
Abstract
Background
Controversies exist in the best surgical approach (open vs. laparoscopy) to large adrenal tumours without peri-operative evidence of primary carcinoma, mainly due to possible capsular disruption of an unsuspected malignancy. In addition, intra-operative blood loss, conversion rate, operative time, and hospital stay may be increased with laparoscopy. The aims of our study were: (1) to compare clinical outcomes of laparoscopic adrenalectomy for large versus small adrenal tumours and (2) to identify risk factors associated with increased operative time and hospital stay in laparoscopic adrenalectomy.
Methods
This is a multicentre retrospective cohort study in a large patient population (N = 200) who underwent laparoscopic adrenalectomy in 2004–2014 at three Italian academic hospitals. Patients were divided into two cohorts according to tumour size: “large” tumours were defined as ≥5 cm (N = 50) and “small” tumours as <5 cm (N = 150). Further analysis adopting a ≥8 cm (N = 15) cut-off size was performed.
Results
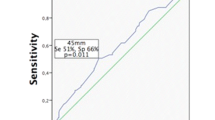
The study groups were comparable in age and gender distribution as well as their tumour characteristics. The operative time (p = 0.671), conversion rate (p = 0.488), intra- (p = 0.876) and post-operative (p = 0.639) complications, and hospital stay (p = 0.229) were similar between groups. With a cut-off size ≥5 cm, the early study period (2004–2009), which included operators’ learning curve, was associated with increased risk of longer operative time (HR 0.57; 95 % CI 0.40–0.82), while American Society of Anaesthesiology score ≥3 was associated with prolonged hospital stay (HR 0.67; 95 % CI 0.47–0.97). Tumour size ≥8 cm was associated with prolonged operative time (HR 0.47; 95 % CI 0.24–0.94).
Conclusions
Surgeons skilled in advanced laparoscopy and adrenal surgery can perform laparoscopic adrenalectomy safely in patients with ≥5-cm tumours with no increase in hospital stay, or conversion rate, although operative time may be increased for ≥8-cm tumours. Surgeon’ experience, size ≥8 cm, and patient comorbidities have the largest impact on operative time and length of hospital stay in laparoscopic large adrenal tumour resection.
Similar content being viewed by others


References
Stefanidis D, Goldfarb M, Kercher KW, Hope WW, Richardson W, Fanelli RD (2013) SAGES guidelines for minimally invasive treatment of adrenal pathology. Surg Endosc 27:3960–3980
Saunders BD, Doherty GM (2004) Laparoscopic adrenalectomy for malignant disease. Lancet Oncol 5:718–726
Shen WT, Sturgeon C, Duh QY (2005) From incidentaloma to adrenocortical carcinoma: the surgical management of adrenal tumors. J Surg Oncol 89:186–192
Donatini G, Caiazzo R, Do Cao C, Aubert S, Zerrweck C, El-Kathib Z, Gauthier T, Leteurtre E, Wemeau JL, Vantyghem MC, Carnaille B, Pattou F (2014) Long-term survival after adrenalectomy for stage I/II adrenocortical carcinoma (ACC): a retrospective comparative cohort study of laparoscopic versus open approach. Ann Surg Oncol 21:284–291
Porpiglia F, Miller BS, Manfredi M, Fiori C, Doherty GM (2011) A debate on laparoscopic versus open adrenalectomy for adrenocortical carcinoma. Horm Cancer 2:372–377
Nih C (2002) NIH state-of-the-science statement on management of the clinically inapparent adrenal mass (“incidentaloma”). NIH Consens State Sci Statements 19:1–25
Asari R, Koperek O, Niederle B (2012) Endoscopic adrenalectomy in large adrenal tumors. Surgery 152:41–49
Conzo G, Musella M, Corcione F, De Palma M, Ferraro F, Palazzo A, Napolitano S, Milone M, Pasquali D, Sinisi AA, Colantuoni V, Santini L (2013) Laparoscopic adrenalectomy, a safe procedure for pheochromocytoma. A retrospective review of clinical series. Int J Surg 11:152–156
Erbil Y, Barbaros U, Karaman G, Bozbora A, Ozarmagan S (2009) The change in the principle of performing laparoscopic adrenalectomy from small to large masses. Int J Surg 7:266–271
MacGillivray DC, Whalen GF, Malchoff CD, Oppenheim DS, Shichman SJ (2002) Laparoscopic resection of large adrenal tumors. Ann Surg Oncol 9:480–485
Castillo OA, Vitagliano G, Secin FP, Kerkebe M, Arellano L (2008) Laparoscopic adrenalectomy for adrenal masses: Does size matter? Urology 71:1138–1141
Walz MK, Petersenn S, Koch JA, Mann K, Neumann HP, Schmid KW (2005) Endoscopic treatment of large primary adrenal tumours. Br J Surg 92:719–723
Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, de Santibanes E, Pekolj J, Slankamenac K, Bassi C, Graf R, Vonlanthen R, Padbury R, Cameron JL, Makuuchi M (2009) The Clavien–Dindo classification of surgical complications: five-year experience. Ann Surg 250:187–196
Gagner M, Pomp A, Heniford BT, Pharand D, Lacroix A (1997) Laparoscopic adrenalectomy: lessons learned from 100 consecutive procedures. Ann Surg 226:238–246 (discussion 246–237)
Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR (1996) A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol 49:1373–1379
Henry JF, Defechereux T, Gramatica L, Raffaelli M (1999) Should laparoscopic approach be proposed for large and/or potentially malignant adrenal tumors? Langenbecks Arch Surg 384:366–369
Kazaryan AM, Mala T, Edwin B (2001) Does tumor size influence the outcome of laparoscopic adrenalectomy? J Laparoendosc Adv Surg Tech A 11:1–4
Parnaby CN, Chong PS, Chisholm L, Farrow J, Connell JM, O’Dwyer PJ (2008) The role of laparoscopic adrenalectomy for adrenal tumours of 6 cm or greater. Surg Endosc 22:617–621
Ramacciato G, Mercantini P, La Torre M, Di Benedetto F, Ercolani G, Ravaioli M, Piccoli M, Melotti G (2008) Is laparoscopic adrenalectomy safe and effective for adrenal masses larger than 7 cm? Surg Endosc 22:516–521
Kouriefs C, Mokbel K, Choy C (2001) Is MRI more accurate than CT in estimating the real size of adrenal tumours? Eur J Surg Oncol 27:487–490
Boylu U, Oommen M, Lee BR, Thomas R (2009) Laparoscopic adrenalectomy for large adrenal masses: pushing the envelope. J Endourol 23:971–975
Hobart MG, Gill IS, Schweizer D, Sung GT, Bravo EL (2000) Laparoscopic adrenalectomy for large-volume (> or =5 cm) adrenal masses. J Endourol 14:149–154
Bhat HS, Nair TB, Sukumar S, Saheed CS, Mathew G, Kumar PG (2007) Laparoscopic adrenalectomy is feasible for large adrenal masses >6 cm. Asian J Surg 30:52–56
Hara I, Kawabata G, Hara S, Yamada Y, Tanaka K, Fujisawa M (2005) Clinical outcomes of laparoscopic adrenalectomy according to tumor size. Int J Urol 12:1022–1027
Tsuru N, Suzuki K, Ushiyama T, Ozono S (2005) Laparoscopic adrenalectomy for large adrenal tumors. J Endourol 19:537–540
Gaujoux S, Bonnet S, Leconte M, Zohar S, Bertherat J, Bertagna X, Dousset B (2011) Risk factors for conversion and complications after unilateral laparoscopic adrenalectomy. Br J Surg 98:1392–1399
Tiberio GA, Solaini L, Arru L, Merigo G, Baiocchi GL, Giulini SM (2013) Factors influencing outcomes in laparoscopic adrenal surgery. Langenbecks Arch Surg 398:735–743
Copeland PM (1984) The incidentally discovered adrenal mass. Ann Surg 199:116–122
Barnett CC Jr, Varma DG, El-Naggar AK, Dackiw AP, Porter GA, Pearson AS, Kudelka AP, Gagel RF, Evans DB, Lee JE (2000) Limitations of size as a criterion in the evaluation of adrenal tumors. Surgery 128:973–982 (discussion 982–973)
Acknowledgments
The authors thank Dr. Simone Sala for his substantial contribution to the revision of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Carlo V. Feo, Mattia Portinari, Umberto Maestroni, Paolo Del Rio, Silvia Severi, Lorenzo Viani, Riccardo Pravisani, Giorgio Soliani, Maria Chiara Zatelli, Maria Rosaria Ambrosio, Jenny Tong, Giovanni Terrosu, and Vittorio Bresadola have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Feo, C.V., Portinari, M., Maestroni, U. et al. Applicability of laparoscopic approach to the resection of large adrenal tumours: a retrospective cohort study on 200 patients. Surg Endosc 30, 3532–3540 (2016). https://doi.org/10.1007/s00464-015-4643-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4643-6