
Abstract
Aims/hypothesis
Glycaemic markers and fasting insulin are frequently measured outcomes of intervention studies. To extrapolate accurately the impact of interventions on the risk of diabetes incidence, we investigated the size and shape of the associations of fasting plasma glucose (FPG), 2 h post-load glucose (2hPG), HbA1c, fasting insulin and HOMA-IR with incident type 2 diabetes mellitus.
Methods
The study population included 1349 participants aged 50–75 years without diabetes at baseline (1989) from a population-based cohort in Hoorn, the Netherlands. Incident type 2 diabetes was defined by the WHO 2011 criteria or known diabetes at follow-up. Logistic regression models were used to determine the associations of the glycaemic markers, fasting insulin and HOMA-IR with incident type 2 diabetes. Restricted cubic spline logistic regressions were conducted to investigate the shape of the associations.
Results
After a mean follow-up duration of 6.4 (SD 0.5) years, 152 participants developed diabetes (11.3%); the majority were screen detected by high FPG. In multivariate adjusted models, ORs (95% CI) for incident type 2 diabetes for the highest quintile in comparison with the lowest quintile were 9.0 (4.4, 18.5) for FPG, 6.1 (2.9, 12.7) for 2hPG, 3.8 (2.0, 7.2) for HbA1c, 1.9 (0.9, 3.6) for fasting insulin and 2.8 (1.4, 5.6) for HOMA-IR. The associations of FPG and HbA1c with incident diabetes were non-linear, rising more steeply at higher values.
Conclusions/interpretation
FPG was most strongly associated with incident diabetes, followed by 2hPG, HbA1c, HOMA-IR and fasting insulin. The strong association with FPG is probably because FPG is the most frequent marker for diabetes diagnosis. Non-linearity of associations between glycaemic markers and incident type 2 diabetes should be taken into account when estimating future risk of type 2 diabetes based on glycaemic markers.
Similar content being viewed by others
Introduction
Increased levels of glucose and insulin, in the fasting and postprandial state, and HbA1c are key characteristics of type 2 diabetes mellitus. Increments in these risk factors, years before disease onset, precede the development of diabetes [1, 2]. Increases in post-load glucose have been shown to become apparent before increases in fasting glucose [2]. When people reach the impaired glucose tolerance (IGT) state, the transition from IGT to type 2 diabetes within populations occurs at a remarkably high rate: an estimated 25% of people with IGT develop type 2 diabetes within 3–5 years and 40–50% within 10 years [3].
Intervention studies for drugs, lifestyle or diet often use glycaemic markers as their primary outcome measures. To extrapolate the impact of such interventions on diabetes incidence and to estimate their public health impact, accurate quantification of the association between glycaemic markers and incident type 2 diabetes is needed. Knowledge of these associations may subsequently be used to build health impact models that estimate the effect of different interventions on diabetes incidence.
Despite this, only a limited number of studies have reported on the independent continuous associations of fasting plasma glucose (FPG), 2 h post-load glucose (2hPG), HbA1c and fasting insulin with incident type 2 diabetes mellitus. Some studies have investigated the association between impaired fasting glucose (IFG) or IGT status vs normoglycaemia on diabetes incidence [3,4,5,6], rather than reporting risks for the entire glucose distribution. Other studies have investigated the continuous association of glycaemic markers with risk of diabetes mostly assuming a linear association [3, 7,8,9,10]. To our knowledge, a non-linear shape of the association between glycaemic markers and incident type 2 diabetes has only been previously described for FPG and HbA1c, with both showing a curvilinear relationship [11]. The shapes of the associations of 2hPG, fasting insulin and HOMA-IR, a measure of insulin resistance [12], with incident type 2 diabetes have not been extensively studied.
The aim of this study was to assess the size and shape of the associations of FPG, 2hPG, HbA1c, fasting insulin, and HOMA-IR with incident type 2 diabetes.
Methods
Study population
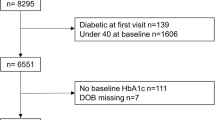
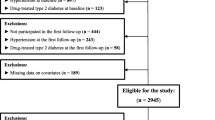
The Hoorn Study is a population-based prospective cohort study on glucose metabolism performed in the city of Hoorn, the Netherlands. Details of the study have been described previously [13]. In brief, a random sample of 3553 residents from the municipal registry of Hoorn, aged 50–75 years, was invited to participate in the study. In total, 2484 participants were included in the baseline examination from October 1989 to February 1992. Of the original cohort, 150 had died, 108 had moved out of Hoorn and 140 could not be invited for logistical reasons. Of the remaining 2086 individuals who were invited to participate in the follow-up examination from January 1996 to December 1998, 1513 (72.5%) participated [3]. In the present study, we excluded 20 participants with missing data on glycaemic markers at follow-up. We further excluded 144 participants with diabetes at baseline; of whom 41 had known diabetes and 103 were detected at screening (FPG ≥ 7.0 mmol/l or 2hPG ≥ 11.1 mmol/l or HbA1c ≥ 6.5% [48 mmol/mol]). Therefore, 1349 participants were included in the present analyses. The study was approved by the Ethics Committee of the VU University Medical Center and written informed consent was obtained from all participants.
Baseline measures
Weight (kg) and height (cm) were determined according to standardised procedures in participants wearing light clothes without shoes [14]. BMI was calculated as weight in kilograms divided by height in metres squared (kg/m2). Waist circumference (cm) was measured in standing position midway between the lower rib margin and the iliac crest. Systolic blood pressure (mmHg) was measured twice on the right arm with a random-zero sphygmomanometer (Hawksley-Gelman, Lancing, Sussex, UK) while participants were sitting after 5 min of rest, and the mean of the two readings was used for analysis. Information on family history of diabetes, physical activity and smoking were self-reported. Information about alcohol consumption was obtained by a validated semi-quantitative food frequency questionnaire, in which participants were questioned about how many glasses of several alcohol beverages they usually consume per week [15].
For the measurement of FPG levels a venous blood glucose sample was collected after an overnight fast. Subsequently, a standard 75 g OGTT was performed and a blood sample was drawn 2 h after ingestion to measure the 2hPG level. FPG and 2hPG levels were determined by the glucose dehydrogenase method (Merck, Darmstadt, Germany; interassay CV of 1.4%). HbA1c levels were determined in fasting whole blood by ion exchange HPLC (Bio-Rad Diamat, Veenendaal, the Netherlands; interassay CV of 0.6–3.1%). Fasting specific serum insulin levels were quantified by an insulin-specific double-antibody radioimmunoassay (antibody SP21; Linco Research, St Louis, MO, USA; interassay CV of 6% at insulin levels in the range of 40–1000 pmol/l). HOMA-IR was calculated as [fasting glucose (mmol/l) x fasting insulin (pmol/l)]/135 [16]. Participants with elevated levels of glycaemic markers at baseline were advised to take their screening results to their general practitioner.
Triacylglycerol was measured in fasting blood samples by enzymatic techniques (Boehringer-Mannheim, Mannheim, Germany). LDL-cholesterol levels were calculated with the Friedewald formula [17] only for participants with a triacylglycerol level ≤ 4.5 mmol/l because the formula is not reliable above this level.
Outcome measure: incident type 2 diabetes
At the follow-up examination from January 1996 to December 1998, measures of FPG, 2hPG and HbA1c were determined with the same procedures and assays as previously described for the baseline examination. Incident type 2 diabetes was defined as newly diagnosed diabetes at follow-up. In line with the WHO 2011 diagnostic criteria [18], participants were diagnosed with type 2 diabetes when they met at least one of the following criteria: FPG ≥ 7.0 mmol/l or 2hPG ≥ 11.1 mmol/l or HbA1c ≥ 6.5% (48 mmol/mol) or known diabetes at follow-up (i.e. defined by self-reported current treatment with insulin or hypoglycaemic agents). Medical records were checked in case of doubt to verify diabetes status.
Statistical analysis
Baseline characteristics of the study participants are summarised by baseline quintiles of FPG. Data are presented as mean (SD) for normally distributed continuous variables or median (25th–75th percentile) for positively skewed distributions. Categorical variables are presented as percentages. Independent variables with positively skewed distributions were transformed taking the natural logarithm (log e ) prior to further analysis. The follow-up duration was calculated as the time between the baseline and follow-up examinations. In order to investigate possible collinearity between independent baseline variables, the correlations between FPG, 2hPG, HbA1c, fasting insulin and HOMA-IR were determined using Spearman correlation coefficients.
Multiple imputation techniques were performed to handle missing data in baseline independent variables. As the percentage of missing values was < 5% for all variables, except for physical activity (9%), five imputed datasets were created and the results of the analyses from the different imputed datasets were pooled using Rubin’s rules [19]. The Multivariate Imputation by Chained Equations (MICE) algorithm was used with the predictive mean matching method.
Logistic regression models were used to estimate the ORs for incident diabetes per SD, and per quintile (Q) of FPG, 2hPG, HbA1c, fasting insulin and HOMA-IR relative to the lowest quintile. Model 1 was adjusted for age, sex and follow-up duration because participants with elevated glucose levels had shorter follow-up durations. In model 2, additional adjustment was made for potentially confounding factors which were determined a priori. Such a model quantifies, for example, the association of incident diabetes per SD increase in FPG, given that all the other variables in the model stay the same. BMI, waist circumference, systolic blood pressure, triacylglycerol and LDL-cholesterol were all modelled as continuous variables. Smoking status (non-smokers vs smokers), alcohol consumption (0 g/day [reference category], < 10 g/day, 10–30 g/day, ≥ 30 g/day), physical activity (< or ≥ 30 min physical activity per day in summer) and family history of diabetes (parent only with diabetes, sibling only with diabetes or parent and sibling with diabetes) were all modelled as categorical variables. In model 3, the independent variables were mutually adjusted for each other, together with the previously mentioned covariates, in order to examine whether the associations of FPG, 2hPG, HbA1c, fasting insulin and HOMA-IR with incident type 2 diabetes were independent of each other. A two-sided p value < 0.05 was considered to indicate statistical significance.
Effect-modification was investigated by including interaction terms between baseline blood glucose measures and age (as a continuous variable) and sex, respectively, in the logistic regression models, and calculating their corresponding p values. For interaction terms, a p value < 0.10 was considered statistically significant.
To investigate the shapes of the associations, logistic regression models including restricted cubic spline (RCS) functions with three knots (percentile 10, 50, 90) were conducted for each independent variable separately [20]. These models were adjusted for age, sex and follow-up duration. The -2 log likelihoods of the logistic regression models with and without RCS functions were compared in the likelihood ratio test (following a χ2 distribution with one degree of freedom) to evaluate which model fitted the data best.
In addition, to facilitate comparison of the results of the logistic regression models with RCS functions to the logistic regression models with quintiles of the markers, and to visualise the results, the following was performed. ORs were derived from RCS logistic regression models by calculating the odds at each value of the markers and dividing this by the odds of a reference category. The reference category for calculating the ORs was chosen as the mean value of the first quintile of each marker.
Probabilities for developing type 2 diabetes were computed from the logistic regression models with RCS functions and plotted for each of the markers.
Data analyses were performed using IBM SPSS Statistics version 21 for Windows (SPSS, Chicago, IL, USA) and R version 3.2.3 (www.R-project.org), using the packages rms (https://cran.r-project.org/web/packages/rms/index.html) and ggplot2 (https://cran.r-project.org/web/packages/ggplot2/index.html).
Results
The mean baseline age of the total study population was 60.3 (6.9) years and 54.6% were male. Relative to participants in the lowest quintile of FPG, those in the highest quintile had higher mean BMI, waist circumference, systolic blood pressure, 2hPG, HbA1c, fasting insulin and HOMA-IR (Table 1). Participants in the follow-up examination were on average younger (60.6 years vs 63.2 years), had lower mean baseline FPG levels (5.6 mmol/l vs 5.9 mmol/l), lower 2hPG levels (5.9 mmol/l vs 6.2 mmol/l) and lower HbA1c levels (5.4% [36 mmol/mol] vs 5.6% [38 mmol/mol]) compared with non-participants (n = 971).
After a mean follow-up duration of 6.4 (0.5) years, 152 participants developed type 2 diabetes (11.3%). The majority of incident cases had isolated FPG ≥ 7.0 mmol/l (61 participants), followed by isolated 2hPG ≥ 11.1 mmol/l (21 participants) and isolated HbA1c ≥ 6.5% [48 mmol/mol] (21 participants). The remainder had a combination of two criteria (33 participants), while 13 participants had type 2 diabetes based on all three criteria. Three patients with incident diabetes were receiving glucose-lowering medication and had normal glucose and HbA1c levels.
The Spearman correlation coefficients among FPG, 2hPG, HbA1c and fasting insulin ranged between 0.04 and 0.31. As a consequence of high correlations between HOMA-IR and its components (HOMA-IR and FPG: r = 0.50; HOMA-IR and fasting insulin: r = 0.97), the mutually adjusted model of HOMA-IR was only adjusted for 2hPG and HbA1c in order to avoid possible problems with collinearity.
The associations of FPG, 2hPG, HbA1c, fasting insulin and HOMA-IR with type 2 diabetes risk are shown in Table 2. No interactions were observed between baseline glycaemic markers and age or sex (p value interaction terms > 0.10). In all models, FPG was most strongly associated with incident diabetes, followed by 2hPG, HbA1c, HOMA-IR and fasting insulin. After multivariate adjustment (model 2), all markers, except fasting insulin, were significantly associated with diabetes incidence. Mutual adjustment for other markers (model 3), slightly attenuated the associations.
Figure 1 shows the shape of the associations of the glycaemic markers, fasting insulin and HOMA-IR with diabetes incidence. Comparison of the -2 log likelihoods of the logistic regression models with and without RCS functions revealed a statistically significant improvement in model fit for the non-linear RCS models for the glycaemic markers FPG and HbA1c (likelihood ratio tests p < 0.001). In contrast, for 2hPG, log e fasting insulin and log e HOMA-IR (likelihood ratio tests p = 0.79, p = 0.56 and p = 0.28, respectively), the model fit did not significantly improve when including the non-linear RCS functions into the models. Therefore, the shape of the association of FPG and HbA1c with incident type 2 diabetes is non-linear, while the shape of 2hPG, log e fasting insulin and log e HOMA-IR with incident type 2 diabetes is linear.

Curves of ORs (95% CI) derived from logistic regression models including restricted cubic splines to evaluate the associations of incident type 2 diabetes with (a) FPG (b) 2hPG (c) HbA1c (d) log e fasting insulin and (e) log e HOMA-IR. The dots (95% CI) are the ORs after each risk factor is converted into quintiles with the first dot indicating the lowest quintile, which is used as reference category. Adjustment was made for age, sex, and follow-up duration. The vertical dotted lines indicate the knot locations (percentile 10, 50, 90)
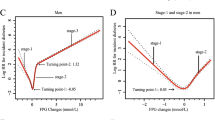
As shown in Fig. 2, the estimated probability of developing diabetes sharply increases when FPG exceeds 5.6 mmol/l and when HbA1c exceeds 5.5% (37 mmol/mol). For 2hPG, insulin and HOMA-IR, the increment in probability to develop diabetes is more gradual over the whole range of their corresponding distributions.

Absolute risks for type 2 diabetes within 6.4 years follow-up for baseline (a) FPG (b) 2hPG (c) HbA1c (d) log e fasting insulin and (e) log e HOMA-IR
Discussion
In this cohort study of a 50–75-year-old Dutch population, FPG was most strongly associated with incident type 2 diabetes followed by 2hPG, HbA1c, HOMA-IR and fasting insulin. In multivariate adjusted models, fasting insulin was no longer associated with incident type 2 diabetes. The key finding of this study was non-linearity of the associations of FPG and HbA1c with incident type 2 diabetes, in contrast to 2hPG, log e fasting insulin and log e HOMA-IR, which were all linearly associated with incident type 2 diabetes.
A limited number of other prospective cohort studies have reported associations for incident type 2 diabetes of all three glycaemic markers, i.e. FPG, 2hPG and HbA1c. In the Australian Diabetes, Obesity and Lifestyle Study (AusDiab), a population-based study in which 6537 individuals were followed for over 5 years, FPG (per SD) was the strongest predictor for incident type 2 diabetes, followed by HbA1c and 2hPG, after multivariate adjustment [8]. However, in the KORA S4/F4 cohort study, the association with incident type 2 diabetes was stronger for 2hPG (per SD) than for FPG and HbA1c in multivariate adjusted models [9]. Inconsistencies in results between studies may be explained by the use of different definitions of diabetes. In the AusDiab and KORA studies, type 2 diabetes was defined by FPG and 2hPG criteria, while in our study HbA1c was also included as a diagnostic criterion for incident type 2 diabetes. In addition, the number of people diagnosed with diabetes based on elevated FPG and/or 2hPG levels may differ between cohorts. In our study, the strong association between FPG and incident type 2 diabetes is potentially explained by the high number of individuals who were diagnosed based on FPG. The numbers of participants identified by the individual criteria were not reported for the AusDiab and KORA study.
Another potential explanation for differences in the strengths of associations is diversity in the intra-individual variation between markers. Previous studies have indicated lowest intra-individual variation for FPG and higher intra-individual variations for 2hPG, HbA1c and fasting insulin [21,22,23]. The higher intra-individual variability of fasting insulin, but also of HbA1c, compared with glucose may partly explain the weaker associations with type 2 diabetes [24].
Information on the associations between fasting insulin and HOMA-IR with incident type 2 diabetes is scarce. In the Prospective Study of Pravastatin in the Elderly at Risk (PROSPER) study, HOMA-IR was more strongly associated with incident type 2 diabetes than fasting insulin [25], which corresponds to the observations in our study. Moreover, in the PROSPER study and the San Antonio Heart Study, fasting insulin was significantly associated with the risk of developing type 2 diabetes after adjustment for confounders, while in our study the association between fasting insulin and incident type 2 diabetes was no longer statistically significant after adjusting for metabolic and lifestyle risk factors [25, 26].
In the present study, non-linearity of the associations of FPG and HbA1c with incident type 2 diabetes was indicated by a better model fit of logistic regression models including the RCS functions for these associations. A previous publication showed curvilinear associations for FPG and HbA1c with incident type 2 diabetes [11], which corresponds to the shape of these associations established in our study. Furthermore, the shape of the associations of FPG and HbA1c with incident type 2 diabetes in the present study suggests that the risk plateaus for FPG levels < 5.6 mmol/l and HbA1c levels < 5.5% [37 mmol/mol]. In contrast, the linear associations of 2hPG, log e fasting insulin and log e HOMA-IR with incident type 2 diabetes suggest that the risk is lowered with lower levels. Contrary to the diagnostic criteria for type 2 diabetes, for which the thresholds are based on associations with complications, thresholds for IFG, IGT and the prediabetes HbA1c are based on associations of the glycaemic markers with incident type 2 diabetes. The presently observed increase in risk from FPG levels about 5.6 mmol/l is closer to the threshold for IFG from the ADA (5.6 mmol/l) [27] than from the WHO (6.1 mmol/l) [18].
Our study thus shows that non-linearity of associations should be taken into account when extrapolating data on risk factors to population risks of type 2 diabetes incidence. For example, in the current study, when a linear association between FPG and incident type 2 diabetes was assumed, a more than twofold increased risk of diabetes for each 0.5 mmol/l increase in FPG was estimated. The current study suggests that at levels < 5.6 mmol/l FPG is not related to diabetes risk, whereas in the higher levels of FPG (> 5.6 mmol/l) the risk is increased two to sixfold. These data are highly relevant for policymakers and public health bodies in future predictions of type 2 diabetes incidence. In addition, this information is relevant when estimating the public health implications of intervention studies targeting glycaemic measures.
The strengths of this study include the use of the 2011 WHO diagnostic criteria, the use of OGTT as well as HbA1c as diagnostic tests for type 2 diabetes mellitus, and the ability to compare the strengths of the associations of incident diabetes with all three glycaemic measures as well as insulin. Our study also has some limitations. First, this study includes a relatively small sample size, which limits the power of the study. Second, screening included only one single blood sample, while in clinical practice two measurements are needed for diabetes diagnosis [28]. Third, the strengths of the associations found in our study were specific to a population aged 50–75 years, which limits the generalisability to broader age ranges. Fourth, participants at the follow-up examination were on average healthier compared with non-participants. Therefore, potential selection bias may have occurred and thus the study population may not be completely representative of the general population. Finally, the fixed follow-up duration of 6 years does not allow the modelling of risks over time.
In conclusion, FPG was most strongly associated with incident diabetes, followed by 2hPG, HbA1c, HOMA-IR and fasting insulin. The strong association of FPG compared with 2hPG and HbA1c is in line with FPG being the most common marker for the diagnosis of type 2 diabetes. These results have potential implications for accurately estimating the risk of type 2 diabetes on the basis of glycaemic measures and translating the effects observed in intervention studies into type 2 diabetes risk.
Abbreviations
- 2hPG:
-
2 h post-load glucose
- AusDiab:
-
Australian Diabetes, Obesity and Lifestyle Study
- FPG:
-
Fasting plasma glucose
- IFG:
-
Impaired fasting glucose
- IGT:
-
Impaired glucose tolerance
- PROSPER:
-
Prospective Study of Pravastatin in the Elderly at Risk
- Q:
-
Quintile
- RCS:
-
Restricted cubic spline
References
Heianza Y, Arase Y, Fujihara K et al (2012) Longitudinal trajectories of HbA1c and fasting plasma glucose levels during the development of type 2 diabetes: the Toranomon Hospital Health Management Center Study 7 (TOPICS 7). Diabetes Care 35:1050–1052
Tabak AG, Jokela M, Akbaraly TN, Brunner EJ, Kivimaki M, Witte DR (2009) Trajectories of glycaemia, insulin sensitivity, and insulin secretion before diagnosis of type 2 diabetes: an analysis from the Whitehall II study. Lancet 373:2215–2221
de Vegt F, Dekker JM, Jager A et al (2001) Relation of impaired fasting and postload glucose with incident type 2 diabetes in a Dutch population: the Hoorn Study. JAMA 285:2109–2113
Li CL, Tsai ST, Chou P (2003) Relative role of insulin resistance and beta-cell dysfunction in the progression to type 2 diabetes – the Kinmen Study. Diabetes Res Clin Pract 59:225–232
Harati H, Hadaegh F, Saadat N, Azizi F (2009) Population-based incidence of type 2 diabetes and its associated risk factors: results from a six-year cohort study in Iran. BMC Public Health 9:186
Wang JJ, Yuan SY, Zhu LX et al (2004) Effects of impaired fasting glucose and impaired glucose tolerance on predicting incident type 2 diabetes in a Chinese population with high post-prandial glucose. Diabetes Res Clin Pract 66:183–191
Forouhi NG, Luan J, Hennings S, Wareham NJ (2007) Incidence of type 2 diabetes in England and its association with baseline impaired fasting glucose: the Ely study 1990–2000. Diabet Med 24:200–207
Magliano DJ, Barr EL, Zimmet PZ et al (2008) Glucose indices, health behaviors, and incidence of diabetes in Australia: the Australian Diabetes, Obesity and Lifestyle Study. Diabetes Care 31:267–272
Rathmann W, Strassburger K, Heier M et al (2009) Incidence of type 2 diabetes in the elderly German population and the effect of clinical and lifestyle risk factors: KORA S4/F4 cohort study. Diabet Med 26:1212–1219
Chamnan P, Simmons RK, Forouhi NG et al (2011) Incidence of type 2 diabetes using proposed HbA1c diagnostic criteria in the European prospective investigation of cancer-Norfolk cohort: implications for preventive strategies. Diabetes Care 34:950–956
Soulimane S, Simon D, Shaw JE et al (2011) Comparing incident diabetes as defined by fasting plasma glucose or by HbA1c. The AusDiab, Inter99 and DESIR studies. Diabet Med 28:1311–1318
Wallace TM, Levy JC, Matthews DR (2004) Use and abuse of HOMA modeling. Diabetes Care 27:1487–1495
Mooy JM, Grootenhuis PA, de Vries H et al (1995) Prevalence and determinants of glucose intolerance in a Dutch Caucasian population. The Hoorn Study. Diabetes Care 18:1270–1273
Beks PJ, Mackaay AJ, de Neeling JN, de Vries H, Bouter LM, Heine RJ (1995) Peripheral arterial disease in relation to glycaemic level in an elderly Caucasian population: the Hoorn study. Diabetologia 38:86–96
Grootenhuis PA, Westenbrink S, Sie CM, de Neeling JN, Kok FJ, Bouter LM (1995) A semiquantitative food frequency questionnaire for use in epidemiologic research among the elderly: validation by comparison with dietary history. J Clin Epidemiol 48:859–868
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC (1985) Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28:412–419
Friedewald WT, Levy RI, Fredrickson DS (1972) Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 18:499–502
World Health Organization (2011) In: WHO/NMH/CHP/CPM/11.1 (ed) Use of glycated haemoglobin (HbA1c) in the diagnosis of diabetes mellitus. World Health Organization, Geneva
Rubin DB (1987) Multiple imputation for nonresponse in surveys. Wiley, New York
Desquilbet L, Mariotti F (2010) Dose-response analyses using restricted cubic spline functions in public health research. Stat Med 29:1037–1057
Mooy JM, Grootenhuis PA, de Vries H et al (1996) Intra-individual variation of glucose, specific insulin and proinsulin concentrations measured by two oral glucose tolerance tests in a general Caucasian population: the Hoorn Study. Diabetologia 39:298–305
Utzschneider KM, Prigeon RL, Tong J et al (2007) Within-subject variability of measures of beta cell function derived from a 2 h OGTT: implications for research studies. Diabetologia 50:2516–2525
Simon D, Senan C, Balkau B, Saint-Paul M, Thibult N, Eschwege E (1999) Reproducibility of HbA1c in a healthy adult population: the Telecom Study. Diabetes Care 22:1361–1363
Rosner B, Spiegelman D, Willett WC (1992) Correction of logistic regression relative risk estimates and confidence intervals for random within-person measurement error. Am J Epidemiol 136:1400–1413
Welsh P, Preiss D, Lloyd SM et al (2014) Contrasting associations of insulin resistance with diabetes, cardiovascular disease and all-cause mortality in the elderly: PROSPER long-term follow-up. Diabetologia 57:2513–2520
Haffner SM, Stern MP, Mitchell BD, Hazuda HP, Patterson JK (1990) Incidence of type II diabetes in Mexican Americans predicted by fasting insulin and glucose levels, obesity, and body-fat distribution. Diabetes 39:283–288
Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (1997) Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 20:1183–1197
International Expert Committee (2009) International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 32:1327–1334
Acknowledgements
The authors express their gratitude to the participants of the Hoorn Study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Data availability
The datasets analysed during the current study are available from the corresponding author on reasonable request.
Funding
The present study was financially supported by a grant from Unilever R&D Vlaardingen, the Netherlands, and from the EMGO Institute for Health and Care Research Amsterdam, the Netherlands.
Duality of interest
MA, DJM and PLZ are employees of Unilever R&D Vlaardingen, the Netherlands. The other authors declare that there is no duality of interest associated with this manuscript.
Contribution statement
CR researched the data and wrote the manuscript. CR, MA, IAB, VMHC, JMD, JWB, MRO, PLZ and DJM contributed to conception and design of the study. JMD contributed to the acquisition of the data. VMHC, MH and FPCS helped with the statistical analysis. CR, MA, IAB, VMHC, JMD, MH, JWB, FPCS, MRO, PLZ and DJM interpreted the data. CR, MA, IAB, VMHC, JMD, MH, JWB, FPCS, MRO, PLZ and DJM critically revised and edited the manuscript for important intellectual content. All authors approved the final version of the manuscript to be published. CR is the guarantor of this work.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Ruijgrok, C., Dekker, J.M., Beulens, J.W. et al. Size and shape of the associations of glucose, HbA1c, insulin and HOMA-IR with incident type 2 diabetes: the Hoorn Study. Diabetologia 61, 93–100 (2018). https://doi.org/10.1007/s00125-017-4452-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-017-4452-7