
Abstract
Aims/hypothesis
Enteroviral infection has been implicated in the development of islet autoimmunity in type 1 diabetes and enteroviral antigen expression has been detected by immunohistochemistry in the pancreatic beta cells of patients with recent-onset type 1 diabetes. However, the immunohistochemical evidence relies heavily on the use of a monoclonal antibody, clone 5D8/1, raised against an enteroviral capsid protein, VP1. Recent data suggest that the clone 5D8/1 may also recognise non-viral antigens; in particular, a component of the mitochondrial ATP synthase (ATP5B) and an isoform of creatine kinase (CKB). Therefore, we evaluated the fidelity of immunolabelling by clone 5D8/1 in the islets of patients with type 1 diabetes.
Methods
Enteroviral VP1, CKB and ATP5B expression were analysed by western blotting, RT-PCR and immunocytochemistry in a range of cultured cell lines, isolated human islets and human tissue.
Results
Clone 5D8/1 labelled CKB, but not ATP5B, on western blots performed under denaturing conditions. In cultured human cell lines, isolated human islets and pancreas sections from patients with type 1 diabetes, the immunolabelling of ATP5B, CKB and VP1 by 5D8/1 was readily distinguishable. Moreover, in a human tissue microarray displaying more than 80 different cells and tissues, only two (stomach and colon; both of which are potential sites of enterovirus infection) were immunopositive when stained with clone 5D8/1.
Conclusions/interpretation
When used under carefully optimised conditions, the immunolabelling pattern detected in sections of human pancreas with clone 5D8/1 did not reflect cross-reactivity with either ATP5B or CKB. Rather, 5D8/1 is likely to be representative of enteroviral antigen expression.
Similar content being viewed by others

Introduction
Considerable evidence has accumulated to support the possibility that type 1 diabetes may have a viral aetiology, at least in some individuals. A number of viruses have been implicated, but the majority view suggests that one or more enteroviruses are the most likely candidates [1, 2]. However, this evidence remains largely circumstantial and relies on a body of epidemiological data supported by immunohistochemical studies conducted with pathological specimens recovered from patients diagnosed with type 1 diabetes [1, 3–5]. These have revealed that a minority of islet cells of individuals with recent-onset disease (and some with longer-duration illness) display evidence of enteroviral antigen expression [3–5]. In a small number of cases, the immunocytochemical evidence has been supported by more direct evidence of the presence of virus, via the detection of positive in situ hybridisation signals indicative of the presence of viral RNA [6]. On two occasions, a potentially diabetogenic strain of Coxsackievirus (CV)B4 has been isolated directly from the pancreases of patients with diabetes [3, 7]. Group B Coxsackieviruses have also been linked to type 1 diabetes in epidemiological studies [8, 9], and they can cause pancreatitis and diabetes in mice [10]. Collectively, these studies imply that, in a proportion of recently diagnosed patients with type 1 diabetes, the development of a persistent enterovirus infection (especially with CVB4) might underlie the changes that lead to autoimmunity and ultimately to the loss of pancreatic beta cells.
One important caveat is that the majority of studies in which viral antigen expression has been detected in the islets of patients with type 1 diabetes have employed a commercial monoclonal antiserum, clone 5D8/1 [3–5]. This antibody is directed against a peptide sequence (EIPALTAVE [11–13]) encoded within one of the viral capsid proteins, VP1, which is expressed by a range of enteroviral species. The antibody has been validated extensively and is widely recognised to bind to VP1 with high avidity. This antibody has been used in several studies to detect enteroviral VP1 in various human and mouse tissues, including thyroid, myocardium and pancreas [3–5, 13–17]. However, it is accepted that few antibodies display absolute specificity under all conditions and it is well known that 5D8/1 can bind to additional proteins under some circumstances, especially when it is used at high concentrations or after incomplete optimisation within the target tissue [18]. Recently, this issue has been brought to the fore by studies implying that 5D8/1 can bind to two specific proteins, a component of the mitochondrial ATPase complex, ATP5B, and an isoform of creatine kinase, CKB, on western blots of human islet extracts [19]. This led the authors to propose that previous work in which 5D8/1 was used to define viral antigen expression in pancreas sections by immunohistochemistry should be re-evaluated, since the conclusion that immunopositivity is indicative of the presence of virus protein might be unsafe.
In the present study we have undertaken this re-evaluation and show that, under carefully optimised conditions, 5D8/1 does not label either ATP5B or CKB in fixed tissue samples studied by immunocytochemical methods. As such, this work lends further support to earlier conclusions that the detection of VP1 in the islet cells of patients with type 1 diabetes is indicative of the presence of an enteroviral infection.
Methods
Viruses
CVB4 (VD2921), CVB1 (CVB1-10802 CDC strain), CVB3 (Nancy) and CVB4E2 were used. VD2921 (GenBank accession number AF328683) was originally isolated from the cerebrospinal fluid of a patient with aseptic meningitis [20, 21]. The CVB1-10802 CDC strain was isolated in Argentina in 1998 by the Centers for Disease Control and Prevention (Atlanta, GA, USA). The CVB4E2 diabetogenic strain was kindly provided by Dr J.-W. Yoon (Calgary, AB, Canada). CVB3 (Nancy) was originally isolated in Connecticut in 1949 and is available from the American Type Culture Collection (www.lgcstandards-atcc.org/).
Cell culture and virus infection
HeLa and HepG2 cells were cultured in RPMI 1640 at 37°C and 5% CO2. CVB3 Nancy was propagated in HeLa cells and the titre was determined using a standard plaque assay. HeLa and HepG2 cells were mock infected or incubated with CVB3 Nancy (multiplicity of infection [MOI] 20 or 30 for HeLa and HepG2 cells, respectively) for 1 h.
PANC-1 cells were cultured in DMEM and infected with 0.01 MOI of CVB4E2. At 24 h postinfection, cells were washed three times with DMEM, resuspended in fresh medium and incubated at 37°C.
Specimens
Pancreases recovered from two patients with type 1 diabetes mellitus were selected from cohorts used previously [5]. The specimens were studied with approval from Greater Glasgow NHS Research Ethics Committee, and had been fixed in buffered formalin and paraffin embedded.
Human tissue array
A normal and cancer human tissue array was provided by the NHS Greater Glasgow and Clyde Bio Repository (UK).
Isolation and culture of human islets
Islets of Langerhans were isolated, cultured and infected in Uppsala University, Sweden, using a protocol approved by the local ethics committee, as previously described [22, 23].
RNA extraction and real-time RT-PCR
Total RNA from islets stored in RNAlater was extracted using RNeasy Plus (Qiagen AB, Sollentuna, Stockholm, Sweden). Up to 50 ng total RNA per sample was reverse transcribed using SuperScript II Reverse Transcriptase (Invitrogen, Stockholm, Sweden). Real-time PCRs were run with Power SYBR Green Master Mix (Applied Biosystems, Stockholm, Sweden). Predesigned gene-specific primer sets (QuantiTect Primer Assays, Qiagen) were used to detect CKB cDNA. PCR specificity was verified by melt-curve analysis of products.
Formalin-fixed paraffin embedding of islets or cultured cells
Islets were fixed in 4% paraformaldehyde at room temperature for 4 h, washed in PBS and dehydrated with increasing ethanol concentrations then xylene. Islets were paraffin embedded, sectioned (5 μm) and mounted on glass slides (Superfrost Plus, Thermo Scientific, Waltham, MA, USA).
Western blotting
Cellular extracts or recombinant purified proteins were separated using SDS-PAGE, transferred to nitrocellulose or polyvinylidene fluoride membranes and then incubated with the relevant primary antibodies overnight at 4°C: VP1 (1:400, Dako clone 5D8/1), CKB (1:500, Sigma Prestige [#HPA001254], Sigma, Poole, UK) and ATP5B (1:250, Sigma Prestige [#HPA001520]). Actin (1:30,000, MP Biomedicals, Cambridge, UK) served as a loading control. Immunoreactive bands were detected using horseradish peroxidase-labelled secondary antibodies (1:1,000, Bio-Rad, Hemel Hempstead, UK) and visualised using SuperSignal enhanced chemiluminescent substrate (Thermo Scientific, Rockford, IL, USA).
Immunohistochemistry
Sections of 4 μm were heated in 10 mmol/l citrate (pH 6.0) in a pressure cooker in a microwave oven at 800 W for 20 min, then cooled at room temperature for 20 min. Primary antibodies (Electronic Supplementary Material [ESM] Table 1) were applied and the Dako REAL EnVision Detection System (Dako, Ely, UK) was used for antigen detection. Clone 5D8/1 (1:2,000) was preincubated overnight at 4°C with peptides (10 μg/ml) or recombinant protein (at 1,000-fold molar excess) in blocking experiments.
Combined immunofluorescence
Rabbit anti-CKB, anti-ATP5B and mouse anti-VP1 (Dako) were detected with Alexa Fluor 568-conjugated anti-rabbit antibody or an Alexa Fluor 488 conjugated anti-mouse antibody (Invitrogen). DAPI (1:1,000, Invitrogen) was included in the final secondary incubation to stain cell nuclei. Sections were mounted in Vectashield hard-set mounting medium (Vector Laboratories, Peterborough, UK) under glass coverslips. Images were captured using either a Nikon Eclipse 80i microscope (Nikon, Guildford, UK) and overlaid using NIS-Elements BR 3.0 software (Nikon) or a Zeiss LSM510 meta confocal microscope (Zeiss, Cambridge, UK) to study the relative localisation of each antigen.
Peptide ELISA
High-binding enzyme immunoassay plates were coated with 1 μg/well of relevant peptide antigens (synthesised by GenScript, Piscataway, NJ, USA) in 50 mmol/l sodium carbonate buffer (pH 9.4). Plates were blocked with 5% normal goat serum (Vector Laboratories) in PBS and incubated for 2 h with varying dilutions of clone 5D8/1 in 5% normal goat serum/PBS. The plates were washed with PBS–Tween-20 (0.05%) and binding of the antibody was detected with alkaline phosphatase-conjugated anti-mouse IgG (1:4,000, Sigma) using p-nitrophenyl-phosphate (Sigma) as substrate. The reaction was stopped using 3 mol/l NaOH. Absorbance was read at 405 nm.
Results
Analysis of the cross-reactivity of 5D8/1 with CKB and ATP5B on western blots
It was initially established that cultured cell lines that are susceptible to infection with group B Coxsackieviruses express CKB and/or ATP5B (Fig. 1a, b). In both cell types, a strongly immunoreactive band of appropriate molecular mass was detected in both uninfected cells and cells harvested after infection with CVB3. The intensity of CKB labelling declined with increasing time postinfection, whereas the labelling of ATP5B was not altered during viral infection. When these extracts were probed with the enterovirus antibody 5D8/1, an immunoreactive band corresponding to that detected by the CKB antibody was again detected (Fig. 1a, b). In contrast, no band migrating in the position expected for ATP5B was labelled by 5D8/1 in either cell line.

Western blotting of CBV3-infected and mock-infected cell extracts or purified recombinant CKB and ATP5B. HeLa (a) and HepG2 (b) cells were infected with CVB3 Nancy (HeLa, 20 MOI; HepG2, 30 MOI). Total protein was isolated at various time points (0–8 h, as shown) postinfection. A total of 5 μg protein from each sample was loaded onto SDS–polyacrylamide gels and the expression of VP1, CKB and ATP5B was assessed on western blots. Actin was detected as the loading control. (c) A total of 100 ng recombinant CKB (rCKB) or ATP5B tagged with glutathione-S-transferase (rATP5B; molecular mass ∼95 kDa) was run on SDS–polyacrylamide gels and then electroblotted, and the membranes were incubated with 5D8/1 (1:400) anti-CKB (1:500) or anti-ATP5B (1:250) as shown. Immunoreactive bands were detected with chemiluminescent substrate
VP1 immunoreactivity was detected with clone 5D8/1 within 4 h of CVB3 infection in HeLa cells and this was maintained until at least 8 h postinfection (Fig. 1a). In HepG2 cells, the intensity of VP1 labelling was minimal at 4 h but increased dramatically by 6 and 8 h postinfection (Fig. 1b). Neither of the antisera directed against CKB or ATP5B detected the time-dependent expression of VP1.
To confirm these data, purified recombinant proteins (rCKB and rATP5B) were examined by western blotting (Fig. 1c) and it was found that, under denaturing conditions, rCKB was detected by 5D8/1 whereas rATP5B was not. In addition, an ELISA assay was developed in which peptide sequences corresponding to the epitopes purportedly recognised by 5D8/1 in VP1, CKB and ATP5B [19] were employed (Table 1). This confirmed that the relevant peptide epitopes within both VP1 (pVP1) and CKB (pCKB) are bound by 5D8/1, although pVP1 was bound more avidly (Fig. 2a). No binding to pATP5B was detected (Fig. 2a). In confirmation, the addition of an excess of pVP1 or pCKB led to displacement of the immunolabelling achieved with 5D8/1 in islet cells, whereas pATP5B did not displace the binding of 5D8/1 (Fig. 2b).

Analysis of the interactions between clone 5D8/1, CKB and ATP5B. (a) Binding of clone 5D8/1 to peptides derived from VP1 (triangles), CKB (squares) and ATP5B (diamonds) was analysed by ELISA. (b) Islet sections (×200 magnification) from a patient with type 1 diabetes were incubated with 5D8/1 and the ability of peptides derived from VP1 (pVP1), CKB (pCKB) and ATP5B (pATP5B) to displace the binding was studied. pCKB and pVP1 displaced the immunolabelling achieved with 5D8/1, whereas pATP5B did not
These results were confirmed using cell lines infected with Coxsackievirus (ESM Fig. 1), in which it was found that pCKB and pVP1 each abrogated the immunolabelling of VP1 by clone 5D8/1, while pATP5B was ineffective.
Analysis of the cross-reactivity of 5D8/1 with CKB and ATP5B by immunocytochemistry in fixed cells
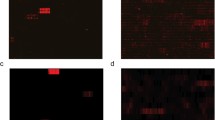
To establish whether clone 5D8/1 displays similar cross-reactivity under optimised conditions in fixed, paraffin-embedded cells and tissue, the antibody was applied to both HeLa and HepG2 cells stained in parallel with antisera raised against either CKB or ATP5B (Fig. 3a, b). As expected from the western blotting experiments, both CKB and ATP5B were present in the cells, although their expression was not uniform within the cell population. Importantly, none of the uninfected HeLa or HepG2 cells were stained positively by 5D8/1, despite the fact that both cell lines expressed abundant levels of CKB and ATP5B within the cell population. In contrast, when these cell lines were infected with CVB3, the majority of cells then became strongly immunopositive when stained with 5D8/1.

HeLa (a; ×400 magnification) and HepG2 (b; ×400 magnification) cells were infected with CVB3 Nancy and cells were collected 4 h (HeLa) or 6 h (HepG2) postinfection. Cells were fixed with formalin and embedded in paraffin and 5 μm sections were cut and mounted onto glass slides. Serial sections of mock and CVB3-infected cells were immunostained for the presence of enterovirus VP1 protein (antibody dilution 1:2,000; equivalent to 55 ng/ml), CKB (1:500) and ATP5B (1:500). (c) Formalin-fixed, paraffin-embedded, CVB4E2-infected PANC1 cells were immunostained for CKB (1:500) and VP1 (1:2,000). Images were captured at ×400 magnification (d) Photomicrographs (×600 magnification) of representative CVB3-infected PANC1 cells immunostained for CKB (red) and VP1 (green) revealed that CKB (white arrow) and VP1 (orange arrow) did not co-localise. Nuclear (DAPI) staining is shown in blue in the merged image
A third human cell line, PANC1, was also examined by immunocytochemistry. Like HeLa and HepG2 cells, the PANC1 line also expressed CKB under control (uninfected) conditions, but these cells did not stain positively when 5D8/1 was applied. In contrast, when PANC1 cells were infected with CVB4E2, they became immunopositive for VP1 (Fig. 3d). Dual-immunofluorescence labelling revealed that some cells were differentially immunopositive when stained with both antisera together (Fig. 3d). Thus, detection of CKB with Alexa Fluor 568 (red) revealed the presence of strongly stained cells that were immunonegative for enteroviral VP1 (Alexa Fluor 488 [green]). Conversely, other cells within the population were clearly immunopositive for VP1 (green) but negative for CKB (red).
Analysis of the cross-reactivity of 5D8/1 with CKB by immunocytochemistry in isolated human islets of Langerhans
Having established that, despite the possibility that 5D8/1 may cross-react with CKB on western blots and in ELISA assays, it does not do so in fixed cells under optimal conditions, we then examined the labelling patterns obtained in isolated human islets following fixation (ESM Fig. 2). Control islets were immunonegative for both VP1 and CKB, whereas islets infected with a strain of Coxsackievirus that establishes a more persistent infection (VD2921) were stained positively for CKB. Despite this, most cells did not stain positively when exposed to 5D8/1 in islets infected with VD2921. In contrast, infection of islets with an acutely lytic strain of Coxsackievirus (CVB1-11) resulted in the appearance of cells that were strongly positive for VP1, but that remained largely immunonegative when probed for CKB (ESM Fig. 2).
Analysis of the cross-reactivity of 5D8/1 with CKB and ATP5B by immunocytochemistry in pancreas sections from patients with recent-onset type 1 diabetes
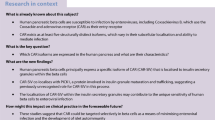
We next examined the situation more closely in pancreatic sections from patients with recent-onset type 1 diabetes and, as seen previously [4, 5], a small minority of beta cells were labelled by 5D8/1 (Figs 4, 5, 6). Some islets that contained only a few cells that were positive for VP1 also had cells that were strongly labelled by anti-CKB (Fig. 4). However, both the intensity of staining and the proportion of immunopositive cells were much higher when the sections were probed for CKB than when they were stained with 5D8/1. This is reminiscent of the situation seen in isolated islets that had been persistently infected with strain VD2921 (ESM Fig. 2). Furthermore, dual-immunofluorescence labelling revealed that islet cells that were strongly immunopositive for CKB (red) were not always stained positively for VP1 (green) and vice versa (Fig. 4d). Even in those cells that were stained positively with both antisera, higher-resolution analysis revealed that the staining of the two antigens was clearly separable, suggesting that they occupy a different subcellular localisation (Fig. 4e).

Photomicrographs (×200 magnification) of a representative islet from a patient with recent-onset type 1 diabetes. Serial sections were immunostained for (a) insulin, (b) VP1 and (c) CKB. (d) Fluorescence microscopy analysis (×400 magnification) of a representative islet from a patient with recent-onset type 1 diabetes revealed VP1-positive cells (green arrow), CKB-positive cells (red arrows) and double-positive cells (yellow arrow). (e) High-resolution analysis (×600 magnification) demonstrated that the staining of the two antigens (VP1 [green] and CKB [red]) was separable. (d, e) Nuclear (DAPI) staining is shown in blue

Photomicrographs (×200 magnification) of a representative islet from a patient with recent-onset type 1 diabetes. Serial sections were immunostained for (a) insulin, (b) ATP5B and (c) VP1. (d) Fluorescence microscopy analysis (×400 magnification) of a representative islet revealed both VP1-positive cells (green) and ATP5B-positive cells (red). Nuclei were stained with DAPI (blue). Sections were preincubated with (e) antibody diluent alone or (f) ATP5B antibody (10 μg/ml) overnight, prior to immunostaining for VP1 (green; 1:2,000)

Effects of the addition of an excess of either recombinant (r)CKB or a peptide epitope derived from CKB (pCKB) on the immunolabelling achieved with 5D8/1 in the islets of a patient with type 1 diabetes and in cultured cells infected with Coxsackievirus. (a) Islet sections were incubated with clone 5D8/1 (1:2,000) either alone or in the presence of an excess of pCKB or rCKB prior to immunodetection. (b) CVB5-infected Vero cells were immunostained with 5D8/1 (1:2,000) either alone or in combination with an excess of rCKB prior to immunodetection. Images were captured at ×200 magnification
A similar analysis was undertaken for the labelling of VP1 (with 5D8/1) and ATP5B in pancreas sections from patients with recent-onset type 1 diabetes. This revealed that the majority of islet cells expressed low levels of ATP5B (Fig. 5b). In contrast, very few cells stained positively with 5D8/1 (Fig. 5c). Moreover, when each antigen was detected in parallel using dual-immunofluorescence (Fig. 5d), the low level of ATP5B detected in the majority of cells (red) contrasted markedly with the pattern of staining of VP1 (green). Importantly, cells that were stained with 5D8/1 did not show any evidence of increased expression of ATP5B or any obvious change in its cellular localisation.
Finally, an antibody-blocking approach was employed and sections were incubated with an excess of anti-ATP5B to occupy the majority of available binding sites (Fig. 5f). Since the epitope purportedly recognised by 5D8/1 falls within the region of ATP5B against which the primary antiserum to this protein was raised [19], occupation of these sites by the primary antibody should preclude the subsequent binding of 5D8/1, if the target regions are common. This, however, was not the case (Fig. 5e, f).
As a further confirmation of the specificity of labelling achieved with 5D8/1, we also examined the ability of recombinant CKB to displace the immunolabelling achieved with this antibody in both islet sections (Fig. 6a) and in Coxsackievirus-infected cell lines (Fig. 6b). Importantly, rCKB failed to displace the immunolabelling achieved with 5D8/1 in either the islets or infected cells although, as noted in infected cells (ESM Fig. 1), the peptide derived from CKB was able to displace binding.
Tissue expression of immunoreactive VP1
As a further verification, a human tissue array consisting of 154 samples covering more than 80 cell and tissue types (including normal and tumour tissues) was probed with clone 5D8/1 (1:2,000). This yielded only two positive signals, in one of two samples of gastric body and normal colon (ESM Table 2). We also examined several mitochondria-rich tissues in greater detail, and such tissues (including liver and kidney) were uniformly negative when stained with 5D8/1 at a dilution of 1:2,000 (ESM Fig. 3).
Discussion
The concept that the triggering events leading to the initiation of islet cell autoimmunity and type 1 diabetes in humans may involve the development of a sustained enteroviral infection of islet beta cells has received widespread attention [1, 2]. Epidemiological evidence supports this proposition and, in rare cases, enteroviruses have even been isolated from pancreas samples recovered from patients with type 1 diabetes [1, 7]. In addition, a strong association has been found between the expression of viral antigens in the beta cells of patients and disease development [3–5]. However, much of the immunohistological evidence has relied on the use of clone 5D8/1 to detect the production of an enterovirus capsid protein (VP1). This antibody is used preferentially because it binds the target protein with high avidity in tissue samples and is capable of detecting a conserved sequence found in a wide range of different enterovirus serotypes [11, 24]. Accordingly, in the world’s largest study, more than 60% of pancreases recovered from patients with recent-onset type 1 diabetes contained islets that were immunopositive for enterovirus VP1 when stained with 5D8/1 [4]. This compared with only 6% immunopositivity in the islets of age-matched controls [4]. This evidence is striking, but it relies upon the specificity of clone 5D8/1, and this has been a cause of concern because of suggestions that this antibody can, if used under suboptimal labelling conditions, provide false-positive signals [18]. Importantly, Hansson et al have recently identified two potentially cross-reactive antigens and have argued that, in the beta cells of patients with recent-onset type 1 diabetes, labelling of these proteins could provide a basis for false positivity [19]. However, we now provide firm evidence to confirm that the immunoreactivity seen in islet cells does not derive from a cross-reaction between 5D8/1 with either CKB or ATP5B.
First, we re-examined the recent conclusion [19] that 5D8/1 labels CKB and ATP5B on western blots, and an immunoreactive band that co-migrated with a protein labelled by an antibody to CKB in various cultured cell lines was seen. Purified recombinant CKB was also detected by 5D8/1 on western blots, thereby confirming that clone 5D8/1 can label this enzyme under denaturing conditions. In contrast, no cross-reactivity was detected with a protein that co-migrated in the expected position of ATP5B and, when purified recombinant ATP5B was probed with clone 5D8/1, no immune-cross-reactivity was detected. In support of these data, we also found that the peptide antigens identified as the likely epitopes recognised by clone 5D8/1 [19] were differentially detected in an ELISA assay. As expected, the antibody bound with highest affinity to the peptide from VP1, but it also recognised that from CKB. In contrast, no binding was detected to the relevant peptide from ATP5B.
When cultured cells were fixed and paraffin embedded for analysis by immunohistochemistry using methods similar to those employed to detect the presence of viral VP1 in the pancreases of type 1 diabetic patients, it was apparent that both CKB and ATP5B are expressed in a majority of the population. However, these cells were unstained by clone 5D8/1. Despite this lack of cross-reactivity, the antibody labelled VP1 readily in enterovirus-infected cells. Thus, under optimal conditions, it is clear that neither CKB nor ATP5B are readily stained by clone 5D8/1 in cultured cells after fixation and paraffin embedding. Similar conclusions were also drawn from the examination of tissue microarrays, in which 80 different tissues were immunostained in parallel. Of these, only colon and stomach tissues stained positively with clone 5D8/1, and both of these are probable sites of infection by enteroviruses.
Our conclusions were reinforced by dual-immunocytochemical analysis of cultured cells following infection with enteroviruses. This allowed the firm identification of a population of cells expressing VP1 in addition to CKB, as well as further subpopulations that expressed each of these antigens alone. Thus, the antibodies were not cross-reactive with common antigens under the experimental conditions employed.
The study was then extended to include isolated human islets. When these were immunostained with antisera directed against CKB and VP1, respectively, no evidence of cross-reactivity was found. However, whereas CKB was detected only weakly in uninfected human islets, it was present in islets that had been infected with a strain of Coxsackievirus type B that establishes a persistent sublytic infection. This implies that CKB might become upregulated under such conditions. To our knowledge, such upregulation has not been noted previously in cells infected with enteroviruses, although it has been reported that CKB is required for the replication of certain strains of hepatitis C, another positive-strand RNA virus [25, 26]. Thus, it seems possible that CKB might play a hitherto unrecognised role in the development of a sustained infection of islet cells. This will require additional verification but, if confirmed, may have implications for the progression of such infections in the beta cells of patients developing type 1 diabetes. However, irrespective of this conclusion, it is clear that the altered expression of CKB does not lead to the development of a corresponding immunopositivity when the islets are stained with 5D8/1. This confirms that CKB is not a target for clone 5D8/1 under such conditions and also reveals that the synthesis of VP1 capsid protein is minimal under conditions of persistent enterovirus infection. This may, in turn, have relevance to the situation found in pancreas sections from patients with type 1 diabetes, where the proportion of immunopositive cells is very low (∼5% at best [5]), implying that production of VP1 occurs in only a few cells at any given time. As such, this would be consistent with a mechanism in which the majority of islet cells sustain a persistent sublytic infection and very few are involved in the active synthesis of viral capsid proteins.
Finally, dual-immunofluorescence detection of each protein in turn was undertaken and compared with the pattern of labelling achieved with clone 5D8/1. The data again implied that all of the antigens are separate and are detected independently by each antiserum employed. Most significantly, some cells were found to display strong immunoreactivity both to an antibody raised against CKB as well as to that against VP1. However, high-resolution analysis of the images clearly showed that the antigens were not co-localised within the cells.
These considerations raise the important question of why CKB is detected by clone 5D8/1 on western blots (and in ELISA assays) but not in tissue samples labelled in situ. Hansson et al [19] have argued that this may be because clone 5D8/1 only recognises the relevant epitopes present in CKB (and ATP5B) when the protein is expressed in stressed islet cells. However, they offer no molecular basis for this proposition, except to suggest that this may reflect a level of mitochondrial stress. We consider this to be unlikely, not least because CKB is a cytosolic protein [27, 28] and not normally localised within mitochondria. Rather, we suspect that, by reference to the crystal structure of CKB [29], the epitope detected by clone 5D8/1 is not normally accessible to the antibody in tissue sections. CKB is a dimer that, as noted by Eder et al [29], can only be dissociated under strongly denaturing conditions (i.e. similar to those used for western blotting). Thus, in tissue sections, it is probable that the protein structure is not disrupted sufficiently to allow access of the antibody, even after antigen retrieval. As a result, the selectivity for VP1 is maintained during immunohistochemical analysis whereas it may be lost on western blots. This hypothesis is supported by data revealing that a peptide epitope derived from CKB was capable of displacing the binding of 5D8/1 to both Coxsackievirus-infected cells and islet sections, whereas the full-length recombinant protein was not.
A further argument against the stress hypothesis of Hansson et al [19] is that infection of cells with enteroviruses that produce isoforms of VP1 that are not recognised by 5D8/1 do not stain positively with the antiserum [12, 13]. This confirms that the high level of stress imposed under these conditions does not lead to aberrant labelling of ATP5B or CKB.
Finally, we have recently had opportunity to conduct a more detailed concordance analysis across a range of different well-preserved pancreas samples from the JDRF’s nPOD (Network for Pancreatic Organ Donors with Diabetes) collection. In this analysis, the immunohistochemical labelling of VP1 was correlated with detection of the viral genome by in situ hybridisation. The results revealed a very high level of concordance (S. J. Richardson, G. Frisk, M. Oikarinen, J. E. Laiho, H. Hyoty, and N. G. Morgan; manuscript in preparation) and also showed that immunopositivity for VP1 correlated positively with hyperexpression of MHC class I molecules. Since MHC class I hyperexpression is likely to be driven by release of interferons, and this occurs in response to viral infection, these results add further weight to the view that detection of positive immunostaining of human beta cells by clone 5D8/1 under stringent conditions may reflect an underlying enteroviral infection.
Abbreviations
- CKB:
-
Creatine kinase B
- CV:
-
Coxsackievirus
- MOI:
-
Multiplicity of infection
References
Craig ME, Nair S, Stein H, Rawlinson WD (2013) Viruses and type 1 diabetes: a new look at an old story. Pediatr Diabetes 14:149–158
Taylor K, Hyöty H, Toniolo A, Zuckerman AJ (eds) (2013) Diabetes and viruses. Springer, New York
Dotta F, Censini S, van Halteren AG et al (2007) Coxsackie B4 virus infection of beta cells and natural killer cell insulitis in recent-onset type 1 diabetic patients. Proc Natl Acad Sci U S A 104:5115–5120
Richardson SJ, Willcox A, Bone AJ, Foulis AK, Morgan NG (2009) The prevalence of enteroviral capsid protein vp1 immunostaining in pancreatic islets in human type 1 diabetes. Diabetologia 52:1143–1151
Richardson SJ, Leete P, Bone AJ, Foulis AK, Morgan NG (2013) Expression of the enteroviral capsid protein VP1 in the islet cells of patients with type 1 diabetes is associated with induction of protein kinase R and downregulation of Mcl-1. Diabetologia 56:185–193
Ylipaasto P, Klingel K, Lindberg AM et al (2004) Enterovirus infection in human pancreatic islet cells, islet tropism in vivo and receptor involvement in cultured islet beta cells. Diabetologia 47:225–239
Yoon JW, Austin M, Onodera T, Notkins AL (1979) Isolation of a virus from the pancreas of a child with diabetic ketoacidosis. N Engl J Med 300:1173–1179
Gamble DR, Kinsley ML, FitzGerald MG, Bolton R, Taylor KW (1969) Viral antibodies in diabetes mellitus. Br Med J 3:627–630
Yeung WC, Rawlinson WD, Craig ME (2011) Enterovirus infection and type 1 diabetes mellitus: systematic review and meta-analysis of observational molecular studies. BMJ 342:d35
Toniolo A, Onodera T, Jordan G, Yoon JW, Notkins AL (1982) Virus-induced diabetes mellitus. Glucose abnormalities produced in mice by the six members of the Coxsackie B virus group. Diabetes 31:496–499
Samuelson A, Forsgren M, Sallberg M (1995) Characterization of the recognition site and diagnostic potential of an enterovirus group-reactive monoclonal antibody. Clin Diagn Lab Immunol 2:385–386
Oikarinen M, Tauriainen S, Penttila P et al (2010) Evaluation of immunohistochemistry and in situ hybridization methods for the detection of enteroviruses using infected cell culture samples. J Clin Virol 47:224–228
Richardson SJ, Willcox A, Hilton DA et al (2010) Use of antisera directed against dsRNA to detect viral infections in formalin-fixed paraffin-embedded tissue. J Clin Virol 49:180–185
Oikarinen M, Tauriainen S, Honkanen T et al (2008) Detection of enteroviruses in the intestine of type 1 diabetic patients. Clin Exp Immunol 151:71–75
Oikarinen M, Tauriainen S, Honkanen T et al (2008) Analysis of pancreas tissue in a child positive for islet cell antibodies. Diabetologia 51:1796–1802
Li Y, Bourlet T, Andreoletti L et al (2000) Enteroviral capsid protein VP1 is present in myocardial tissues from some patients with myocarditis or dilated cardiomyopathy. Circulation 101:231–234
Hammerstad SS, Tauriainen S, Hyoty H, Paulsen T, Norheim I, Dahl-Jorgensen K (2013) Detection of enterovirus in the thyroid tissue of patients with Graves’ disease. J Med Virol 85:512–518
Roivainen M, Klingel K (2009) Role of enteroviruses in the pathogenesis of type 1 diabetes. Diabetologia 52:995–996
Hansson SF, Korsgren S, Ponten F, Korsgren O (2013) Enteroviruses and the pathogenesis of type 1 diabetes revisited: cross-reactivity of enterovirus capsid protein (VP1) antibodies with human mitochondrial proteins. J Pathol 229:719–728
Frisk G, Diderholm H (2000) Tissue culture of isolated human pancreatic islets infected with different strains of coxsackievirus B4: assessment of virus replication and effects on islet morphology and insulin release. Int J Exp Diabetes Res 1:165–175
Yin H, Berg AK, Westman J, Hellerstrom C, Frisk G (2002) Complete nucleotide sequence of a Coxsackievirus B-4 strain capable of establishing persistent infection in human pancreatic islet cells: effects on insulin release, proinsulin synthesis, and cell morphology. J Med Virol 68:544–557
Skog O, Korsgren O, Frisk G (2011) Modulation of innate immunity in human pancreatic islets infected with enterovirus in vitro. J Med Virol 83:658–664
Moell A, Skog O, Ahlin E, Korsgren O, Frisk G (2009) Antiviral effect of nicotinamide on enterovirus-infected human islets in vitro: effect on virus replication and chemokine secretion. J Med Virol 81:1082–1087
Samuelson A, Forsgren M, Johansson B, Wahren B, Sallberg M (1994) Molecular basis for serological cross-reactivity between enteroviruses. Clin Diagn Lab Immunol 1:336–341
Hara H, Aizaki H, Matsuda M et al (2009) Involvement of creatine kinase B in hepatitis C virus genome replication through interaction with the viral NS4A protein. J Virol 83:5137–5147
Vassilaki N, Kalliampakou KI, Kotta-Loizou I et al (2013) Low oxygen tension enhances hepatitis C virus replication. J Virol 87:2935–2948
Wallimann T, Tokarska-Schlattner M, Schlattner U (2011) The creatine kinase system and pleiotropic effects of creatine. Amino Acids 40:1271–1296
Wallimann T, Wyss M, Brdiczka D, Nicolay K, Eppenberger HM (1992) Intracellular compartmentation, structure and function of creatine kinase isoenzymes in tissues with high and fluctuating energy demands: the ‘phosphocreatine circuit’ for cellular energy homeostasis. Biochem J 281:21–40
Eder M, Schlattner U, Becker A, Wallimann T, Kabsch W, Fritz-Wolf K (1999) Crystal structure of brain-type creatine kinase at 1.41 A resolution. Protein Sci 8:2258–2269
Acknowledgements
We thank D. Lobert (University Lille 2, Lille, France) for culture and infection of PANC1 cells. Details of the nPOD-V Consortium can be found at www.jdrfnpod.org.
Funding
This work was supported by funding from the European Union’s Seventh Framework Programme PEVNET (FP7/2007-2013) under grant agreement number 261441. Additional support was from a Diabetes Research and Wellness Foundation non-clinical research fellowship to SJR and from the Karolinska Institutet (KL), the Strategic Research Programme in Diabetes at the Karolinska Institutet (MF-T) and the Swedish Research Council (MF-T). The research was also performed with the support of the Network for Pancreatic Organ Donors with Diabetes (nPOD), a collaborative type 1 diabetes research project sponsored by the JDRF, and with a JDRF research grant awarded to the nPOD-V Consortium. Organ procurement organisations partnering with nPOD to provide research resources are listed at www.jdrfnpod.org/our-partners.php.
Duality of interest
HH is a minor (<5%) shareholder and member of the board of Vactech, which develops vaccines against picornaviruses. All other authors declare that there is no duality of interest associated with this manuscript.
Contribution statement
SJR was responsible for the study design and performed experiments, analysed data and wrote the manuscript. PL, SD, MAR, MO, JEL, KL, ES and TR performed experiments, analysed data and edited the manuscript. NC, DH, GF, HH, MF-T and AJB, contributed to the study design and reviewed and edited the manuscript. AKF collected samples, contributed to the study design and reviewed and edited the manuscript. NGM was responsible for the study design and wrote the manuscript. All authors reviewed and approved the final manuscript.
Author information
Authors and Affiliations
Consortia
Corresponding authors
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM Fig. 1
CVB5-infected Vero cells were immunostained with 5D8/1 (1:2000) either alone (no addition) or in combination with 10μg/ml of either pCKB, pATP5B or pVP1 prior to immunodetection of labelling. (PDF 213 kb)
ESM Fig. 2
Photomicrographs of representative isolated uninfected human islets (control) and human islets infected with CVB1-11 (strain 10802) or CVB4 (strain VD2921) immunostained to reveal the expression of VP1 (clone 5D8/1; left panels) or CKB (right panels). (PDF 204 kb)
ESM Fig. 3
Photomicrographs of normal human liver (A) and kidney (B) immunostained with clone 5D8/1 (1:2000). (PDF 313 kb)
ESM Table 1
(PDF 184 kb)
ESM Table 2
(PDF 181 kb)
Rights and permissions
About this article
Cite this article
Richardson, S.J., Leete, P., Dhayal, S. et al. Evaluation of the fidelity of immunolabelling obtained with clone 5D8/1, a monoclonal antibody directed against the enteroviral capsid protein, VP1, in human pancreas. Diabetologia 57, 392–401 (2014). https://doi.org/10.1007/s00125-013-3094-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-013-3094-7