
Avoid common mistakes on your manuscript.
Chimeric antigen-receptor T cells, CAR-T cells, are genetically engineered T-cells, and after decades of development, CAR-T constructs are approved for selected relapsed and refractory (r/r) CD19-positive hematological malignancies and are currently being tested in cancer, infectious disease and autoimmunity [1]. About one-third of CAR-T patients require ICU treatment [2, 3]. Here are ten things your hematologist wants you to know about CAR-T cells.
-
1.
Patients with relapsed/refractory diffuse large B cell lymphoma (r/r DLBCL) and r/r B-acute lymphoblastic leukemia (r/r B-ALL) have a dismal prognosis and limited therapeutic options other than CAR-T cells.
DLBCL is the most common subtype of non-Hodgkin lymphoma, and about half of the DLBCL patients become refractory to treatment or relapse, resulting in a dismal prognosis with a median overall survival of only 6.3 months [4, 5]. Similarly, r/r B-ALL has a disastrous prognosis even with allogeneic stem-cell transplantation [6].
Thus, r/r DLBCL and r/r B-ALL patients had very limited therapeutic options, which have dramatically changed with CAR-T cells. In patients responding to CAR-T cell therapy, long-lasting remissions and in some cases possibly even cure are achievable. Therefore, treatment of these patients on the ICU should include both hematologists and critical care specialists in order to optimize prognostication and management.
-
2.
Immunotherapy and CAR-Ts in particular induce a paradigm shift in hematology oncology.
Evasion of immune surveillance as essential capability of cancer cells is one of the hallmarks of cancer [7]. Immune-targeting medications as checkpoint inhibitors have been approved in several indications and are studied as means of replacing chemoradiotherapy [8].
CAR-T cells represent a paradigm shift, as they exhibit a unique efficacy and can induce remissions lasting several years. They might even cure patients with refractory disease; who otherwise do not respond to treatment [9, 10].
-
3.
Patient eligibility for CAR-T is restricted by patient- and disease-characteristics and is assessed in interdisciplinary CAR-T boards.
Two CAR-T cell constructs targeting CD19 have been approved for selected CD19-positive hematological malignancies: axicabtagene ciloleucel (Yescarta, Kite/Gilead) and tisagenlecleucel (Kymriah, Novartis) [3, 9]. For patient eligibility, most centers, including our departments, require a thorough check of eligibility and discussion of each patient in a multidisciplinary board often including ICU physicians.
-
4.
Candidates for CAR-T treatment are at high risk of disease progression during CAR-T manufacturing and often require bridging therapy.
Disease progression is highly probable in patients with aggressive underlying diseases as r/r DLBCL or r/r B-ALL [4]. Thus, the timeline of 3–4(-6) weeks from apheresis to delivery for CAR-T cells is one limiting factor or the application of CAR-T cells. Bridging therapy between apheresis and delivery of CAR-T product using conventional chemoimmunotherapy or targeted therapies is often required and should not be considered as an additional line of treatment. Importantly, the optimal choice and timing of bridging therapies is yet unknown and often limited by patient comorbidities and refractory disease leading to a race between disease progression and CAR-T production. Novel manufacturing techniques allowing fast in-house manufacturing of CAR-T cells within 10-12 days from apheresis are being developed and tested in clinical trials [11].
-
5.
CAR-T are complex living drugs and require elaborate manufacturing on individual patient basis.
CAR-T cells are living cells that are produced individually for every single patient. CAR-T treatment is preceded by a complex process starting with patient identification followed by a chain of interventions aimed at collecting enough functional T-cells and keeping the underlying disease under control while waiting for the functional product to be delivered.
After collecting collection of peripheral blood mononuclear cells by apheresis and shipment to the production facilities, CAR-T cells are manufactured by selection and activation of T-cells, expansion and lenti- or retroviral transduction with the CAR and final quality control before shipment as fresh or cryopreserved badge depending on construct and center.
-
6.
CAR-T induce complete remission in some patients, and responses can persist for years but can take months to develop their full potential.
In contrast to conventional antineoplastic treatments, CAR-T cells are living organisms and their expansion and antineoplastic activity is a dynamic process and yet poorly understood. Complete or partial response 3 months after CAR-T treatment might be predictive of long-term response durability, but many patients initially responding only partially converse to a complete remission even months after treatment [2, 3]. In patients treated with tisagenlecleucel in the JULIET trial, conversion from partial to complete response occurred in 54% of the patients, including conversion 15 to 17 months after initial response in two patients [3].
-
7.
CAR-T centers are highly selected and interdisciplinary.
CAR-T therapy involves multiple coordinated critical procedures as patient selection, bridging treatment, apheresis and management of complications [12]. To date, only selected medical facilities with expertise in cellular therapies and an infrastructure that includes interdisciplinary designated specialists from hematology, intensive care medicine and neurology among others are certified to administer CAR-T cells.
-
8.
CAR-T therapy causes substantial primary and secondary costs.
Enthusiasm for CAR-T therapy was dampened by financial toxicity given the initial list price of $475,000 for tisagenlecleucel and $373,000 for axicabtagene ciloleucel. Importantly, these costs do not cover apheresis, hospital fees, inpatient treatment and treatment of potential toxicities including ICU treatment. Therefore, the treatment of CAR-T patients puts hospitals at high risk of economic losses. Even more, as indications for CAR-T treatment might expand to more frequent conditions including solid tumors in the near future.
-
9.
CAR-T patients suffer from severe long-term immunosuppression.
Candidates for CAR-T treatment have received multiple line of therapy inducing severe immunosuppression. Moreover, they receive lymphodepleting chemotherapy causing prolonged cytopenia [2, 3]. Also, targeting CD-19 can induce prolonged B-cell depletion depending on the highly variable persistence of CAR-T cells, resulting in hypogammaglobulinemia particularly in children [13]. Consequently, about one-fourth of patients (23%) experience infections after CAR-T cell treatment including fungal infections in 5% and life-threatening infections in 4% [14].
-
10.
CAR-T patients are at high risk of tumor- and treatment-associated complications other than cytokine release syndrome (CRS) and neurotoxicity (ICANS).
CAR-T patients are severely immunosuppressed and frequently experience treatment-related toxicities from chemo- and radiotherapy prior to CAR-T treatment [14]. Therefore, considering differential diagnoses to CRS and ICANS is essential, as they may present with similar signs and symptoms as sepsis and septic shock and no clear laboratory or clinical finding safely excludes neither sepsis nor CRS. Thus, a thorough workup and antibiotic treatment is warranted in addition to CRS treatment. Figure 1 indicates potential differential diagnoses in CAR-T patients presenting with critical illness.
Fig. 1 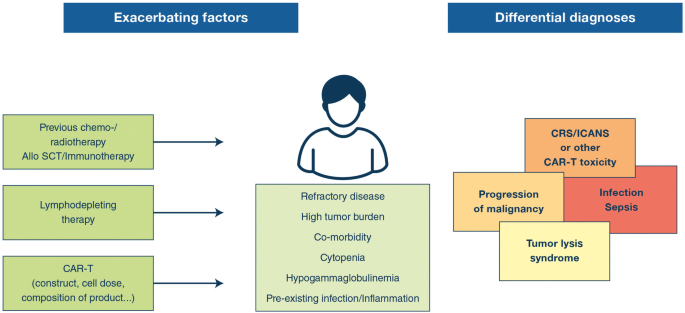
Triggers and differential diagnoses in CAR-T patients presenting with critical illness

References
Holzinger A, Abken H (2019) CAR T Cells: a snapshot on the growing options to design a CAR. Hemasphere 3(1):e172. https://doi.org/10.1097/HS9.0000000000000172
Locke FL, Ghobadi A, Jacobson CA, Miklos DB, Lekakis LJ, Oluwole OO, Lin Y, Braunschweig I, Hill BT, Timmerman JM, Deol A et al (2018) Long-term safety and efficacy of axicabtagene ciloleucel (anti-CD19 CAR T) in refractory large B-cell lymphoma: a multicenter, single arm, phase 1-2 trial. Lancet Oncol 2045(18):31–42
Schuster SJ, Bishop MR, Tam CS et al (2019) Long-term follow-up of tisagenlecleucel in adult patients with relapsed or refractory diffuse large B-cell lymphoma: updated analysis of juliet study. Biol Blood Marrow Transpl 25:S20–S21
Crump M, Neelapu SS, Farooq U et al (2017) Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood 130(16):1800–1808
Maurer MJ, Habermann TM, Shi Q et al (2018) Progression-free survival at 24 months (PFS24) and subsequent outcome for patients with diffuse large B-cell lymphoma (DLBCL) enrolled on randomized clinical trials. Ann Oncol 29(8):1822–1827
Von Stackelberg A, Locatelli F, Zugmaier G et al (2016) Phase I/phase II study of blinatumomab in pediatric patients with relapsed/refractory acute lymphoblastic leukemia. J Clin Oncol 34(36):4381–4389
Hanahan D, Weinberg RA (2011) Hallmarks of cancer: the next generation. Cell 144(5):646–674. https://doi.org/10.1016/j.cell.2011.02.013
Khalil DN, Smith EL, Brentjens RJ, Wolchok JD (2016) The future of cancer treatment: immunomodulation, CARs and combination immunotherapy. Nat Rev Clin Oncol 13(5):273–290
Locke FL, Ghobadi A, Jacobson CA et al (2019) Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, phase 1–2 trial. Lancet Oncol 20(1):31–42. https://doi.org/10.1016/S1470-2045(18)30864-7
Schuster SJ, Bishop MR, Tam CS et al (2018) Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N Engl J Med 380(1):45–56
Lock D, Mockel-Tenbrinck N, Drechsel K et al (2017) Automated manufacturing of potent CD20-directed chimeric antigen receptor T cells for clinical use. Hum Gene Ther 28(10):914–925
June CH, Sadelain M (2018) Chimeric antigen receptor therapy. N Engl J Med 379(1):64–73
Maude SL, Laetsch TW, Buechner J et al (2018) Tisagenlecleucel in children and young adults with B-cell lymphoblastic leukemia. N Engl J Med 378(5):439–448
Hill JA, Li D, Hay KA et al (2018) Infectious complications of CD19-targeted chimeric antigen receptor-modified T-cell immunotherapy. Blood 131(1):121–130
Acknowledgements
Open Access funding provided by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
BB has received research grants from Astellas, Gilead Sciences and MSD and speaker fees from Astellas, Celgene, Johnson & Johnson, Gilead Sciences, MSD, Novartis and Takeda and has been a consultant to Gilead Sciences, MSD, Novartis and Takeda.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Böll, B., Subklewe, M. & von Bergwelt-Baildon, M. Ten things the hematologist wants you to know about CAR-T cells. Intensive Care Med 46, 1243–1245 (2020). https://doi.org/10.1007/s00134-020-06002-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-020-06002-9