
Abstract
Purpose
To find ways to reduce the rate of over-triage without drastically increasing the rate of under-triage, we applied a current guideline and identified relevant pre-hospital triage predictors that indicate the need for immediate evaluation and treatment of severely injured patients in the resuscitation area.
Methods
Data for adult trauma patients admitted to our level-1 trauma centre in a one year period were collected. Outpatients were excluded. Correct triage for trauma team activation was identified for patients with an ISS or NISS ≥ 16 or the need for ICU treatment due to trauma sequelae. In this retrospective analysis, patients were assigned to trauma team activation according to the S3 guideline of the German Trauma Society. This assignment was compared to the actual need for activation as defined above. 13 potential predictors were retained. The relevance of the predictors was assessed and 14 models of interest were considered. The performance of these potential triage models to predict the need for trauma team activation was evaluated with leave-one-out cross-validated Brier and logarithmic scores.
Results
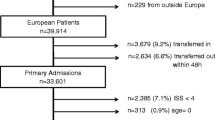
A total of 1934 inpatients ≥ 16 years were admitted to our trauma department (mean age 48 ± 22 years, 38% female). Sixty-nine per cent (n = 1341) were allocated to the emergency department and 31% (n = 593) were treated in the resuscitation room. The median ISS was 4 (IQR 7) points and the median NISS 4 (IQR 6) points. The mortality rate was 3.5% (n = 67) corresponding to a standardized mortality ratio of 0.73. Under-triage occurred in 1.3% (26/1934) and over-triage in 18% (349/1934). A model with eight predictors was finally selected with under-triage rate of 3.3% (63/1934) and over-triage rate of 10.8% (204/1934).
Conclusion
The trauma team activation criteria could be reduced to eight predictors without losing its predictive performance. Non-relevant parameters such as EMS provider judgement, endotracheal intubation, suspected paralysis, the presence of burned body surface of > 20% and suspected fractures of two proximal long bones could be excluded for full trauma team activation. The fact that the emergency physicians did a better job in reducing under-triage compared to our final triage model suggests that other variables not present in the S3 guideline may be relevant for prediction.



Similar content being viewed by others


References
Sasser SM, Hunt RC, Faul M, Sugerman D, Pearson WS, Dulski T, Wald MM, Jurkovich GJ, Newgard CD, Lerner EB, et al. Guidelines for field triage of injured patients: recommendations of the National Expert Panel on field triage, 2011. MMWR Recomm Rep. 2012;61(RR-1):1–20.
Bouillon B, Flohe S, Lendemans S, Ruchholtz S, Siebert H. Weissbuch schwerverletzten-versorgung. empfehlungen zur struktur, organisation und ausstattung sowie förderung von qualität und sicherheit in der schwerverletzten-versorgung in der bundesrepublik deutschland. Orthopädie Unfallchirurgie Mitteilungen Nachrichten. 2012;1(3, Supplement 1):1–35.
American College of Surgeon CoT. 2014 Resources for optimal care of the injured patient 2014. American College of Surgeons, Chicago.
Siebert H, Stürmer KM, Neugebauer E. S3-Leitlinie Polytrauma/Schwerverletzten-Behandlung. Orthopädie Unfallchirurgie Mitteilungen Nachrichten. 2011;1(1, Supplement 1):1–188.
Carron PN, Taffe P, Ribordy V, Schoettker P, Fishman D, Yersin B. Accuracy of prehospital triage of trauma patients by emergency physicians: a retrospective study in western Switzerland. Eur J Emerg Med. 2011;18(2):86–93.
Champion HR, Sacco WJ, Copes WS, Gann DS, Gennarelli TA, Flanagan ME. A revision of the Trauma Score. J Trauma. 1989;29(5):623–9.
Lefering R. Development and validation of the revised injury severity classification score for severely injured patients. Eur J Trauma Emerg Surg. 2009;35(5):437–47.
Baker SP, O’Neill B, Haddon W Jr, Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974;14(3):187–96.
Champion HR, Sacco WJ, Hunt TK. Trauma severity scoring to predict mortality. World J Surg. 1983;7(1):4–11.
American College of Surgeon. Resources for optimal care of the injured patient 2006. 1st ed. Chicago: American College of Surgeon, Committee on Trauma; p. 181.
Held L, Sabanes Bove D, Gravestock I. Approximate bayesian model selection with the deviance statistic. Stat Sci. 2015;30(2):242–57.
Steyerberg E. Clinical prediction models: a practical approach to development, validation and updating. New York: Springer; 2008.
Gneiting T, Raftery AE. Strictly proper scoring rules, prediction, and estimation. J Am Stat Assoc. 2007;102(477):359–78.
Brier GW. Verification of forecasts expressed in terms of probability. Mon Weather Rev. 1950;78(1):1.
R Development Core Team. R: a language and environment for statistical Computing. Vienna: R Foundation for Statistical Computing; 2016.
Mackersie RC. History of trauma field triage development and the American College of Surgeons Criteria. Prehospital Emerg Care. 2006;10(3):287–94.
Moore K. Trauma triage: right person, right place, right time. J Emerg Nurs. 2012;38(2):193–4. (Quiz 201).
Kohn MA, Hammel JM, Bretz SW, Stangby A. Trauma team activation criteria as predictors of patient disposition from the emergency department. Acad Emerg Med. 2004;11(1):1–9.
Engum SA, Mitchell MK, Scherer LR, Gomez G, Jacobson L, Solotkin K, Grosfeld JL. Prehospital triage in the injured pediatric patient. J Pediatr Surg. 2000;35(1):82–7.
Bond RJ, Kortbeek JB, Preshaw RM. Field trauma triage: combining mechanism of injury with the prehospital index for an improved trauma triage tool. J Trauma. 1997;43(2):283–7.
Santaniello JM, Esposito TJ, Luchette FA, Atkian DK, Davis KA, Gamelli RL. Mechanism of injury does not predict acuity or level of service need: field triage criteria revisited. Surgery. 2003;134(4):698–703. (Discussion 4).
Matsushima K, Chouliaras K, Koenig W, Preston C, Gorospe D, Demetriades D. Should we still use motor vehicle intrusion as a sole triage criterion for the use of trauma center resources? Injury. 2016;47(1):235–8.
Dowd MD, McAneney C, Lacher M, Ruddy RM. Maximizing the sensitivity and specificity of pediatric trauma team activation criteria. Acad Emerg Med. 2000;7(10):1119–25.
Mutschler M, Nienaber U, Munzberg M, Fabian T, Paffrath T, Wolfl C, Bouillon B, Maegele M. Assessment of hypovolaemic shock at scene: is the PHTLS classification of hypovolaemic shock really valid? Emerg Med J. 2014;31(1):35–40.
Senkowski CK, McKenney MG. Trauma scoring systems: a review. J Am Coll Surg. 1999;189(5):491–503.
Knopp R, Yanagi A, Kallsen G, Geide A, Doehring L. Mechanism of injury and anatomic injury as criteria for prehospital trauma triage. Ann Emerg Med. 1988;17(9):895–902.
Harbrecht BG, Franklin GA, Smith JW, Benns MV, Miller KR, Nash NA, Bozeman MC, Coleman R, O’Brien D, Richardson JD. Intubated trauma patients do not require full trauma team activation when effectively triaged. J Am Coll Surg. 2016;222(4):603–11.
Tinkoff GH, O’Connor RE. Validation of new trauma triage rules for trauma attending response to the emergency department. J Trauma. 2002;52(6):1153–8. (Discussion 8–9).
Cudnik MT, Werman HA, White LJ, Opalek JM. Prehospital factors associated with mortality in injured air medical patients. Prehosp Emerg Care. 2012;16(1):121–7.
Curtis K, Olivier J, Mitchell R, Cook A, Rankin T, Rana A, Watson WL, Nau T. Evaluation of a tiered trauma call system in a level 1 trauma centre. Injury. 2011;42(1):57–62.
Davis JS, Allan BJ, Sobowale O, Ivascu F, Orion K, Schulman CI. Evaluation of a new elderly trauma triage algorithm. Southern Med J. 2012;105(9):447–51.
Demetriades D, Sava J, Alo K, Newton E, Velmahos GC, Murray JA, Belzberg H, Asensio JA, Berne TV. Old age as a criterion for trauma team activation. J Trauma. 2001;51(4):754–6. (Discussion 6–7).
Kuhne CA, Ruchholtz S, Kaiser GM, Nast-Kolb D. Mortality in severely injured elderly trauma patients–when does age become a risk factor? World J Surg. 2005;29(11):1476–82.
Grossman MD, Miller D, Scaff DW, Arcona S. When is an elder old? Effect of preexisting conditions on mortality in geriatric trauma. J Trauma. 2002;52(2):242–6.
Justiniano CF, Evans DC, Cook CH, Eiferman DS, Gerlach AT, Beery PR, 2nd, Lindsey DE, Saum GE, Murphy CV, Miller SF, et al. Comorbidity-polypharmacy score: a novel adjunct in post-emergency department trauma triage. J Surg Res. 2012;172:348.
Acknowledgements
We thank D. Lanzi for basic data management.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
Approval by the local ethics committee was obtained for the analysis (KEK-ZH-Nr. 2013-0037). The study was conducted according to our institutional guidelines for good clinical practice and was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki and its later amendments. Due to this ethical approval no consent to participate in the study was needed, because only anonymised data were used.
Conflict of interest
Jensen KO, Heyard R, Schmitt D, Mica L, Ossendorf C, Simmen HP, Wanner GA, Werner CML, Held L and Sprengel K declare that they have no conflict of interest.
Funding
No sources of funding and/or publication are given.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Jensen, K.O., Heyard, R., Schmitt, D. et al. Which pre-hospital triage parameters indicate a need for immediate evaluation and treatment of severely injured patients in the resuscitation area?. Eur J Trauma Emerg Surg 45, 91–98 (2019). https://doi.org/10.1007/s00068-017-0889-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-017-0889-0