
Abstract
Objective
The aim of the study was to explore the relationship between perceived social support and quality of life (QOL) among recipients after kidney transplantation.
Methods
210 kidney transplant recipients participated in this survey, and survey tools included the Multidimensional Scale of Perceived Social Support (MSPSS) and the Medical Outcomes Study 36-item Short Form (SF-36).
Results
The mean scores of kidney transplant recipients for MSPSS three sub-scales family support, friend support, and significant others support were 6.18±0.90, 5.48±1.32, 5.65±1.05 respectively, while MSPSS total scale score was 5.77±0.91. The mean scores for SF-36 Physical Component Summary (PCS) and Mental Component Summary (MCS) were 47.48±6.70, 48.40±9.65 respectively. Recipients’ PCS scores were correlated to significant others support sub-scale score and MSPSS total score significantly (P<0.05), while MCS scores were correlated to three sub-scales scales and total scale score (P<0.01).
Conclusion
Perceived social support of patients after kidney transplantation was significant related to their quality of life. The higher perceived social support was associated with the better quality of life.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Avoid common mistakes on your manuscript.
I. Introduction
With the advances of transplant surgical techniques and immunosuppression treatment, the prognosis of kidney transplant recipients improved. However, what recipients and medical professional focus on is not only the survival rate and survival time, quality of life (QOL) has assumed immense importance. It found that worsening QOL in kidney transplant recipients was associated with the graft loss [1] and increased risk of mortality [2]. Precious studies showed that kidney transplantation itself significantly improved QOL of patients with chronic kidney disease and end-stage kidney disease, and recipients’ QOL scores were significantly better than their QOL scores before pre-transplant or those waiting for transplantation [1,3-4].However, compared with healthy subjects, the transplant recipients scored significantly worse [5].QOL is a multidimensional concept, including individual physical status, psychological status, social function, subjective judgment and satisfaction [6], therefore, it was easy to be influenced by many factors. Socioeconomic factors, such as lower family income, unemployment, lower education, living alone; physical factors, such as female, old, high BMI; clinical factors, such as recent critical illness and hospitalization, treatment side effects; psychological factors such as depression, may decrease recipients’ QOL scores [7-10].
Many studies confirmed the importance of psycho-social factors and its impact on QOL after kidney transplant [8], and social support is an important factor of psycho-social factors. As functional content of social relationships, social support can be categorized into four types of supportive behaviors or acts: emotional support, instrumental support, informational support, and appraisal support [11]. Social support have positive effects on people’s physical, mental, and social health, it is helpful for people to get stable social returns and positive emotional experience, such as security, belonging and so on [12]. Social support have subjective and objective dimensions, objective support means received support or enacted support while subjective support means perceived support [12]. Perceived social support is considered to be better predictor of psychological status than objectively measured social support [13].This cross-sectional study examines the perceived social support and QOL of kidney transplant recipients and explores the relationship between them, thereby providing a basis for health professionals and recipients to facilitate the development and implementation of specific interventions to improve the recipients’ perceived social support and QOL.
II. Subjects and methods
A. Participants
A cross-sectional study was carried out in one general hospital in Beijing between September 2012 and January 2014, and 210 kidney transplant recipients were recruited as study participants when they visited transplant follow-up clinics in the hospital. All participants were over 18 years with a functioning graft (meaning the recipient does not need dialysis) and were able to speak and read Chinese. Patients who had multiple organ transplants or who had more than one kidney transplant were excluded from this study.
B. Measurement
Data collection included social-demographic information, transplant specific information, and two standardized questionnaires assessing perceived social support and QOL. Social-demographic information included current age, gender, employment status, education, marital status, whether the transplant was self-paid or national insurance paid and family financial income. Transplant specific information, such as the date of transplant, the type and duration of dialysis and whether the kidney was from a living or cadaveric donor, was also collected.
1) Perceived Social Support
The Multidimensional Scale of Perceived Social Support (MSPSS) was adopted to assess the transplant recipient’s perceived social support. Th scale was developed by Zimet (1988) and demonstrated good internal reliability (Cronbach’s α=0.85~0.91) and good stability (test-retest value=0.72~0.85) [14]. Huang Li [15] translated MSPSS into Chinese version and examined the components of MSPSS with factor analysis, and this Chinese version was widely used in China. MSPSS includes 12 items and the items were divided into three sub-scales relating to the source of the support (family, friends, and significant other). Each of these sub-scales consists of four items, and each item ranges from very strongly disagree (score=1) to very strongly agree (score=7). Average score of four items in each sub-scale was the sub-scale score (range=1~7), and average score of all 12 items was the total score (range=1~7), with higher scores indicating higher perceived social support from their social networks. In this study, the Cronbach α coefficient of MSPSS sub-scales (family, friends, and significant other) and scale as a whole were 0.790, 0.891, 0.774,and 0.890 respectively.
2) Quality of life
Quality of life was measured by the Medical Outcomes Study 36-item Short Form (MOS SF-36) (Cronbach’s α=0.91), a 36-item self-administered brief questionnaire [16]. The questionnaire was translated into Chinese. It covers 8 domains (physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health) as well as two summary scores, Physical Component Summary (PCS) including physical functioning, role-physical, bodily pain, and general health sub-scales and Mental Component Summary (MCS) including vitality, social functioning, role-emotional, and mental health sub-scales [16]. Scores of each domain and field range from 0 to 100, with higher scores indicating better QOL. The MCS and PCS scores are standardized to a mean of 50, with scores above and below 50 indicating above and below average functioning, respectively. The Cronbach α coefficient of SF-36 PCS and MCS in our study were 0.705 and 0.805 respectively.
C. Ethical considerations
The study methodology was approved by the university ethics committee, which requires processes to ensure the confidentiality of all data. The purpose, risks and benefits of this study were explained to the recipients before they were asked to participate. They were assured that participation was voluntary, and that choosing not to participate would not influence their clinical care.
D. Data collection procedures
All data were collected in the transplant follow-up clinics by the help and supervision of the investigators who were trained before the survey to make sure that they were familiar with the requirements and methods of data collection. The principal investigator prepared survey questionnaires, including survey packets and a cover letter with a description of the project, response confidentiality, consent procedure, and investigator contact information. When recipients visited the follow-up clinic, investigators would judge whether they meet the criteria and invite they to participate if they meet the criteria. Consent was demonstrated by their completing and returning the surveys. The investigators were present at the clinic all the time until recipients completed and returned the survey packet. Recipients did not put their name or any other identifying information on the surveys.
E. Statistical analysis
Original data were input into Excel software and checked by two research assistants. Data was analyzed using SPSS 21.0 software. Continuous variables were expressed as mean ±standard deviation (SD) or range. Discrete variables were reported as frequency and percentage. Student’s t test and ANOVA were conducted to examine for differences in recipients’ quantitative data in different groups. The correlation between the perceived social support scores and QOL scores was assessed using the correlation coefficient. The level of significance was set at a p-value <0.05.
III. Results
A. Study enrollment and sample characteristics
A total of 210 questionnaires were distributed and all were returned (the return rate is 100%). The characteristics of the recipients are shown in Table 1. The mean age of recipients was 43.34±11.38 years (range 19-71) and 132 (62.9%) were male. One hundred and eleven (52.9%) of the recipients were employed and one hundred sixty-nine (80.5%) were married at the time of the survey. Twenty paid “out of pocket” for their healthcare. Forty-nine of the recipients had a middle school education or below, one hundred attended high school or technical secondary school and 61 got a college degree or above. Thirty (14.3%) received their graft from living donors. The meantime since transplantation was 3.20 ±2.59 years (range 0.09-17.06). One hundred and ninety-seven recipients had received peritoneal dialysis or hemodialysis before kidney transplantation.
B. Perceived social support
The mean and standard deviations of the three MSPSS sub-scales and total scale scores of recipients are shown in Table 2. The average total score was 5.77±0.91. Ranking MSPSS sub-scales scores in descending order, the three sub-scales were family, significant other, and friends. Analyzing the scores in different sub-scales (family support 6.18±0.90, friend support 5.48±1.32, significant others support 5.65±1.05) with ANOVA, the F value was 23.45 (P< 0.01). Comparing each two sub-scales, the T values of Student’s t test between family and friends sub-scales, family and significant other sub-scales were 6.40 and 5.65 (both P < 0.01), while T value between friends and significant other sub-scales was -1.42 (P> 0.05) indicating the social support kidney transplant recipients perceived from their family was higher than they perceived from their friends or significant others.
C. Quality of life
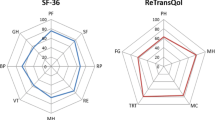
The SF-36 scores of the 210 kidney transplant recipients are shown in Table 3. The mean score of PCS and MCS were 47.48±6.70 and 48.40±9.65. Comparing the SF-36 scores of recipients with the scores of residents in Sichuan province [17] with Student’s t test, there were significant differences in all SF-36 dimensions except mental health(t=0.852, P>0.05). Scores of recipients in the remaining seven dimensions were statistically lower than Sichuan province residents’ scores(P<0.05).
D. Relationship between perceived social support and QOL
Table 4 details the correlation coefficients among the SF-36 two summary scores and each MSPSS sub-scale and total scale. It shows that SF-36 PCS score significantly related to MSPSS family sub-scale and total scale(P<0.05), while MCS score significantly related to all MSPSS sub-scales and total scale(P<0.05).
IV. Discussion
A. Perceived social support from family of kidney transplant recipients is high
In our study, the MSPSS was used to assess 210 kidney recipients’ perceived social support and it found that the total MSPSS score of recipients averaged 5.77±0.91, and their perceived support from their family was significantly higher than perceived support from friends or significant other. This result was similar to many other Chinese studies [18-19]. In their studies, it was found that social support of kidney transplant recipients was significantly high than norm in China. There may be two reasons. Firstly, chronic kidney diseases and end-stage kidney disease the patients suffered usually have longer course and serious medical conditions, and kidney transplantation costing much, so those who had high social support, especially material support, can tide over difficult waiting period and eventually be transplanted. Secondly, it may be related to objects’ social-demographic characteristic. In our study, mean age of recipients was 43.34 years, most of them had a wide social network compared to adolescent or elder; 80.5% of recipients got yet married, their spouses can give more support in the family; 76.7% of recipients graduated from high school or above, they may know more people and have more ways and strategies to seek support. This maybe the reason why the recipients in this study all had high social support.
Our study found that family support was the main source of recipients in three specific social support sources. Similar result appeared in the lung transplant recipients in China [20]. Physical function of recipients after transplant didn’t recover completely, so nearly half of participants in our study couldn’t get back to work, staying at home decreased their social interaction; for another, their primary caregivers usually were their direct relative, such as spouse, parents, sons and daughters in China [21], so their main support source was their family rather than their friends or significant others. However, support from friends, professional health-care workers, recipients’ club, and other organization or individual carried out important roles during their rehabilitation [22]. It is necessary to encourage recipients to participate in various social activities and productively utilize the help and support from others.
B. QOL of kidney transplant recipients is lower than the Chinese general public
In our study, SF-36 PCS and MCS scores of kidney transplant recipients were 47.48±6.70 and 48.40±9.65, respectively, both below 50. Besides, the SF-36 scores of kidney transplant recipients were significantly lower than the scores of Sichuan residents in seven dimensions of the SF-36, meaning that the QOL of kidney transplant recipients was apparently lower than the Chinese general public. This was similar to Quan’s research results [5]. Even if it’s confirmed that kidney transplantation can effectively improve recipients’ physical function and alleviate their psychological pressure, and then recipients had more opportunities to participate in family and social activities, however, there were still various problems may affect the quality of life of kidney transplant recipients, such as taking immunosuppressant for life and its uncomfortable side effect, risk of infection and rejection, heavy economic burden, limitation of activity, and regular follow-up to the clinic [23]. Medical staff should evaluate the postoperative quality of life of kidney transplant recipients in time and take effective measures to improve it.
C. Perceived social support of kidney transplant recipients is related to their quality of life
In our study, the PCS score of the SF-36 significantly correlated with MSPSS significant other sub-scale score and total scale score, while the MCS of the SF-36 significantly related to all MSPSS sub-scales and total scale scores, indicating there were significant positive correlation between perceived social support and QOL of kidney transplant recipients. The better subjective social support recipients perceived, the better quality of life they had. Similar results were found in previous research [23-25].
Social network and social support can influence the frequency and duration of exposure to pressure source, which in turn may enhance mental and physical health, for example, a supportive family may not need recipients to return to work soon after transplantation and they can rest and recover at home; social network and social support can promote health behaviors, for example, family remind recipients take medicine on time may help improve recipients’ medication compliance behavior; social network and social support have potential effects on organizational and community’s ability to garner its resources and solve problems, so kidney transplant recipients can receive funding for charity and community services easily [11]. Therefore, to improve QOL of kidney transplant recipients, some interventions including individual, family, and society-based approaches designed to enhance recipients' social support may be meaningful. The healthcare stuff should help kidney transplant recipients to know the importance of social support on their physical and mental health, assess recipients’ social network fully and accurately, encourage recipients to participate in various social activities and actively use the support from friends, ward-mates, community and other society organizations. For kidney transplantation costs much, providing economic support may be very important to some recipients, it is probably an effective way to establish more kidney transplant foundation or charity organization. It is good to set up kidney transplant club so that recipients can communicate their experience and puzzle with each other and reduce their anxiety and worry. The enterprise and institution should provide more employment opportunities to recipients, and not discriminate against recipients.
There are certain limitations in our study such as being a single-center cross-sectional survey. Additional multi-center studies of perceived social support and health-related quality of life in kidney transplant recipients are needed. Influence factors of social support and QOL are needed to be explored.
Acknowledgment
The study was funded by the National Natural Science Foundation of China: No.81171860. Special thanks to the participants in this study.
Transparency declarations
There is no conflict of interest. The results presented in this paper have not been published previously in whole or part.
References
N. Maglakelidze, T. Pantsulaia, I. Tchokhonelidze, L. Managadze, and A. Chkhotua, "Assessment of health-related quality of life in renal transplant recipients and dialysis patients." Transplantation proceedings. Vol. 43. No. 1. Elsevier, 2011.
M. Molnar-Varga, M. Z. Molnar, L. Szeifert, A. Z. Kovacs, A. Kelemen, A. Becze, .. and M. Novak, "Health-related quality of life and clinical outcomes in kidney transplant recipients." American Journal of Kidney Diseases 58.3 (2011): 444–452.
S. A. Joshi, N. Almeida, and A. Almeida, "Assessment of the perceived quality of life of successful kidney transplant recipients and their donors pre-and post-transplantation." Transplantation proceedings. Vol. 45. No. 4. Elsevier, 2013.
He Y, Shi X, Wang C, Wang Y, Li R. "Prospective cohort study on quality of life in patients undergoing renal transplantation or hemodialysis."; West China Medical Journal. 29.7 (2014): 1229–1232.
Quan S, Wang Z, Zhang Z. "Investigation of quality of life in renal transplant recipients and its influencing factors." Medical Science Journal of Central South China 42.2 (2014): 212–214.
Zhu Y. "Measurement and Evaluation of Quality of Life (QOL)." [M](2010).
S. Gentile, D. Beauger, E. Speyer, E. Jouve, B. Dussol, C. Jacquelinet, and S. Briançon, "Factors associated with health-related quality of life in renal transplant recipients: results of a national survey in France."Health Qual Life Outcomes 11.1 (2013): 88.
M. R. Malekahmadi, S. Rahimzadeh, M. L. Dezfuli Nejad, M. M. Lankarani, B. Einollahi, and S. Assari, "Importance of socioeconomic, clinical, and psychological factors on health-related quality of life in adolescents after kidney transplant." Exp Clin Transplant 9.1 (2011): 50–5.
J. M. Costa, and L. T. Nogueira, "Association between work, income and quality of life of kidney transplant recipient the municipality of Teresina, PI, Brazil." Jornal Brasileiro de Nefrologia 36.3 (2014): 332–338.
L. Prihodova, I. Nagyova, J. Rosenberger, R. Roland, J. P. Van Dijk, and J. W. Groothoff, "Impact of personality and psychological distress on health‐related quality of life in kidney transplant recipients." Transplant International 23.5 (2010): 484–492.
C A. Heaney, and B A. Israel, "Chapter 9 Social networks and social support, Health behavior and health education: Theory, research, and practice", 4th. ed; Jossey-Bass San Francisco, 2002.
Liu X, and Huang T. "Social support and its mechanism on mental health." Psychological Research,01( 2010): 3–8.
M. Barrera Jr, "Distinctions between social support concepts, measures, and models." American journal of community psychology 14.4 (1986): 413–445.
G. D. Zimet, N. W. Dahlem, S. G. Zimet, and G. K. Farley, "The multidimensional scale of perceived social support." Journal of personality assessment 52.1 (1988): 30–41.
Huang L, Jiang Q, and Ren W."Correlation between coping style, social support and psychosomatic symptoms in cancer patients." Chinese Mental Health Journal 10.4 (1996): 160–161.
J. E. Ware Jr, and C. D. Sherbourne, "The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection."Medical care (1992): 473–483.
Li N, Liu C, Li J and Ren X, "SF-36 evaluation values of urban and rural residents in Sichuan province in China."; Journal of West China University of Medical Sciences 32,(2001) :43–47.
Li J, Wu D, Dong Y, Xiao H, Tian J, Tian N, Liu M, and Zhu Y, "Investigation of social support status of kidney transplant patients." Nurs J Chin PLA 31.4 (2014): 21–23.
Liu X. "Investigation of social support in kidney transplant patients and its nursing intervention." Chinese Journal of Nursing 41.9 (2006): 854–857.
Chen L, Lin X, Huang D, and Mou X, "Quality of life in patients awaiting lung transplantation and the influencing factors" Journal of Nursing Science 26.10 (2011): 15–17.
Zhu S, and Lei J. "Study on the structure of social support supplier of renal transplantation recipients." Chinese Nursing Research 4 (2011): 878–879.
Guo H, and Fu Q. "Influence of social support and coping style on quality of life in renal transplant patients." Journal of Clinical Rehabilitative Tissue Engineering Research 11.34 (2007): 6721–6724.
Yang P, and Liu J. "The relationship between social support and quality of life of renal transplant patients." Medicine and Society 24.2 (2011): 41–43.
Zhou C, Wang N, and Liu Y. "A research on the social support and the quality of life of renal transplant patients." Chinese Medical Ethics 22.1 (2009): 125–127.
W. C. Chen, C. H. Chen, P. C. Lee, and W. L. Wang, "Quality of life, symptom distress, and social support among renal transplant recipients in Southern Taiwan: a correlational study."Journal of Nursing Research 15.4 (2007): 319–329.
Author information
Authors and Affiliations
Additional information
Authors’ profile

Xiaohong Lin, is a Registered Nurse, and she is now studying in School of Nursing, Beijing University of Chinese Medicine for her master degree.

Yabin Shang is now studying in School of Nursing, Beijing University of Chinese Medicine for her master degree.

Sha Teng is now studying in School of Nursing, Beijing University of Chinese Medicine for her master degree.

Dr. Hongxia Liu, corresponding author, is an Associate Professor for Master Program in School of Nursing, Beijing University of Chinese Medicine.

Liu Han is now studying in School of Nursing, Beijing University of Chinese Medicine for her master degree.
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made.
The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
To view a copy of this licence, visit https://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lin, X., Shang, Y., Teng, S. et al. Relationship between Perceived Social Support and Quality of Life among Kidney Transplant Recipients. GSTF J Nurs Health Care 3, 35 (2015). https://doi.org/10.7603/s40743-015-0035-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.7603/s40743-015-0035-1