
Abstract
Background
To evaluate the increment in β-hCG levels (%) in the 48-h interval prior to treatment as a predictor of therapeutic success in the management of ectopic pregnancy with methotrexate.
Methods
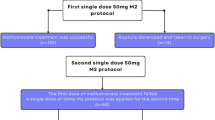
A prospective observational study was carried out between April 2002 and November 2006 at the Federal University of São Paulo in 65 patients with an ectopic pregnancy treated with a single dose of 50 mg/m2 of methotrexate administered intramuscularly. The following predictive factors were evaluated: β-hCG level on the day of hospital admission and the percent increment in β-hCG in the 48-h interval prior to treatment.
Results
Treatment was successful in 49 cases (75.4%). In these cases, β-hCG levels at hospitalization were lower when compared to the levels found in cases of therapeutic failure (1,928.9 vs. 4,828.6 mIU/ml, respectively; P < 0.01), and the increment in β-hCG level in the 48-h interval prior to treatment was smaller (13.1 vs. 36.3%, respectively; P = 0.01). A β-hCG measurement ≤2,685 mIU/ml on the day of hospitalization and an increment in β-hCG level ≤11.1% in the 48 h preceding treatment were factors indicative of therapeutic success with sensitivity of 79.6 and 61.7%, respectively, and specificity of 75 and 81.3%, respectively.
Conclusions
The lower the β-hCG measurement on the day of hospital admission and the lower its increment in the 48-h interval prior to treatment, the greater the likelihood that treatment of ectopic pregnancy with methotrexate will be successful. The margin of safety for treatment with methotrexate is high when β-hCG measurement on the day of hospitalization is ≤2,685 mIU/ml and its increment in the 48 h prior to treatment is ≤11.1%.

Similar content being viewed by others


References
Tanaka T, Hayashi H, Kutsuzawa T, Fujimoto S, Ichinoe K (1982) Treatment of interstitial ectopic pregnancy with methotrexate: report of a successful case. Fertil Steril 37:851–855
Stovall TG, Ling FW, Gray LA, Carson SA, Buster JE (1991) Methotrexate treatment of unruptured ectopic pregnancy. A report of 100 cases. Obstet Gynecol 77:749–753
Caraballo AD, Donoso GR (1998) A 6-year clinical trial of methotrexate therapy in the treatment of ectopic pregnancy. Eur J Obstet Gynecol Reprod Biol 79:167–171
Elito J Jr, Reichmann AP, Uchiyama MN, Camano L (1999) Predictive score for the systemic treatment of unruptured ectopic pregnancy with a single dose of methotrexate. Int J Gynecol Obstet 67:75–79
Menon S, Colins J, Barnhart KT (2007) Establishing a human chorionic gonadotropin cutoff to guide methotrexate treatment of ectopic pregnancy: a systematic review. Fertil Steril 87:481–484
Creinin MD, Washington AE (1993) Cost of ectopic pregnancy management: surgery versus methotrexate. Fertil Steril 60:963–969
Lipscomb GH, Maccord ML, Stovall TG, Huff G, Portera SG, Ling FW (1999) Predictors of success of methotrexate therapy for ectopic pregnancy. Obstet Gynecol 93:590–593
Tawfiq A, Agameya A, Claman P (2000) Predictors of treatment failure for ectopic pregnancy treated with single-dose methotrexate. Fertil Steril 74:877–880
Potter MB, Lepine LA, Jamieson DJ (2003) Predictors of success with methotrexate treatment of tubal ectopic pregnancy at Grady Memorial Hospital. Am J Obstet Gynecol 188:1192–1194
Soares RC, Elito J Jr, Hann KK, Camano L (2004) Endometrial thickness as an orienting factor for the medical treatment of unruptured tubal pregnancy. Acta Obstet Gynecol Scand 83:289–292
Takacs P, Chakhtoura N, De Santis T, Verma U (2005) Evaluation of the relationship between endometrial thickness and failure of single-dose methotrexate in ectopic pregnancy. Arch Gynecol Obstet 6:1–4
Lipscomb GH, Givens VM, Meyer NL, Brand D (2005) Comparison of multidose and single-dose methotrexate protocols for the treatment of ectopic pregnancy. Am J Obstet Gynecol 192:1844–1848
Cacciatore B, Stenman UH, Ylostalo P (1990) Diagnosis of ectopic pregnancy by vaginal ultrasound in a combination with a discriminatory serum hCG level of 1.000mIU/ml. Br J Obstet Gynaecol 97:904–908
Ankun WM, Van der Veen F, Hamerlynk JVTH, Lammes FB (1993) Transvaginal sonography and human chorionic gonadotrophin measurements in suspected ectopic pregnancy; a detailed analysis of a diagnostic approach. Hum Reprod 8:1307–1311
Kadar N, Bohrer M, Kemmann E, Shelden R (1994) The discriminatory human chorionic gonadotropin zone for endovaginal sonography: a prospective, randomized study. Fertil Esteril 61:1016–1020
Graczykowiski JW, Seifer DB (1999) Diagnosis of acute and persistent ectopic pregnancy. Clin Obstet Gynecol 42:9–22
Corsan GH, Karacan M, Qasim S, Bohrer MK, Ransom MX, Kemmann E (1995) Identification of hormonal parameters for successful systemic single-dose methotrexate therapy in ectopic pregnancy. Hum Reprod 10:2719–2722
Gamzu R, Almog B, Levin Y, Avni A, Jaffa A, Lessing JB et al (2002) Efficacy of methotrexate treatment in extrauterine pregnancies defined by stable or increasing human chorionic gonadotropin concentrations. Fertil Steril 77:761–765
Olofsson JI, Poroma IS, Ottander U, Kjellberg L, Damber M (2001) Clinical and pregnancy outcome following ectopic pregnancy; a prospective study comparing expectancy, surgery and systemic methotrexate treatment. Acta Obstet Gynecol Scand 80:744–749
Barnhart KT, Rinaudo P, Hummel A, Pena J, Sammel MD, Chittams J (2003) Acute and chronic presentation of ectopic pregnancy may be two clinical entities. Fertil Steril 80:1345–1351
Nazac A, Gervaise A, Bouyer J, De Tayrac R, Capella-Allouc S, Fernandez H (2003) Predictors of success in methotrexate treatment of women with unruptured tubal pregnancies. Ultrasound Obstet Gynecol 21:181–185
Natale A, Candiani M, Merlo D, Izzo S, Gruft L, Busacca M (2003) Human chorionic gonadotropin level as predictor of trophoblastic infiltration into the tubal wall in ectopic pregnancy: a blinded study. Fertil Steril 79:981–986
Dudley PS, Heard MJ, Sangi-Haghpeykar H, Carson SA, Buster JE (2004) Characterizing ectopic pregnancies that rupture despite treatment with methotrexate. Fertil Steril 82:1374–1378
Hajneius PJ, Mol BW, Bossuyt PM, Ankum WM, Van Der Veen F (2000) Interventions for tubal ectopic pregnancy. Cocharne Database Syst Rev Library Issue 2, CD000324. Update in: Cochrane Database Syst Rev 2007, Issue 1, CD000324
Acknowledgments
The authors would like to express their gratitude to Professors Rita de Cássia Ribeiro Silva (School of Nutrition, Federal University of Bahia, UFBA) and Kleber Pimentel Santos (Bahia State School of Sciences) for their collaboration in the statistical analysis of this study.
Conflict of interest statement
Regarding the article, there is not any potential conflict of interest involving the manuscript authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
da Costa Soares, R., Junior, J.E. & Camano, L. Increment in β-hCG in the 48-h period prior to treatment: a new variable predictive of therapeutic success in the treatment of ectopic pregnancy with methotrexate. Arch Gynecol Obstet 278, 319–324 (2008). https://doi.org/10.1007/s00404-008-0589-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-008-0589-4