of life of cancer drugs approved by European Medicines Agency: retrospective cohort study of drug approvals 2009–13. BMJ 359:j4530. https://doi.org/10.1136/bmj.j4530
Basch E, Wilfong L, Schrag D (2020) Adding patient-reported outcomes to Medicare’s oncology value-based payment model. JAMA 323(3):1538–3598. https://doi.org/10.1001/jama.2019.19970
Atkinson TM et al (2012) Reliability of adverse symptom event reporting by clinicians. Qual Life Res 21(7):1159–1164. https://doi.org/10.1007/s11136-011-0031-4
Basch E et al (2006) Patient versus clinician symptom reporting using the National Cancer Institute Common Terminology Criteria for Adverse Events: results of a questionnaire-based study. Lancet Oncology 7(11):903–909. https://doi.org/10.1016/S1470-2045(06)70910-X
Basch E et al (2009) Adverse symptom event reporting by patients vs clinicians: relationships with clinical outcomes. J Natl Cancer Inst 101(23):1624–1632. https://doi.org/10.1093/jnci/djp386
Brunelli C et al (1998) Quality-of-life evaluation : when do terminal cancer patients and health-care providers agree? J Pain Symptom Manage 15(3):151–158. https://doi.org/10.1016/s0885-3924(97)00351-5
Chandwani KD et al (2017) Lack of patient-clinician concordance in cancer patients: its relation with patient variables. J Pain Symptom Manage 53(6):988–998. https://doi.org/10.1016/j.jpainsymman.2016.12.347
Chidambaram, S., et al., (2014) Patient and provider concordance on symptoms during the oncology outpatient clinic visit. Journal of Community and Supportive Oncology, 12(10): p. 370–7. https://doi.org/10.12788/jcso.0080.
Nekolaichuk CL et al (1999) A comparison of patient and proxy symptom assessments in advanced cancer patients. Palliat Med 13(4):311–323. https://doi.org/10.1191/026921699675854885
Efficace F et al (2014) Patient-reported outcomes in randomised controlled trials of prostate cancer: methodological quality and impact on clinical decision making. Eur Urol 66(3):416–427. https://doi.org/10.1016/j.eururo.2013.10.017
Velikova G et al (2004) Measuring quality of life in routine oncology practice improves communication and patient well-being: a randomized controlled trial. J Clin Oncol 22(4):714–724. https://doi.org/10.1200/JCO.2004.06.078
Roberts NA et al (2020) Statistical process control assessed implementation fidelity of patient-reported outcome measures (PROMs) in routine care. J Clin Epidemiol 127:76–86. https://doi.org/10.1016/j.jclinepi.2020.06.022
Calvert M et al (2019) Maximising the impact of patient reported outcome assessment for patients and society. BMJ 364:k5267. https://doi.org/10.1136/bmj.k5267
Penedo FJ et al (2020) The increasing value of eHealth in the delivery of patient-centred cancer care. Lancet Oncology 21(5):240–251. https://doi.org/10.1016/S1470-2045(20)30021-8
Black N et al (2016) Patient-reported outcomes: pathways to better health, better services, and better societies. Qual Life Res 25(5):1103–1112. https://doi.org/10.1007/s11136-015-1168-3
Devlin, N.J., Appleby, J. (2010) Getting the most out of PROMs: putting health outcomes at the heart of NHS decision-making. Office of Health Economics, 2010.
Camuso N et al (2016) Engaging patients as partners in developing patient-reported outcome measures in cancer-a review of the literature. Support Care Cancer 24(8):3543–3549. https://doi.org/10.1007/s00520-016-3151-0
Caram MEV et al (2019) Patient and provider variables associated with variation in the systemic treatment of advanced prostate cancer. Urology Practice 6(4):234–242. https://doi.org/10.1097/UPJ.0000000000000020
dela Rama F and C. Pratz 2015 Navigating treatment of metastatic castration- resistant prostate cancer: nursing perspectives Clin J Oncol Nurs 19 6 723 732 https://doi.org/10.1188/15.CJON.723-732
Basch, E., et al., (2014) Development of the National Cancer Institute’s patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). Journal of the National Cancer Institute 106(9). https://doi.org/10.1093/jnci/dju244.
Dooley, C., et al., Irish Prostate Cancer Outcomes Research Annual Report 2018. Available from: https://www.ipcor.ie/wp-content/uploads/2019/01/IPCOR_Annual-Report2018_Digital_NEW.pdf
Prostate Cancer UK, Life after prostate cancer diagnosis - study summary. 2018.Available from: https://www.lifeafterprostatecancerdiagnosis.com/wp-content/uploads/sites/50/2019/04/Study-summary-The-Life-After-Prostate-Cancer-Diagnosis-Study_20-pages.pdf
Scottish Government, Recovery and redesign: cancer services - action plan. 2020. Available from: https://www.gov.scot/publications/recovery-redesign-action-plan-cancer-services/
Jones J, Hunter D (1995) Consensus methods for medical and health services research. BMJ 311(7001):376–380. https://doi.org/10.1136/bmj.311.7001.376
G Kleiner-Fisman P Gryfe G Naglie 2013 A patient-based needs assessment for living well with parkinson disease: implementation via nominal group technique Parkinson’s Disease https://doi.org/10.1155/2013/974964
Marino LV et al (2018) The development of a consensus-based nutritional pathway for infants with CHD before surgery using a modified Delphi process. Cardiol Young 28(7):938–948. https://doi.org/10.1017/S1047951118000549
Fitch MI (2008) Supportive care framework. Can Oncol Nurs J 18(1):6–24. https://doi.org/10.5737/1181912x181614
National Cancer Institute (NCI), Common Terminology Criteria for Adverse Events (CTCAE) v4.0., N.I.o. Health, Editor. 2010: Services USDoHH.
Paterson C et al (2015) Identifying the unmet supportive care needs of men living with and beyond prostate cancer: a systematic review. Eur J Oncol Nurs 19(4):405–418. https://doi.org/10.1016/j.ejon.2014.12.007
Boulkedid R et al (2011) Using and reporting the Delphi method for selecting healthcare quality indicators: a systematic review. PLoS ONE 6(6):e20476. https://doi.org/10.1371/journal.pone.0020476
McMillan SS, King M, Tully MP (2016) How to use the nominal group and Delphi techniques. Int J Clin Pharm 38(3):655–662. https://doi.org/10.1007/s11096-016-0257-x
Creswell, J. and V.L. Plano Clark, (2011) Designing and conducting mixed methods research. Thousand Oaks, CA: Sage. Thousand Oaks, CA: Sage Publications.
Sprangers MA, Aaronson NK (1992) The role of health care providers and significant others in evaluating the quality of life of patients with chronic disease: a review. J Clin Epidemiol 45(7):743–760. https://doi.org/10.1016/0895-4356(92)90052-o
Wagland R et al (2019) ‘Very difficult for an ordinary guy’: factors influencing the quality of treatment decision-making amongst men diagnosed with localised and locally advanced prostate cancer: findings from a UK-wide mixed methods study. Patient Educ Couns 102(4):797–803. https://doi.org/10.1016/j.pec.2018.12.004
Fletcher C et al (2017) The information needs of adult cancer survivors across the cancer continuum: a scoping review. Patient Educ Counsel 100(3):383–410. https://doi.org/10.1016/j.pec.2016.10.008
Regnault A et al (2017) Towards the use of mixed methods inquiry as best practice in health outcomes research. J Patient Report Outcomes 2(1):19. https://doi.org/10.1186/s41687-018-0043-8
C Hsu BA Sandford 2007 The Delphi technique: making sense of consensus Pract Assess Res Eval 12 https://doi.org/10.7275/pdz9-th90
Scottish Government, Beating cancer: ambition and action. 2016. Available from: https://www.gov.scot/publications/beating-cancer-ambition-action-2016-update-achievements-new-action-testing-change/
Acknowledgements
We thank NHS Greater Glasgow & Clyde (NHS GGC), the West of Scotland Cancer Network (WoSCaN) CMOP Research Team, Delivery Group, and Programme Board; Clinician and Patient Participants for their support and input into this programme of work; and Pharmacist Gillian Barmack for her contribution to the drafting of this manuscript. We also thank Dr Steven Karlsson Brown, Research Assistant, on the CMOP Programme.
Funding
The Cancer Medicines Outcomes Programme (CMOP) is funded by the Scottish Government.
Author information
Authors and Affiliations
Contributions
Ms Emma Dunlop contributed to study design, participant recruitment, data collection, data analysis, and writing of the manuscript. Miss Aimee Ferguson contributed to writing of the manuscript and interpretation of qualitative analysis. Dr Tanja Mueller contributed to data collection, data validation, data analysis, and review of manuscript. Mrs Kelly Baillie and Ms Julie Clarke contributed to participant recruitment and review of manuscript. Mrs Jennifer Laskey is the clinical lead of the Programme and contributed to study design and review of manuscript. Dr Amanj Kurdi contributed to review of manuscript. Prof Olivia Wu contributed to review of manuscript. Dr Rob Jones contributed to participant recruitment, clinical advice on data collection, and review of manuscript. Dr Hilary Glen provided clinical advice on data collection and reviewed the manuscript. Prof Marion Bennie is the Programme Academic Lead and contributed to continuous review of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
Ethical approval was obtained from the NHS West of Scotland Ethics Committee (Reference Number 17/WS/0202).
Consent to participate
All participants provided written informed consent prior to participation.
Consent for publication
As part of the informed consent process, all participants consented to publication. All authors consent to publication also.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dunlop, E., Ferguson, A., Mueller, T. et al. What matters to patients and clinicians when discussing the impact of cancer medicines on health-related quality of life? Consensus-based mixed methods approach in prostate cancer. Support Care Cancer 30, 3141–3150 (2022). https://doi.org/10.1007/s00520-021-06724-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-021-06724-6