
Abstract
Purpose
To provide evidence-based guidelines for early enteral nutrition (EEN) during critical illness.
Methods
We aimed to compare EEN vs. early parenteral nutrition (PN) and vs. delayed EN. We defined “early” EN as EN started within 48 h independent of type or amount. We listed, a priori, conditions in which EN is often delayed, and performed systematic reviews in 24 such subtopics. If sufficient evidence was available, we performed meta-analyses; if not, we qualitatively summarized the evidence and based our recommendations on expert opinion. We used the GRADE approach for guideline development. The final recommendations were compiled via Delphi rounds.
Results
We formulated 17 recommendations favouring initiation of EEN and seven recommendations favouring delaying EN. We performed five meta-analyses: in unselected critically ill patients, and specifically in traumatic brain injury, severe acute pancreatitis, gastrointestinal (GI) surgery and abdominal trauma. EEN reduced infectious complications in unselected critically ill patients, in patients with severe acute pancreatitis, and after GI surgery. We did not detect any evidence of superiority for early PN or delayed EN over EEN. All recommendations are weak because of the low quality of evidence, with several based only on expert opinion.
Conclusions
We suggest using EEN in the majority of critically ill under certain precautions. In the absence of evidence, we suggest delaying EN in critically ill patients with uncontrolled shock, uncontrolled hypoxaemia and acidosis, uncontrolled upper GI bleeding, gastric aspirate >500 ml/6 h, bowel ischaemia, bowel obstruction, abdominal compartment syndrome, and high-output fistula without distal feeding access.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Existing guidelines recommend initiating enteral nutrition (EN) within the first 24–48 h after intensive care unit (ICU) admission if patients are unable to eat, not clearly defining reasons to delay EN [1–3]. The present guideline is issued by the Working Group on Gastrointestinal Function within the Metabolism, Endocrinology and Nutrition (MEN) Section of the European Society of Intensive Care Medicine (ESICM) and is endorsed by ESICM. Our objective was to provide evidence-based guidelines for early enteral nutrition (EEN) in critically ill patients, focusing on specific clinical conditions frequently associated with delayed EN. Caloric and protein requirements, time to reach targets, type and route of EN, and timing of supplemental or full parenteral nutrition (PN) were not addressed. A full version of the introduction with references is available in Supplement 1.
Methods
A full version of methods with references is available in Supplement 1.
We performed a systematic review of “early” EN (EEN) vs. early parenteral nutrition (PN) and EEN vs. delayed EN in adult critically ill patients. After critical appraisal of identified studies and in accordance with current guidelines [1–3], we defined EEN as EN started within 48 h of admission independent of the type or amount.
Thereafter, we predefined conditions in which EN is frequently delayed and performed a systematic review for each of these questions.
If randomised controlled trials (RCT) were available, we gave an evidence-based recommendation; if not, our recommendations were based on expert opinion (very low quality evidence), as all observational studies evaluating EEN are intrinsically biased, because patients who are less severely ill are more likely to receive and tolerate EEN.
General considerations
We focussed on specific conditions in which EN is frequently delayed and tolerance of EN might be impaired. Therefore, all our recommendations are based on general principles and precaution measures outlined in Table 1 [4–9]. All study questions and recommendations refer to adult critically ill patients.
Results
All recommendations with the final agreed results are presented in Table 2.
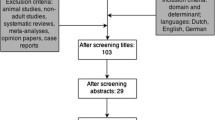
A flow chart with evidence identification process (Supplement 2), number of identified abstracts and assessed full texts for each study question (Supplement 3), Pubmed search formulas (Supplement 4), evidence tables for each question with respective references (Supplement 5), evidence profiles for questions with meta-analyses (Table 3), evidence profiles for additional meta-analyses for Question 1 and 11 (Supplement 6), Forest plots for meta-analyses (Figs. 1, 2 and Supplement 7) are provided.

Forest plots (a mortality; b infections) Question 1A: early EN (EEN) vs. early PN (EPN) in unselected critically ill patients

Forest plots (a mortality; b infections) Question 1B: early EN (EEN) vs. delayed EN (DEN) in unselected critically ill patients
Question 1: Should we use EEN in critically ill adult patients?
The methodology is described in Supplement 1.
Question 1A: Should we use EEN rather than early PN?
Eight trials fulfilled the criteria and were included in meta-analyses (Supplement 5, Table 1A). Results are presented in Fig. 1.
For mortality, we included seven RCTs (2686 patients). EEN did not reduce mortality compared to early PN (RR 0.95; 95% CI 0.76–1.19; P = 0.64; I 2 = 9%). The certainty of evidence was moderate. We rated down for imprecision (Table 3).
For infection, we included seven RCTs (2729 patients). EEN reduced the risk of infections compared to early PN (RR 0.55; 95% CI 0.35–0.86; P = 0.009; I 2 = 65%). The certainty of evidence was low. We rated down for risk of bias and inconsistency (Table 3).
Adding 11 additional studies identified during searches for questions in specified patient groups did not significantly change our results (included studies are presented in Supplement 5, Table 1C; evidence profiles in Supplement 6 and Forest plots in Supplement 7, Fig. 3).
Question 1B: Should we use EEN rather than delay nutritional intake?
Fourteen studies fulfilled the criteria and were included in the meta-analysis (Supplement 5, Table 1B). Results of the meta-analyses on EEN vs. delayed nutritional intake (including delayed EN, oral diet or PN) are presented in Fig. 2.
For mortality, we included 12 RCTs (662 patients). EEN did not reduce mortality compared to delayed nutritional intake (RR 0.76; 95% CI 0.52–1.11; P = 0.149; I 2 = 0%).
For infection, we included 11 RCTs (597 patients). EEN reduced risk of infection compared to delayed EN (RR 0.64; 95% CI 0.46–0.90; P = 0.010; I 2 = 25%).
The certainty of evidence was low. We rated down for risk of bias and imprecision (Table 3).
In one study it was not possible to determine whether early PN was also used in some patients in the EEN group [10]. Adding eight additional studies identified via specific searches did not significantly change the results (included studies are presented in Supplement 5, Table 1D; evidence profiles in Supplement 6 and Forest plots in Supplement 7, Fig. 4).
Recommendation 1. We suggest using EEN in critically ill adult patients rather than early PN (Grade 2C) or delaying EN (Grade 2C).
Question 2: Should we delay EN in patients with shock receiving vasopressors or inotropes?
No RCTs were retrieved. We identified and analysed four prospective cohort studies, four case series/retrospective cohort studies and two reviews (Supplement 5, Table 2).
There is concern that EN in shock further jeopardizes the already impaired splanchnic perfusion. Non-occlusive bowel necrosis or non-occlusive mesenteric ischaemia (NOMI) has been reported in fewer than 1% of patients [11, 12], without evidence for causal relationship between shock, vasopressors, EN and NOMI [11–14]. In a large observational study, EEN (<48 h) in patients with ‘stable’ haemodynamics after fluid resuscitation, whilst receiving at least one vasopressor, was associated with reduced mortality compared to late EN (>48 h) [15]. These results suggest that the use of concomitant vasopressors (especially with stable or decreasing doses) should not preclude a trial of EN, despite a high prevalence of feeding intolerance [16]. In very unstable patients, EN may not have priority and potential positive effects of EN are unlikely to help improve instability. Persisting lactic acidosis may help identify uncontrolled shock.
Recommendation 2. We suggest delaying EN if shock is uncontrolled and haemodynamic and tissue perfusion goals are not reached, but start low dose EN as soon as shock is controlled with fluids and vasopressors/inotropes (Grade 2D).
Question 3:
Should we delay EN in patients with:
-
A.
Hypoxaemia;
-
B.
Hypercapnia;
-
C.
Acidosis?
We found no direct evidence on these subquestions in the literature, and RCTs in this population are unlikely to become available.
The rationale to withhold EN in patients with hypoxaemia, hypercapnia and acidosis is to limit oxygen consumption and CO2 production. However, the process of starving mobilises endogenous stores and is energy-consuming [17]. Acidosis may represent persistent shock and possibly contribute to gut dysfunction. Identifying and treating the cause of shock has priority over the initiation of EN. Similarly, in uncontrolled life-threatening hypoxaemia and hypercapnia, EN should be delayed until the symptoms are resolving.
In patients with acute lung injury, an RCT comparing trophic to full EN for up to 6 days was associated with less gastrointestinal intolerance when compared to full EN, without affecting ventilator-free days, infectious complications, physical function, or survival [7, 18]. There are no data suggesting EN in patients with chronic, subacute, compensated or permissive hypercapnia is unsafe or not feasible.
Recommendation 3. We suggest delaying EN in case of uncontrolled life-threatening hypoxaemia, hypercapnia or acidosis, but using EEN in patients with stable hypoxaemia, and compensated or permissive hypercapnia and acidosis (Grade 2D).
Question 4: Should we delay EN in patients receiving neuromuscular blocking agents?
One prospective study was identified (Supplement 5, Table 4), reporting similar gastric emptying as measured by gastric residual volume (GRV) in sedated patients with or without concomitant use of neuromuscular blocking agents [19]. The critical condition necessitating the use of neuromuscular blocking agents always needs to be considered, but these agents per se should not preclude EN. Analgosedation is known to slow gastric emptying [20]. Increased rate of EN intolerance is expected in deeply sedated patients with/without concomitant use of neuromuscular blocking agents.
Recommendation 4. We suggest that EN should not be delayed solely because of the concomitant use of neuromuscular blocking agents (Grade 2D).
Question 5: Should we delay EN in patients receiving therapeutic hypothermia?
One case series study addressing EN during therapeutic hypothermia was identified [21] (Supplement 5, Table 5).
During therapeutic hypothermia, energy metabolism might be markedly reduced [22, 23] when shivering is prevented. The rationale to withhold EN during therapeutic hypothermia is based on the presumed decrease in gut motility due to hypothermia [24, 25] and required analgosedation [20]. It has been suggested that EN could be successfully administered to these patients [21]. Tolerance to enteral feeding was impaired during hypothermia, but improved during rewarming [21].
Recommendation 5. We suggest starting low dose EEN in patients receiving therapeutic hypothermia and increase the dose after rewarming (Grade 2D).
Question 6: Should we delay EN in patients receiving extracorporeal membrane oxygenation (ECMO)?
No RCTs and no prospective cohort studies were identified. Four case series in adult patients with ECMO were assessed (Supplement 5, Table 6), suggesting that EN is feasible during ECMO.
Recommendation 6. We suggest using EEN in patients receiving ECMO (Grade 2D).
Question 7: Should we delay EN during prone position?
One prospective cross-over, one cohort and three case series studies were identified (Supplement 5, Table 7).
Data on tolerance of EN in prone position are controversial. Observational studies found similar GRVs in prone and supine position [26], whereas poor feeding tolerance was improved with semi-recumbent position during supine periods and prokinetics [27, 28]. Although no RCTs on EN tolerance during prone position are available, reported studies do not support withholding EN in prone position. Gastric emptying seems not to be significantly influenced by prone position and adverse events in most studies not increased.
Recommendation 7. We suggest that EN should not be delayed solely because of prone positioning (Grade 2D).
Remark: We suggest considering early use of prokinetics followed by post-pyloric feeding in case of persisting gastric retention.
Question 8: Should we delay EN in patients with traumatic brain injury?
We identified a Cochrane review with two updates and one recent meta-analysis, comparing early vs. late feeding, independent on the route of nutrition (EN or PN) (Supplement 5, Table 8C). We identified three RCTs comparing EEN vs. early PN, three RCTs comparing EEN vs. delayed EN (one with restricted randomisation), and one RCT comparing early PN vs. delayed EN (Supplement 5, Table 8A).
Question 8A: EEN vs. early PN
Three RCTs (116 patients) were included. EEN compared to early PN in patients with traumatic brain injury did not affect mortality (RR 1.91; 95% CI 0.59–6.18; P = 0.279; I 2 = 0%) or the risk of pneumonia (RR 1.23; 95% CI 0.79–1.90; P = 0.36; I 2 = 0%). The certainty of evidence for mortality outcome was low, for pneumonia it was very low. We rated down for risk of bias and imprecision (Table 3). Supplement 7, Fig. 5.
Question 8B: EEN vs. delayed EN
For mortality, two RCTs (86 patients) were included. EEN did not affect mortality compared to delayed EN (RR 0.66; 95% CI 0.18–2.45; P = 0.53; I 2 = 0%). The certainty of evidence was low. We rated down for imprecision (Table 3).
For pneumonia, three RCTs (118 patients) were included. EEN did not affect the risk of pneumonia compared to delayed EN (RR 0.86; 95% CI 0.55–1.35; P = 0.51; I 2 = 0%). The certainty of evidence was very low. We rated down for risk of bias and imprecision (Table 3). Supplement 7, Fig. 6.
In addition to RCTs, five cohort studies addressing this question were identified (Supplement 5, Table 8B).
Existing evidence did not allow determining or excluding any benefit or harm of EEN, therefore our recommendation is based on expert opinion.
Recommendation 8. We suggest using EEN in patients with traumatic brain injury (Grade 2D).
Question 9: Should we delay EN in patients with stroke (haemorrhagic or ischaemic)?
We identified two RCTs in patients with ischaemic stroke and one retrospective study in patients with hypertensive intracerebral haemorrhage (Supplement 5, Tables 9A, B).
One small RCT compared early vs. delayed EN and reported amelioration of cell-mediated immunity [29]; however, both groups received PN to meet caloric targets from day 1. A large RCT compared EEN (“as soon as possible”) to no nutrition within 7 days and reported a trend towards reduction of long-term mortality (6 months) with EN, with an increased risk of poor neurologic outcome in survivors [30]. An observational study reported reduction in infectious complications with EEN vs. delayed EN [31].
Recommendation 9. We suggest using EEN in patients with stroke (ischaemic or haemorrhagic) (Grade 2D).
Question 10: Should we delay EN in patients with spinal cord injury?
One RCT addressed EEN (<72 h) vs. delayed EN in cervical spinal injury [32]. No differences in outcome variables were identified. One retrospective cohort study addressed safety of EN early after spinal cord injury and reported no major complications [33] (Supplement 5, Tables 10A, B).
Recommendation 10. We suggest using EEN in patients with spinal cord injury (Grade 2D).
Question 11: Should we delay EN in patients with severe acute pancreatitis (SAP)?
We identified five systematic reviews with meta-analyses comparing EN to PN while not considering timing (Supplement 5, Table 11B). All meta-analyses concluded that EN was beneficial in reducing infections and three reported reduced mortality [3, 34, 35].
We identified five RCTs addressing EEN (“early” as defined by the authors) vs. early PN in SAP whereas only two studies defined “early” as <48 h. Three further RCTs addressed EEN vs. early PN and one RCT EEN vs. delayed EN in “predicted SAP”. Two RCTs addressing acute pancreatitis independent of severity and one RCT studying mixed patients undergoing abdominal surgery were not included. Supplement 5, Table 11A.
We performed three separate meta-analyses all comparing EEN vs. early PN: (A) SAP and “early” as defined by the authors of the original study; (B) predicted SAP and “early” as defined by the authors of the original study; (C) predicted SAP and early defined as <48 h.
Question 11A: SAP (as stated by the authors). Early (“early” as defined by the authors) EN vs. PN
For mortality we included five RCTs (283 patients). EEN did not reduce the risk of death compared to PN (RR 0.57; 95% CI 0.23–1.38; P = 0.21; I 2 = 35.1%). The certainty of evidence was low. We rated down for imprecision (Table 3).
For any infections we included five RCTs (283 patients). EEN reduced the risk of infections compared to PN (RR 0.48; 95% CI 0.23–0.98; P = 0.045; I 2 = 76%). The certainty of evidence was low. We rated down for inconsistency and imprecision (Table 3).
For pancreatic infections we included four RCTs (233 patients). EEN reduced the risk of pancreatic infections compared to PN (RR 0.33; 95% CI 0.21–0.52; P < 0.0001; I 2 = 0%) The certainty of evidence was low. We rated down for risk of bias and imprecision (Table 3). Supplement 7, Fig. 7.
Question 11B: Predicted SAP. Early (“early” as defined by the authors) EN vs. PN
For mortality we included eight RCTs (417 patients). EEN did not reduce the risk of death compared to PN (RR 0.50; 95% CI 0.22–1.13; P = 0.09; I 2 = 38%). The certainty of evidence was low. We rated down for imprecision (Supplement 6).
For any infections we included eight RCTs (417 patients). EEN reduced the risk of infections compared to PN (RR 0.53; 95% CI 0.30–0.91; P = 0.023; I 2 = 63.5%). The certainty of evidence was low. We rated down for risk of bias and inconsistency (Supplement 6).
For pancreatic infections we included five RCTs (202 patients). The use of EEN reduced the risk of pancreatic infections compared to PN (RR 0.35; 95% CI 0.24–0.52; P < 0.0001; I 2 = 0%). The certainty of evidence was low. We rated down for risk of bias and imprecision (Supplement 6). Supplement 7, Fig. 8.
Question 11C: Predicted SAP. Early (<48 h) EN vs. PN
For mortality we included five RCTs (232 patients). EEN (<48 h) did not reduce the risk of death compared to PN (RR 0.61; 95% CI 0.15–2.55; P = 0.50; I 2 = 41%). The certainty of evidence was low. We rated down for imprecision (Supplement 6).
For any infections we included five RCT (232 patients), EEN (<48 h) reduced the risk of infections compared to PN (RR 0.49; 95% CI 0.28–0.83; P = 0.008, I 2 = 9%). The certainty of evidence was low. We rated down for risk of bias, inconsistency and imprecision (Supplement 6).
For pancreatic infections we included three RCTs (167 patients). EEN (<48 h) reduced the risk of pancreatic infections compared to PN (RR 0.40; 95% CI 0.22–0.73; P = 0.003; I 2 = 0%). The certainty of evidence was low. We rated down for risk of bias and imprecision (Supplement 6). Supplement 7, Fig. 9.
Taken together, the studies in different subpopulations have demonstrated a reduction of infections but no convincing effect of EEN on mortality.
Recommendation 11. We suggest using EEN in patients with severe acute pancreatitis (Grade 2C).
Question 12: Should we delay EN in patients after GI surgery?
Out of three published meta-analyses [36–38] addressing early postoperative feeding including early oral diet, the two more recent papers [36, 37] reached different conclusions: reduced mortality and length of stay (LOS) but increased risk of vomiting analysing 15 RCTs [37] vs. no difference in mortality and LOS, but reduced complications in early group from 13 RCTs [36].
We identified three RCTs comparing early vs. delayed EN after emergency GI surgery and six RCTs in elective GI surgery. Two RCTs compared EEN vs. early PN in patients after elective GI surgery (Supplement 5, Table 12).
Question 12A: Emergency GI surgery. EEN vs delayed EN
Three RCTs (343 patients) were included. EEN did not affect mortality compared to delayed EN (RR 0.80; 95% CI 0.46–1.40; P = 0.44; I 2 = 0%). EEN reduced the risk of infections compared to delayed EN (RR 0.61; 95% CI 0.40–0.93; P = 0.02; I 2 = 0%). The certainty of evidence was low. We rated down for risk of bias and imprecision (Table 3). Supplement 7, Fig. 10.
Question 12B: Elective GI surgery. EEN vs. delayed EN
For mortality three RCTs (346 patients) were included. EEN did not affect mortality compared to delayed EN in patients after elective GI surgery (RR 0.83; 95% CI 0.25–2.81; P = 0.77; I 2 = 17%). The certainty of evidence was low. We rated down for imprecision (Table 3).
For any infections six RCTs (432 patients) were included. EEN reduced the risk of infections compared to delayed EN (RR 0.43; 95% CI 0.23–0.82; P = 0.01; I 2 = 46%). The certainty of evidence was low. We rated down for risk of bias and imprecision (Table 3).
Five RCTs (404 patients) reported anastomotic leak. EEN reduced the risk of surgical leak compared to delayed EN (RR 0.43; 95% CI 0.20–0.93; P = 0.03; I 2 = 0%). The certainty of evidence was low. We rated down for imprecision (Table 3). Supplement 7, Fig. 11.
Question 12C: Elective GI surgery. EEN vs early PN
Two RCTs (440 patients) were included. EEN did not reduce the risk of pneumonia compared to early PN (RR 0.59; 95% CI 0.31–1.14; P = 0.12, I 2 = 0%), but reduced the risk of anastomotic leak compared to early PN (RR 0.42; 95% CI 0.19–0.95; P = 0.04; I 2 = 63%). The certainty of evidence was low. We rated down for risk of bias, inconsistency and imprecision (Table 3). Supplement 7, Fig. 12.
Recommendation 12. We suggest using EEN in patients after GI surgery (Grade 2C).
Question 13: Should we delay EN in patients after abdominal aortic surgery?
No RCTs but two cohort studies were identified (Supplement 5, Table 13). Cohort studies both in elective [39] and emergency repair [40] did not compare EEN with any of our comparators, but showed that EEN was successful in a minority of patients. A multimodal approach has been proposed [41], including early removal of nasogastric tubes, immediate postoperative mobilisation early oral or enteral feeding, accepting GRV up to 500 ml and use of prokinetics. Although these patients are at risk of bowel ischaemia with prevalence reported between 7 and 17% [42, 43], the risk itself should not lead to withholding EN, unless bowel ischaemia is suspected (see also Recommendation 15).
Recommendation 13. We suggest using EEN in patients after abdominal aortic surgery (Grade 2D).
Question 14: Should we delay EN in patients with abdominal trauma?
Ten RCTs and ten cohort studies addressing EEN in trauma patients (RCTs: within 6–48 h; cohort studies: within 12–96 h) were identified, but abdominal trauma specifically was addressed in six RCTs, four of them compared EEN to early PN and two EEN to delayed EN (Supplement 5, Table 14A).
Question 14A: EEN vs early PN
For mortality two RCTs (142 patients) were included. EEN did not affect mortality compared to early PN (RR 0.49; 95% CI 0.09–2.69; P = 0.41; I 2 = 0%). The certainty of evidence was very low. We rated down for risk of bias and imprecision (Table 3).
For any infection four RCTs (219 patients) were included. EEN did not affect the risk of infections compared to early PN (RR 0.59; 95% CI 0.24–1.42; P = 0.24; I 2 = 59%). The certainty of evidence was very low. We rated down for risk of bias, inconsistency and imprecision (Table 3). Supplement 7, Fig. 13.
Question 14B: EEN vs delayed EN
Two RCTs (101 patients) were included. EEN did not affect mortality compared to delayed EN (RR 0.74; 95% CI 0.18–3.11; P = 0.708). The certainty of evidence was very low. We rated down for risk of bias and imprecision (Table 3).
EEN did not affect the risk of infections compared to delayed EN (RR 0.83; 95% CI 0.41–1.70; P = 0.837). The certainty of evidence was very low. We rated down for risk of bias, inconsistency and imprecision (Table 3). See Supplement 7, Fig. 14.
Of note, earlier studies in this patient group almost exclusively used surgical jejunostomy for EN.
Existing evidence did not allow verifying or excluding any benefit or harm of EEN; therefore our recommendation is based on expert opinion. In addition to RCTs, nine observational studies were identified (Supplement 5, Table 14B).
An earlier meta-analysis in adult trauma patients in ICU (not specifically abdominal trauma) showed survival benefit in EEN commenced within 24 h after trauma [44].
Recommendation 14. We suggest using EEN in patients with abdominal trauma when the continuity of the GI tract is confirmed/restored (Grade 2D).
Question 15: Should we delay EN in patients with bowel ischaemia?
We identified no clinical studies, but physiological knowledge and common sense support withholding EN in patients with overt bowel ischaemia. However, patients with endoscopic evidence of mild to moderate large bowel mucosal ischaemia, without signs of transmural ischaemia or bowel distension, might profit from low dose EN. In this case we support considering EN. In a recent retrospective study, survivors were more often fed enterally before the diagnosis of acute mesenteric ischaemia, but no independent association between EN and mortality was demonstrated [45].
Recommendation 15. We suggest delaying EN in patients with overt bowel ischaemia (Grade 2D).
Question 16: Should we delay EN in critically ill adult patients with intestinal fistula?
We identified one retrospective cohort study and two case series, all showing outcome benefit of “early” EN (Supplement 5, Table 16). However, “early” was defined as EN started within 7 days or 14 days of admission. Retrospective design further diminishes the importance of these studies.
Intolerance of EN or increasing fistula output causing skin breakdown or fluid/electrolyte imbalance are evident reasons to decrease or discontinue EN [46].
Recommendation 16. We suggest delaying EN in patients with high-output intestinal fistula if reliable feeding access distal to the fistula is not achievable (Grade 2D).
Question 17: Should we delay EN in patients with an open abdomen?
Seven observational studies (one prospective cohort study, three retrospective cohort studies and four case series) were identified; two studies compared EEN (different definitions) vs delayed EN and reported higher rate of early abdominal closure, less fistula formation and lower incidence of ventilator-associated pneumonia in the “early” EN group (Supplement 5, Table 17). The largest study comparing EN to no EN in patients with open abdomen after abdominal trauma reported independent associations between EN and ultimate fascial closure and decreased mortality rate in patients without bowel injury, but no difference in a subgroup of patients with bowel injury [47].
Recommendation 17. We suggest using EEN in patients with open abdomen (Grade 2D).
Question 18: Should we delay EN in patients with intra-abdominal hypertension?
Four observational studies were identified (Supplement 5, Table 18), only one addressed early vs. delayed EN [48]. All studies reported high incidence of feeding intolerance associated with intra-abdominal hypertension, but data are not conclusive regarding causality. A recently published study demonstrated that EEN did not increase intra-abdominal pressure, but values exceeding 15 mmHg were associated with higher rates of feeding intolerance in patients with severe acute pancreatitis [48].
No prospective study addressing EN in patients with abdominal compartment syndrome [49] was identified. As abdominal compartment syndrome is an immediately life-threatening condition with jeopardized splanchnic perfusion, we suggest to withhold or stop EN and try to lower intra-abdominal pressure.
Recommendation 18a. We suggest using EEN in patients with intra-abdominal hypertension without abdominal compartment syndrome, but consider temporary reduction or discontinuation of EN when intra-abdominal pressure values further increase under EN (Grade 2D).
Recommendation 18b. We suggest delaying EN in patients with abdominal compartment syndrome (Grade 2D).
Question 19: Should we delay EN in patients with upper GI bleeding?
No studies addressing EEN were identified. One RCT in bleeding due to gastric or duodenal ulcer reported shorter hospital stay (4.2 ± 1.2 vs. 5.9 ± 1.4 days, P < 0.001) in the early oral feeding group [50].
EN as protection against stress ulceration and GI bleeding is suggested in one meta-analysis [51], one retrospective study in burns [52] and several reviews [53–55]. An RCT comparing ranitidine and sucralfate reported EN as an independently protective factor against GI bleeding [56]. The main rationale to prohibit eating/EN is based on fear for disturbed visibility in a further endoscopy/intervention due to rebleeding. Therefore, delaying EN for 48–72 h in patients with a high risk of rebleeding has been suggested [57]. Considering the absence of evidence to support this time frame, we suggest starting EN during the first 24–48 h after bleeding has been stopped; prolonged postponement of EN is unnecessary or even harmful because of increased risk of stress ulceration. Importantly, there is no evidence that fine-bore nasogastric tubes cause variceal bleeding [57].
Recommendation 19. We suggest delaying EN in patients with active upper GI bleeding, and starting EN when the bleeding has stopped and no signs of rebleeding are observed (Grade 2D).
Question 20: Should we delay EN in patients with acute liver failure?
We could not identify any study in acute or acute-on-chronic liver failure patients. Some benefits of EN have been shown in patients with alcoholic hepatitis, malnourished patients with cirrhosis and patients with liver transplantation [58–60], where glycogen stores may be depleted after an overnight fast and metabolic conditions resemble prolonged starvation in healthy individuals [61]. EN in fulminant acute liver failure has never been studied. These patients often present with hypoglycaemia, which should be corrected with intravenous glucose, sometimes together with insulin. Fulminant liver failure is associated with increased serum amino acid concentrations, especially glutamine [62, 63]. It seems likely that a failing liver is unable to provide effective metabolic support required for nutrition. The pathophysiological rationale to delay EN in fulminant hepatic failure would be to “spare” the severely injured liver from the duties of metabolising and storing nutrition during a period of stress and also to avoid additional increases in ammonia. Intravenous provision of nutrients except correction of hypoglycemia and appropriate provision of vitamins and trace elements may be futile or harmful early in the clinical course [64].
Recommendation 20. We suggest starting low dose EN when acute, immediately life-threatening metabolic derangements are controlled with or without liver support strategies, independent on grade of encephalopathy (Grade 2D).
Remark: Arterial ammonia levels should be monitored.
Question 21: Should we delay EN in patients with large gastric aspirate volumes (GAV)?
We identified no study addressing this question. Based on existing evidence from two RCTs comparing the threshold volumes to stop already started EN [65, 66], a clear threshold volume (in ranges up to 500 ml) that increased the risk of ventilator-associated pneumonia was not identified. Measurements of GAV/GRV are not a gold standard and alternative methods (like ultrasound) can be applied to diagnose overfilling of the stomach. Gross distension of the stomach is likely to be undesirable and therefore we suggest that EN should be delayed when GAV/GRV is >500 ml/6 h [65], either for a limited time period or until administration of prokinetics. For patients with persistently large GAV/GRVs the use of postpyloric feeding should be considered rather than withholding EN, unless bowel ischaemia or obstruction is suspected (see also Recommendation 15).
Recommendation 21. We suggest delaying EN if gastric aspirate volume is above 500 ml/6 h (Grade 2D).
Question 22: Should we delay EN in patients with absent bowel sounds?
One cohort study was identified [67] (Supplement 5, Table 22). Bowel sounds are frequently absent in mechanically ventilated patients and this is associated with impaired outcome [68]. The concept that bowel sounds must be present before initiation of enteral feeding is not based on evidence and should be abandoned [69]. After laparotomy small intestinal motility is frequently preserved despite gastric and colonic paresis. The small intestine may contract silently (absence of gas), while feeding is well tolerated [69]. Gastric and colonic paresis may effectively be treated with prokinetics [70]. Initiation of EN in absence of bowel sounds might be associated with earlier return of bowel sounds, fewer episodes of vomiting, and shorter ICU and hospital stay [67].
Recommendation 22. We suggest using EEN regardless of the presence of bowel sounds unless bowel ischaemia or obstruction is suspected (Grade 2D).
Question 23: Should we delay EN in patients with diarrhoea?
There were no studies testing delay of EN in case of diarrhoea, but diarrhoea is often considered as a reason to delay EN [71]. Prevalence of diarrhoea in unselected ICU population is between 14 and 21% [72, 73]. Causes include impaired digestion/absorption, bacterial overgrowth or infection such as Clostridium difficile. Observational studies [74, 75] suggest that diarrhoea can be effectively managed with protocolised measures other than immediate cessation in EN. We recommend analysing the causes of diarrhoea and treat appropriately (e.g. C. difficile colitis). We also suggest considering treating bacterial overgrowth by selective decontamination, fibre-enriched or semi-elementary diet or digestive enzymes to reduce diarrhoea.
Recommendation 23. We suggest using EEN in patients with diarrhoea (Grade 2D).
Conclusions
We suggest using EEN, initiated at a low rate, in the majority of critically ill patients; however, the evidence is weak. Beneficial effects in terms of infection prevention have been demonstrated in unselected critically ill patients, as well as in patients with severe acute pancreatitis and after GI surgery. However, we suggest delaying EN in patients with uncontrolled shock (haemodynamic and tissue perfusion goals are not met despite of fluids and vasopressors), uncontrolled hypoxaemia and acidosis, uncontrolled GI bleeding, overt bowel ischaemia (occlusive or non-occlusive), bowel obstruction (mechanical ileus), abdominal compartment syndrome, gastric aspirate volume >500 ml/6 h or high-output fistula if reliable distal feeding access is not achievable.
References
Kreymann KG, Berger MM, Deutz NE, Hiesmayr M, Jolliet P, Kazandjiev G, Nitenberg G, van den Berghe G, Wernerman J, DGEM (German Society for Nutritional Medicine), Ebner C, Hartl W, Heymann C, Spies C, ESPEN (European Society for Parenteral and Enteral Nutrition) (2006) ESPEN guidelines on enteral nutrition: intensive care. Clin Nutr 25:210–223. doi:10.1016/j.clnu.2006.01.021
Fernández-Ortega JF, Herrero Meseguer JI, Martínez García P, Metabolism and Nutrition Working Group of the Spanish Society of Intensive Care Medicine and Coronary units (2011) Guidelines for specialized nutritional and metabolic support in the critically-ill patient: update. Consensus SEMICYUC-SENPE: indications, timing and routes of nutrient delivery. Nutr Hosp 26(Suppl 2):7–11. doi:10.1590/S0212-16112011000800002
Taylor BE, McClave SA, Martindale RG, Warren MM, Johnson DR, Braunschweig C, McCarthy MS, Davanos E, Rice TW, Cresci GA, Gervasio JM, Sacks GS, Roberts PR, Compher C, Society of Critical Care Medicine; American Society of Parenteral and Enteral Nutrition (2016) Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). Crit Care Med 44:390–438. doi:10.1097/CCM.0000000000001525
Casaer MP, Van den Berghe G (2014) Nutrition in the acute phase of critical illness. N Engl J Med 370:1227–1236. doi:10.1056/NEJMra1304623
Weijs PJ, Looijaard WG, Beishuizen A, Girbes AR, Oudemans-van Straaten HM (2014) Early high protein intake is associated with low mortality and energy overfeeding with high mortality in non-septic mechanically ventilated critically ill patients. Crit Care 18:701. doi:10.1186/s13054-014-0701-z
National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network, Rice TW, Wheeler AP, Thompson BT, Steingrub J, Hite RD, Moss M, Morris A, Dong N, Rock P (2012) Initial trophic vs full enteral feeding in patients with acute lung injury: the EDEN randomized trial. JAMA 307:795–803. doi:10.1001/jama.2012.137
Arabi YM, Aldawood AS, Haddad SH, Al-Dorzi HM, Tamim HM, Jones G, Mehta S, McIntyre L, Solaiman O, Sakkijha MH, Sadat M, Afesh L, PermiT Trial Group (2015) Permissive underfeeding or standard enteral feeding in critically ill adults. N Engl J Med 372:2398–2408. doi:10.1056/NEJMoa1502826
Casaer MP, Van den Berghe G (2015) Editorial on the original article entitled “Permissive underfeeding of standard enteral feeding in critically ill adults” published in the New England Journal of Medicine on June 18, 2015. Ann Transl Med 3:226. doi:10.3978/j.issn.2305-5839.2015.07.22
Reintam Blaser A, Malbrain ML, Starkopf J, Fruhwald S, Jakob SM, De Waele J, Braun JP, Poeze M, Spies C (2012) Gastrointestinal function in intensive care patients: terminology, definitions and management. Recommendations of the ESICM working group on abdominal problems. Intensive Care Med 38:384–394. doi:10.1007/s00134-011-2459-y
Chuntrasakul C, Siltharm S, Chinswangwatanakul V, Pongprasobchai T, Chockvivatanavanit S, Bunnak A (1996) Early nutritional support in severe traumatic patients. J Med Assoc Thai 79:21–26
Mancl EE, Muzevich KM (2013) Tolerability and safety of enteral nutrition in critically ill patients receiving intravenous vasopressor therapy. JPEN J Parenter Enteral Nutr 37:641–651. doi:10.1177/0148607112470460
Marvin RG, McKinley BA, McQuiggan M, Cocanour CS, Moore FA (2000) Nonocclusive bowel necrosis occurring in critically ill trauma patients receiving enteral nutrition manifests no reliable clinical signs for early detection. Am J Surg 179:7–12
Wells DL (2012) Provision of enteral nutrition during vasopressor therapy for hemodynamic instability: an evidence-based review. Nutr Clin Pract 27:521–526. doi:10.1177/0884533612448480
Flordelís Lasierra JL, Pérez-Vela JL, Umezawa Makikado LD, Torres Sánchez E, Colino Gómez L, Maroto Rodríguez B, Arribas López P, Gómez de la Cámara A, Montejo González JC (2015) Early enteral nutrition in patients with hemodynamic failure following cardiac surgery. JPEN J Parenter Enteral Nutr 39:154–162. doi:10.1177/0148607113504219
Khalid I, Doshi P, DiGiovine B (2010) Early enteral nutrition and outcomes of critically ill patients treated with vasopressors and mechanical ventilation. Am J Crit Care 19:261–268. doi:10.4037/ajcc2010197
Mentec H, Dupont H, Bocchetti M, Cani P, Ponche F, Bleichner G (2001) Upper digestive intolerance during enteral nutrition in critically ill patients: frequency, risk factors, and complications. Crit Car Med 29:1955–1961
Fontaine E, Müller MJ (2011) Adaptive alterations in metabolism: practical consequences on energy requirements in the severely ill patient. Curr Opin Clin Nutr Metab Care 14:171–175. doi:10.1097/MCO.0b013e328342bad4
Needham DM, Dinglas VD, Bienvenu OJ, Colantuoni E, Wozniak AW, Rice TW, Hopkins RO, NIH NHLBI ARDS Network (2013) One year outcomes in patients with acute lung injury randomised to initial trophic or full enteral feeding: prospective follow-up of EDEN randomised trial. BMJ 346:f1532. doi:10.1136/bmj.f1532
Tamion F, Hamelin K, Duflo A, Girault C, Richard JC, Bonmarchand G (2003) Gastric emptying in mechanically ventilated critically ill patients: effect of neuromuscular blocking agent. Intensive Care Med 29:1717–1722. doi:10.1007/s00134-003-1898-5
Nguyen NQ, Chapman MJ, Fraser RJ, Bryant LK, Burgstad C, Ching K, Bellon M, Holloway RH (2008) The effects of sedation on gastric emptying and intra-gastric meal distribution in critical illness. Intensive Care Med 34:454–460. doi:10.1007/s00134-007-0942-2
Williams ML, Nolan JP (2014) Is enteral feeding tolerated during therapeutic hypothermia? Resuscitation 85:1469–1472. doi:10.1016/j.resuscitation.2014.08.018
Saur J, Leweling H, Trinkmann F, Weissmann J, Borggrefe M, Kaden JJ (2008) Modification of the Harris-Benedict equation to predict the energy requirements of critically ill patients during mild therapeutic hypothermia. In Vivo 22:143–146
Oshima T, Furukawa Y, Kobayashi M, Sato Y, Nihei A, Oda S (2015) Fulfilling caloric demands according to indirect calorimetry may be beneficial for post cardiac arrest patients under therapeutic hypothermia. Resuscitation 88:81–85. doi:10.1016/j.resuscitation.2014.12.025
Bernard SA, MacC Jones B, Buist MD (1999) Experience with prolonged induced hypothermia in severe head injury. Crit Care 3:167–172. doi:10.1186/cc371
Bernard SA, Buist M (2003) Induced hypothermia in critical care medicine: a review. Crit Care Med 31:2041–2051. doi:10.1097/01.CCM.0000069731.18472.61
van der Voort PH, Zandstra DF (2001) Enteral feeding in the critically ill: comparison between the supine and prone positions: a prospective crossover study in mechanically ventilated patients. Crit Care 5:216–220
Reignier J, Thenoz-Jost N, Fiancette M, Legendre E, Lebert C, Bontemps F, Clementi E, Martin-Lefevre L (2004) Early enteral nutrition in mechanically ventilated patients in the prone position. Crit Care Med 32:94–99. doi:10.1097/01.CCM.0000104208.23542.A8
Reignier J, Dimet J, Martin-Lefevre L, Bontemps F, Fiancette M, Clementi E, Lebert C, Renard B (2010) Before-after study of a standardized ICU protocol for early enteral feeding in patients turned in the prone position. Clin Nutr 29:210–216. doi:10.1016/j.clnu.2009.08.004
Bakiner O, Bozkirli E, Giray S, Arlier Z, Kozanoglu I, Sezgin N, Sariturk C, Ertorer E (2013) Impact of early versus late enteral nutrition on cell mediated immunity and its relationship with glucagon like peptide-1 in intensive care unit patients: a prospective study. Crit Care 17:R123. doi:10.1186/cc12795
Dennis MS, Lewis SC, Warlow C, FOOD Trial Collaboration (2005) Effect of timing and method of enteral tube feeding for dysphagic stroke patients (FOOD): a multicentre randomised controlled trial. Lancet 365:764–772. doi:10.1016/S0140-6736(05)17983-5
Lee JS, Jwa CS, Yi HJ, Chun HJ (2010) Impact of early enteral nutrition on in-hospital mortality in patients with hypertensive intracerebral hemorrhage. J Korean Neurosurg Soc 48:99–104. doi:10.3340/jkns.2010.48.2.99
Dvorak MF, Nooman VK, Belanger L, Bruun B, Wing PC, Boyd MC, Fisher C (2004) Early vs late enteral feeding in patients with acute cervical spinal cord injury: a pilot study. Spine 29:E174–E180
Rowan CJ, Gillanders LK, Paice RL, Judson JA (2004) Is early enteral feeding safe in patients who have suffered spinal cord injury? Injury 35:238–242
Petrov MS, van Santvoort HC, Besselink MG, van der Heijden GJ, Windsor JA, Gooszen HG (2008) Enteral nutrition and the risk of mortality and infectious complications in patients with severe acute pancreatitis: a meta-analysis of randomized trials. Arch Surg 143:1111–1117. doi:10.1001/archsurg.143.11.1111
Cao Y, Xu Y, Lu T, Gao F, Mo Z (2008) Meta-analysis of enteral nutrition versus total parenteral nutrition in patients with severe acute pancreatitis. Ann Nutr Metab 53:268–275. doi:10.1159/000189382
Osland E, Yunus RM, Khan S, Memon MA (2011) Early versus traditional postoperative feeding in patients undergoing resectional gastrointestinal surgery: a meta-analysis. JPEN J Parenter Enteral Nutr 35:473–487. doi:10.1177/0148607110385698
Lewis SJ, Andersen HK, Thomas S (2009) Early enteral nutrition within 24 h of intestinal surgery versus later commencement of feeding: a systematic review and meta-analysis. J Gastrointest Surg 13:569–575. doi:10.1007/s11605-008-0592-x
Lewis SJ, Egger M, Sylvester PA, Thomas S (2001) Early enteral feeding versus “nil by mouth” after gastrointestinal surgery: systematic review and meta-analysis of controlled trials. BMJ 323:773–776
Ksienski MR, Fenton TR, Eliasziw M, Zuege DJ, Petrasek P, Shahpori R, Laupland KB (2013) A cohort study of nutrition practices in the intensive care unit following abdominal aortic aneurysm repair. JPEN J Parenter Enteral Nutr 37:261–267. doi:10.1177/0148607112464654
Rahman A, Martin C, Heyland DK (2015) Nutrition therapy for the critically ill surgical patient with aortic aneurysmal rupture: defining and improving current practice. JPEN J Parenter Enteral Nutr 39:104–113. doi:10.1177/0148607113501695
van Zanten AR (2013) Nutrition barriers in abdominal aortic surgery: a multimodal approach for gastrointestinal dysfunction. JPEN J Parenter Enteral Nutr 37:172–177. doi:10.1177/0148607112464499
Vermeulen Windsant IC, Hellenthal FA, Derikx JP, Prins MH, Buurman WA, Jacobs MJ, Schurink GW (2012) Circulating intestinal fatty acid-binding protein as an early marker of intestinal necrosis after aortic surgery: a prospective observational cohort study. Ann Surg 255:796–803. doi:10.1097/SLA.0b013e31824b1e16
Rosset E, Ben Ahmed S, Galvaing G, Favre JP, Sessa C, Lermusiaux P, Hassen-Khodja R, Coggia M, Haulon S, Rinckenbach S, Enon B, Feugier P, Steinmetz E, Becquemin JP, Association Universitaire de Recherche en Chirurgie (2014) Editor’s choice–hybrid treatment of thoracic, thoracoabdominal, and abdominal aortic aneurysms: a multicenter retrospective study. Eur J Vasc Endovasc Surg 47:470–478. doi:10.1016/j.ejvs.2014.02.013
Doig GS, Heighes PT, Simpson F, Sweetman EA (2011) Early enteral nutrition reduces mortality in trauma patients requiring intensive care: a meta-analysis of randomised controlled trials. Injury 42:50–56. doi:10.1016/j.injury.2010.06.008
Leone M, Bechis C, Baumstarck K, Ouattara A, Collange O, Augustin P, Annane D, Arbelot C, Asehnoune K, Baldési O, Bourcier S, Delapierre L, Demory D, Hengy B, Ichai C, Kipnis E, Brasdefer E, Lasocki S, Legrand M, Mimoz O, Rimmelé T, Aliane J, Bertrand PM, Bruder N, Klasen F, Friou E, Lévy B, Martinez O, Peytel E, Piton A, Richter E, Toufik K, Vogler MC, Wallet F, Boufi M, Allaouchiche B, Constantin JM, Martin C, Jaber S, Lefrant JY (2015) Outcome of acute mesenteric ischemia in the intensive care unit: a retrospective, multicenter study of 780 cases. Intensive Care Med 41:667–676. doi:10.1007/s00134-015-3690-8
Polk TM, Schwab CW (2012) Metabolic and nutritional support of the enterocutaneous fistula patient: a three-phase approach. World J Surg 36:524–533. doi:10.1007/s00268-011-1315-0
Burlew CC, Moore EE, Cuschieri J, Jurkovich GJ, Codner P, Nirula R, Millar D, Cohen MJ, Kutcher ME, Haan J, MacNew HG, Ochsner G, Rowell SE, Truitt MS, Moore FO, Pieracci FM, Kaups KL, WTA Study Group (2012) Who should we feed? Western Trauma Association multi-institutional study of enteral nutrition in the open abdomen after injury. J Trauma Acute Care Surg 73:1380–1387. doi:10.1097/TA.0b013e318259924c
Sun JK, Li WQ, Ke L, Tong ZH, Ni HB, Li G, Zhang LY, Nie Y, Wang XY, Ye XH, Li N, Li JS (2013) Early enteral nutrition prevents intra-abdominal hypertension and reduces the severity of severe acute pancreatitis compared with delayed enteral nutrition: a prospective pilot study. World J Surg 37:2053–2060. doi:10.1007/s00268-013-2087-5
Kirkpatrick AW, Roberts DJ, De Waele J, Jaeschke R, Malbrain ML, De Keulenaer B, Duchesne J, Bjorck M, Leppaniemi A, Ejike JC, Sugrue M, Cheatham M, Ivatury R, Ball CG, Reintam Blaser A, Regli A, Balogh ZJ, D’Amours S, Debergh D, Kaplan M, Kimball E, Olvera C, Pediatric Guidelines Sub-Committee for the World Society of the Abdominal Compartment Syndrome (2013) Intra-abdominal hypertension and the abdominal compartment syndrome: updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med 39:1190–1206. doi:10.1007/s00134-013-2906-z
Khoshbaten M, Ghaffarifar S, Jabbar Imani A, Shahnazi T (2013) Effects of early oral feeding on relapse and symptoms of upper gastrointestinal bleeding in peptic ulcer disease. Dig Endosc 25:125–129. doi:10.1111/j.1443-1661.2012.01347.x
Marik PE, Vasu T, Hirani A, Pachinburavan M (2010) Stress ulcer prophylaxis in the new millennium: a systematic review and meta-analysis. Crit Care Med 38:2222–2228. doi:10.1097/CCM.0b013e3181f17adf
Raff T, Germann G, Hartmann B (1997) The value of early enteral nutrition in the prophylaxis of stress ulceration in the severely burned patient. Burns 23:313–318
Hurt RT, Frazier TH, McClave SA, Crittenden NE, Kulisek C, Saad M, Franklin GA (2012) Stress prophylaxis in intensive care unit patients and the role of enteral nutrition. JPEN J Parenter Enteral Nutr 36:721–731. doi:10.1177/0148607112436978
MacLaren R, Jarvis CL, Fish DN (2001) Use of enteral nutrition for stress ulcer prophylaxis. Ann Pharmacother 35:1614–1623
Pilkington KB, Wagstaff MJ, Greenwood JE (2012) Prevention of gastrointestinal bleeding due to stress ulceration: a review of current literature. Anaesth Intensive Care 40:253–259
Cook D, Heyland D, Griffith L, Cook R, Marshall J, Pagliarello J (1999) Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. Crit Care Med 27:2812–2817
Hébuterne X, Vanbiervliet G (2011) Feeding the patients with upper gastrointestinal bleeding. Curr Opin Clin Nutr Metab Care 14:197–201. doi:10.1097/MCO.0b013e3283436dc5
Cabré E, Rodríguez-Iglesias P, Caballería J, Rodríguez-Iglesias P, Caballería J, Quer JC, Sánchez-Lombraña JL, Parés A, Papo M, Planas R, Gassull MA (2000) Short and long term outcome of severe alcohol-induced hepatitis treated with steroids or enteral nutrition: a multicenter randomized trial. Hepatology 32:36–42. doi:10.1053/jhep.2000.8627
Cabré E, Gonzalez-Huix F, Abad-Lacruz A, Esteve M, Acero D, Fernandez-Bañares F, Xiol X, Gassull MA (1990) Effect of total enteral nutrition on the short-term outcome of severely malnourished cirrhotics. A randomized trial. Gastroenterology 98:715–720
Hasse JM, Blue LS, Liepa GU, Goldstein RM, Jennings LW, Mor E, Husberg BS, Levy MF, Gonwa TA, Klintmalm GB (1995) Early enteral nutrition support in patients undergoing liver transplantation. JPEN J Parenter Enteral Nutr 19:437–443
Verboeket-van de Venne WP, Westerterp KR, van Hoek B, Swart GR (1995) Energy expenditure and substrate metabolism in patients with cirrhosis of the liver: effects of the pattern of food intake. Gut 36:110–116
Helling G, Wahlin S, Smedberg M, Pettersson L, Tjäder I, Norberg Å, Rooyackers O, Wernerman J (2016) Plasma glutamine concentrations in liver failure. PLoS One 11:e0150440. doi:10.1371/journal.pone.0150440
Dejong CH, van de Poll MC, Soeters PB, Jalan R, Olde Damink SW (2007) Aromatic amino acid metabolism during liver failure. J Nutr 137(6 Suppl 1):1579S–1585S
Xu ZW, Li YS (2012) Pathogenesis and treatment of parenteral nutrition-associated liver disease. Hepatobiliary Pancreat Dis Int 11:586–593
Montejo JC, Miñambres E, Bordejé L, Mesejo A, Acosta J, Heras A, Ferré M, Fernandez-Ortega F, Vaquerizo CI, Manzanedo R (2010) Gastric residual volume during enteral nutrition in ICU patients: the REGANE study. Intensive Care Med 36:1386–1393. doi:10.1007/s00134-010-1856-y
Reignier J, Mercier E, Le Gouge A, Boulain T, Desachy A, Bellec F, Clavel M, Frat JP, Plantefeve G, Quenot JP, Lascarrou JB, Clinical Research in Intensive Care and Sepsis (CRICS) Group (2013) Effect of not monitoring residual gastric volume on risk of ventilator-associated pneumonia in adults receiving mechanical ventilation and early enteral feeding: a randomized controlled trial. JAMA 309:249–256. doi:10.1001/jama.2012.196377
Thapa PB, Nagarkoti K, Lama T, Maharjan DK, Tuladhar M (2011) Early enteral feeding in intestinal anastomosis. J Nepal Health Res Counc 9:1–5
Reintam A, Parm P, Kitus R, Kern H, Starkopf J (2009) Gastrointestinal symptoms in intensive care patients. Acta Anaesthesiol Scand 53:318–324. doi:10.1111/j.1399-6576.2008.01860.x
Heyland D, Cook DJ, Winder B, Brylowski L, Van deMark H, Guyatt G (1995) Enteral nutrition in the critically ill patient: a prospective survey. Crit Care Med 23:1055–1060
Frost P, Edwards N, Bihari D (1997) Gastric emptying in the critically ill—the way forward? Intensive Care Med 23:243–245
Marshall AP, West SH (2006) Enteral feeding in the critically ill: are nursing practices contributing to hypocaloric feeding? Intensive Crit Care Nurs 22:95–105. doi:10.1016/j.iccn.2005.09.004
Thibault R, Graf S, Clerc A, Delieuvin N, Heidegger CP, Pichard C (2013) Diarrhoea in the ICU: respective contribution of feeding and antibiotics. Crit Care 17:R153. doi:10.1186/cc12832
Reintam Blaser A, Deane AM, Fruhwald S (2015) Diarrhoea in the critically ill. Curr Opin Crit Care 21:142–153. doi:10.1097/MCC.0000000000000188
Ferrie S, East V (2007) Managing diarrhoea in intensive care. Aust Crit Care 20:7–13
Montejo JC (1999) Enteral nutrition-related gastrointestinal complications in critically ill patients: a multicenter study. The Nutritional and Metabolic Working Group of the Spanish Society of Intensive Care Medicine and Coronary Units. Crit Care Med 27:1447–1453
Acknowledgements
Collaborators in ESICM Working Group on Gastrointestinal Function: Claudia Spies, Klinik für Anästhesiologie mit Schwerpunkt operative Intensivmedizin der Charité-Universitätsmedizin Berlin, Campus Virchow Klinikum, Berlin; Pietro Vecchiarelli, Intensive Care Unit, Ospedale Belcolle, Strada Sammartinese, Belcolle Hospital, Viterbo, Italy; Anne Berit Guttormsen, Department of Anesthesia and Intensive Care, Haukeland University Hospital, Bergen, Norway. The costs covering the open access publication of this article were covered by the International Fluid Academy (IFA). The IFA is integrated within the not-for-profit charitable organization iMERiT (International Medical Education and Research Initiative) under Belgian Law, and IFA website (http://www.fluidacademy.org) is an official SMACC (Social Media and Critical Care) affiliated site, based on the philosophy of FOAM (Free Open Access Medical Education).
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflicts of interest
See Supplement 8.
Additional information
Take-home message: The administration of early EN appears to reduce infections and should be used for the majority of critically ill patients. However, there are certain situations when we recommend EN be delayed.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Reintam Blaser, A., Starkopf, J., Alhazzani, W. et al. Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines. Intensive Care Med 43, 380–398 (2017). https://doi.org/10.1007/s00134-016-4665-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-016-4665-0