
Abstract
Objectives
To evaluate the radiation dose in routine multidetector computed tomography (MDCT) examinations in Italian population.
Methods
This was a retrospective multicentre study included 5,668 patients from 65 radiology departments who had undergone common CT protocols: head, chest, abdomen, chest–abdomen–pelvis (CAP), spine and cardiac. Data included patient characteristics, CT parameters, volumetric CT dose index (CTDIvol) and dose length product (DLP) for each CT acquisition phase. Descriptive statistics were calculated, and a multi-regression analysis was used to outline the main factors affecting exposure.
Results
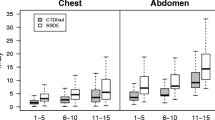
The 75th percentiles of CTDIvol (mGy) and DLP (mGy cm) for whole head were 69 mGy and 1,312 mGy cm, respectively; for chest, 15 mGy and 569 mGy cm; spine, 42 mGy and 888 mGy cm; cardiac, 7 mGy and 131 mGy cm for calcium score, and 61 mGy and 1,208 mGy cm for angiographic CT studies. High variability was present in the DLP of abdomen and CAP protocols, where multiphase examinations dominated (71 % and 73 % respectively): for abdomen, 18 mGy, with 555 and 920 mGy cm in abdomen and abdomen–pelvis acquisitions respectively; for CAP, 17 mGy, with 508, 850 and 1,200 mGy cm in abdomen, abdomen–pelvis and CAP acquisitions respectively.
Conclusion
The results of this survey could help in the definition of updated diagnostic reference levels (DRL).
Key Points
• Radiation dose associated with multidetector CT (MDCT) is an important health issue.
• This national survey assessed dose exposures of 5,668 patients undergoing MDCT.
• Dose indices correlate with BMI, voltage, rotation time, pitch and tube current.
• These results may contribute to an update of national diagnostic reference levels.





Similar content being viewed by others

Abbreviations
- AIFM:
-
Italian Society of Medical Physics
- BMI:
-
body mass index
- CAP:
-
chest–abdomen–pelvis
- CI:
-
confidence interval
- CTDIvol :
-
volumetric computed tomography dose index
- DLP:
-
dose length product
- DRL:
-
diagnostic reference levels
- ECTCM:
-
electrocardiographically controlled tube current modulation
- FOV:
-
field of view
- GEE:
-
generalized estimating equations
- MDCT:
-
multidetector computed tomography
- MV:
-
mean value
- RIS:
-
radiology information system
- SD:
-
standard deviation
- SIRM:
-
Italian Society of Radiology
References
European Commission (1999) European guidelines on quality criteria for computed tomography. EUR 16262 EN. Luxembourg, Office for Official Publications of the European Communities
Bongartz G, Golding SJ, JuriK AG, Leonardi M et al (2008) Quality criteria for multislice computed tomography. Results from a European concerned action on CT (FIGM-CT-2000-2008) Appendix B: European field survey on MDCT 2004. http://MDCT.eu/CT_Quality_Criteria.htm. Accessed 1 Jan 2013
Brenner DJ, Hall EJ (2007) Computed tomography–an increasing source of radiation exposure. N Engl J Med 357:2277–2284
Berrington de Gonzalez A, Mahesh M, Kim KP et al (2009) Projected cancer risks from computed tomographic scans performed in the United States in 2007. Arch Intern Med 169:2071–2077
Marin D, Nelson RC, Schindera ST et al (2010) Low-tubevoltage, high-tube-current multidetector abdominal CT: improved image quality and decreased radiation dose with adaptive statistical iterative reconstruction algorithm–initial clinical experience. Radiology 254:145–153
Kalra MK, Maher MM, Toth TL et al (2004) Techniques and applications of automatic tube current modulation for CT. Radiology 233:649–657
McCollough CH, Bruesewitz MR, Kofler JM Jr (2006) CT dose reduction and dose management tools: overview of available options. Radiographics 26:655
Li J, Udayasankar UK, Toth TL, Seamans J, Small WC, Kalra MK (2007) Automatic patient centering for MDCT: effect on radiation dose. AJR Am J Roentgenol 188:547–552
Kalra MK, Maher MM, Toth TL et al (2004) Strategies for CT radiation dose optimization. Radiology 230:619–628
Hall EJ, Brenner DJ (2008) Cancer risks from diagnostic radiology. BJR 81:362–378
Hendee WR, O’Connor MK (2012) Radiation risks of medical imaging: separating fact from fantasy. Radiology 264:312–321
Decreto Legislativo 26 maggio 2000, n. 187. Gazzetta Ufficiale n. 157 del 7 luglio 2000
Origgi D, Vigorito S, Villa G, Bellomi M, Tosi G (2006) Survey of computed tomography techniques and absorbed dose in Italian hospitals: a comparison between two methods to estimate the dose-length product and the effective dose and verify fulfillment of the diagnostic reference levels. Eur Radiol 16:227–237
Catuzzo P, Aimonetto S, Zenone F, Fanelli G, Marchisio P, Meloni T, Pasquino M, Tofani S (2010) Population exposure to ionizing radiation from CT examinations in Aosta Valley between 2001-2008. BJR 83:1042–1051
Compagnone G, Angelini P, Doenichelli S (2012) Radiation doses to the population of the Emilia-Romagna region from medical exposures. Radiol Med 117:312–332
Shrimpton PC, Hiller MC, Lewis MA, Dunn M (2006) National survey of doses from CT in the UK: 2003. BJR 79:968–980
Brix G, Nagel HD, Stamm G, Veit R, Lechel U, Gribel J, Galanski M (2003) Radiation exposure in multi-slice versus single slice spiral CT: results of a nationwide survey. Eur Radiol 13:1979–1991
Verdun FR, Gutierrez D, Vader JP, Aroua A et al (2008) CT radiation dose in children: a survey to establish age-based diagnostic reference levels in Switzerland. Eur Radiol 18:1980–1986
Galanski M, Nagel HD, Stamm NG (2006) Paediatric CT exposure practise in the Federal Republic of Germany. Result of a nation-wide survey in 2005-2006. Medizinische Hochschule Hannover. http://www.mhhannover.de/fileadmin/kliniken/diagnostische_radiologie/download/Report_German_Paed-CT-Survey_2005_06.pdf. Accessed 1 Jan 2013
Bernier MO, Rehel JL, Brisse HJ, Wu-Zhou X et al (2012) Radiation exposure from CT in early childhood: a French large scale multicentre study. Br J Radiol 85:53–60
Foley SJ, McEntee MF, Rainford LA (2012) Establishment of CT diagnostic reference levels in Ireland. BJR 85:1390–1397
Zarb F, McEntee M, Rainford L (2012) Maltese CT doses from commonly performed examinations demonstrate alignment with published DRLs across Europe. Radiat Prot Dosim 150:198–206
Treier R, Aroua A, Verdun FR, Samara E, Stuessi A, Trueb PR (2010) Patient doses in CT examinations in Switzerland: implementation of national diagnostic reference levels. Radiat Prot Dosim 142:244–254
McCollough CH, Branham T, Herlihy V, Bhargavan M, Robinn L et al (2011) Diagnostic reference levels from the ACR CT accreditation program. J Am Coll Radiol 8:795–803
Roch P, Aubert B (2012) French diagnostic reference levels in diagnostic radiology, computed tomography and nuclear medicine. Radiat Prot Dosim 1–24
Veit R, Guggenberger R, Noßke D, Brix G (2010) Diagnostische Referenzwerte für Röntgenuntersuchungen Radiologe 50:907–912
SIRM SAGO (2010) Censimento Nazionale delle risorse umane e tecnologiche dell’area radiologica. Il Ragiologo Suppl 2:3–39
IMV (2007) Benchmark report CT 2007. IMV Medical Information Division, Illinois US
Liang K, Zeger S (1986) Longitudinal data analysis using generalized linear models. Biometrika 73:13–22
Zeger S, Liang K (1992) An overview of methods for the analysis of longitudinal data. Stat Med 11:1825–1839
Istat (2011) Indagine annuale "Aspetti della vita quotidiana" 2011. www.istat.it. Accessed 1 Jan 2013
International Commission on Radiological Protection (2008) 2007 recommendations of the International Commission on Radiological. Annals of the ICRP, ICRP Publication 103. Pergamon, Oxford
Andoh H, McNulty NJ, Lewis PJ (2013) Improving accuracy in reporting CT scans of oncology patients: assessing the effect of education and feedback interventions on the application of the Response Evaluation Criteria in Solid Tumors (RECIST) criteria. Acad Radiol 20:351–357. doi:10.1016/j.acra.2012.12.002
Perez-Johnston R, Lenhart DK, Sahani DV (2010) CT angiography of the hepatic and pancreatic circulation. Radiol Clin N Am 48:311–330. doi:10.1016/j.rcl.2010.02.021, viii
Frost & Sullivan (2012) Analysis of the US medical computed tomography (CT) imaging system market. www.healthcare.frost.com. Accessed 1 Jan 2013
DDM2 (2011) www.ddmed.eu. Accessed 1 Jan 2013
Pantos I, Thalassinou S, Argentos S, Kelekis NL, Panayiotakis G, Efstathopoulos (2011) Adult patient radiation doses from non-cardiac CT examinations: a review of published results. Br J Radiol 84:293–303
Schilham A, van der Molen AJ, Prokop M, de Jong HW (2010) Overranging at multisection CT: an underestimated source of excess radiation exposure. Radiographics 30:1057–1067
Hausleiter J, Meyer T, Hermann F, Krebs M et al (2009) Estimated radiation dose associated with cardiac CT angiography. JAMA 301:500–507
Wood TJ, Davis AW, Moore CS, Beavis AW, Saunderson JR (2012) Validation of a large scale audit technique for CT dose optimization. Radiat Prot Dosim 150:427–433
Acknowledgments
We are pleased to acknowledge the collaboration of numerous radiologist colleagues and medical physicists (listed in the Appendix) that has allowed the achievement of this large-scale data collection. We are also grateful to the Italian Society of Radiology (SIRM) who financed and supported the study, and to the Italian Society of Medical Physics (AIFM), for its active collaboration.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Participating centres
AOUP Policlinico Palermo, Ospedale P. V. Fazzi Lecce, Ospedale P.O. Spirito Santo Pescara, Ospedali Riuniti Ancona, Ospedale Maggiore Trieste, Azienda Ospedaliero Universitaria Careggi Firenze, A.O OIRM Sant'Anna Torino, Ospedale Belcolle ASL Viterbo, IRCCS Policlinico San Donato Milanese, Fatebenefratelli Sangiovanni Calabita Roma, Istituto Oncologico Veneto IRCCS Padova, Istituto Europeo di Oncologia Milano, Hsr Giglio Cefalù, Ospedale AOU Maggiore della Carità Novara, Ospedale San Donato Usl 8 Arezzo, Ospedale Carlo Poma Mantova, Istituto per la ricerca e la cura del cancro di Candiolo, Fondazione IRCC Policlinico San Matteo Pavia, Ospedale Circolo Fondazione Macchi Varese, Ospedale Niguarda Milano, Istituto Tumori Genova, ASL Cuneo 1, AO SS. Antonio e Biagio e C. Arrigo Alessandria, PO Santa Maria delle Grazie Pozzuoli, Ospedale San Bassiano Ulss3 Bassano del Grappa, Ospedale Santa Maria delle Croci Ravenna, Istituti Ospitalieri Cremona, A.O Città della salute e della scienza Torino, Ospedale Regionale U. Parini Ausl Valle d'aosta, Asl2 Savonese Ospedale Santa Corona Pietra Ligure, San Raffaele Milano, Azienda Ospedaliero Universitaria di Modena Policlinico, Azienda Ospedaliera San Gerardo Monza, Azienda Ospedaliera Polo Universitario L. Sacco Milano, Azienda Sanitaria di Firenze Ospedale del Mugello, Policlinico Universitario Messina, Azienda Sanitaria Locale Torino Ospedale Martini, Ospedale Asl 1 Imperiese Stabilimento Ospedaliero Imperia, Sanremo e Bordighera, Azienda Ospedaliera di Careggi Firenze, ASL 2 Savonese Ospedale Santa Maria di Misericordia Albenga, Azienda Ospedaliera Universitaria Santa Maria della Misericordia Udine, Ospedale Schio Thiene, Fondazione IRCCS Cà Grande Ospedale Maggiore Policlinico Milano, Ospedale Santa Chiara Trento, Asl 3 Genovese Villa Scassi Genova, Istituti Fisioterapici Ospedalieri Regina Elena Roma, Centro Cardiologico Monzino Milano, Fondazione IRCCS Istituto nazionale Tumori Milano, Ulss 20 Verona Ospedale Fracastoro, Azienda Ospedaliera Santa Maria della Misericordia Perugia, Asl Sassari Ospedale Santissima Annunnziata, Spedali Civili di Brescia, Azienda Ospedaliera Provincia Lecco, AOU Ospedale OORR San Giovanni di Dio e Ruggi D'aragona Salerno, Azienda Ospedaliera di Catanzaro Pugliese-Ciaccio, ASL TO 1 Ospedale Evangelico Valdese, Ospedale di Bressanone
Electronic appendix
For each CT examination performed, the phase 2 datasheet included the main data of the patients enrolled in the survey (age, gender, pseudonymous ID number and, if available, the weight and height) and the clinical indication.
For the main technical parameters that can affect dose, the datasheet included: tube voltage, use of automatic (anatomy-based) tube current modulation, fixed tube current value (for acquisitions without automatic modulation), the available current range (for automatic modulated acquisitions), tube rotation time, reconstructed slice thickness, beam collimation, CT field of view (CT acquisition FOV), z-axis length, the use of axial or spiral CT technique, pitch (for spiral acquisitions), reconstruction filter, the use of contrast agent and, if available, the image quality index used and the average mAs. For cardiac acquisitions, the presence of electrocardiographically controlled tube current modulation (ECTCM), the administration of beta-blockers, and the use of prospective vs retrospective acquisition mode were also recorded.
Finally, the dosimetric parameters of each phase were retrieved from the dose reports in terms of mean CTDIvol and Dose Length Product (DLP). The total DLP, referring to the complete patient examination, was also collected for completeness.
Rights and permissions
About this article
Cite this article
Palorini, F., Origgi, D., Granata, C. et al. Adult exposures from MDCT including multiphase studies: first Italian nationwide survey. Eur Radiol 24, 469–483 (2014). https://doi.org/10.1007/s00330-013-3031-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-013-3031-7