
Abstract
Background
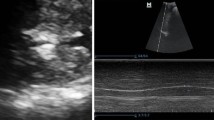
Chronic obstructive pulmonary disease (COPD) is a multisystem disorder that mainly besides the lungs also affects the muscle mass. The force generated by the respiratory muscles decreases, resulting in a negative effect on ventilation and exercise capacity. Recent studies have reported that M-mode ultrasonography is reliable and relatively easy to use for assessment of diaphragmatic motion.
Objective
To evaluate diaphragmatic excursion by M-mode ultrasonography in patients with COPD and to correlate it with different clinical and ventilatory variables.
Patients and methods
A total of 40 patients with COPD who attended Chest Diseases Department Al-Azhar University Hospitals from January 2017 to May 2017 were recruited in this study. Informed consent was obtained. Diagnosis and severity of COPD was made according to the Global Initiative for Chronic Obstructive Lung Disease guidelines. All patients in this study were subjected to full medical history, clinical examination, pulmonary function tests, calculation of BMI, arterial blood gases analysis, 6-min walk test, and ultrasound imaging of the diaphragm.
Results
Diaphragmatic excursion during quiet breathing did not differ significantly between the patients and the controls (P=0.085). However, during deep breathing, the degree of diaphragmatic excursion was lower in the patients (P=0.001). Diaphragmatic excursion during deep breathing correlated significantly with disease severity(r=0.86); the percentage of the predicted forced expiratory volume in the first second, forced vital capacity, and forced expiratory volume in the first second/forced vital capacity (r=0.84, 0.72, and 0.80, respectively); and the 6-min walk test (r=0.47). Conclusion M-mode ultrasonography is an easy, noninvasive and inexpensive method for evaluation of diaphragmatic excursion. Patients with COPD had significantly lower diaphragmatic excursion than normal ones.
Article PDF
Similar content being viewed by others

References
Similowski T, Yan S, Gauthier AP, Macklem PT, Bellemare F. Contractile properties of the human diaphragm during chronic hyperinflation. N Engl J Med 1991; 325:917–923.
Levine S, Nguyen T, Kaiser LR. Human diaphragm remodeling associated with chronic obstructive pulmonary disease: clinical implications. Am J Respir Crit Care Med. 2003; 168:706–713.
Barreiro E, de la Puente B, Minguella J, Corominas JM, Serrano S, Hussain S, et al. Oxidative stress and respiratory muscle dysfunction in severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2005; 171:1116–1124.
Ottenheijm CA, Heunks LM, Sieck GC, Zhan WZ, Jansen SM, Degens H, et al. Diaphragm dysfunction in chronic obstructive pulmonary disease.Am J Respir Crit Care Med 2005; 172:200–205.
Lahgi F, Shaik HS, Morales D, Sinderby C, Jubran A, Tobin MJ. Diaphragmatic neuromechanical coupling and mechanisms of hypercapnia during inspiratory loading. Respir Physiol Neurobiol 2014; 198:32–41.
Baria MR, Shahgholi L, Sorenson EJ, Harper CJ, Lim KG, Strommen JA. B-mode ultrasound assessment of diaphragm structure and function in patients with COPD. Chest 2014; 146:680–685.
DiNino E, Gartman EJ, Sethi JM, McCool FD. Diaphragm ultrasound as a predictor of successful extubation from mechanical ventilation. Thorax 2014; 69:423–427.
Gottesman E, McCool FD. Ultrasound evaluation of the paralyzed diaphragm. Am J Respir Crit Care Med 1997; 155:1570–1574.
Kim WY, Suh HJ, Hong SB, Koh Y, Lim CM. Diaphragm dysfunction assessed by ultrasonography: influence on weaning from mechanical ventilation. Crit Care Med 2011; 39:2627–2630.
Dos Santos Yamaguti WP, Paulin E, Shibao S, Chammas MC, Salge JM, Ribeiro M, et al. Air trapping: the major factor limiting diaphragm mobility in chronic obstructive pulmonary disease patients. Respirology 2008; 13: 138–144.
Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease, updated 2010. Available at: http://www. goldcopd.org. [Accessed at 15 Feb 2011].
Vestbo J, Hurd SS, Agustí AG, Jones PW, Vogelmeier C, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 2013; 187:347–365.
American Thoracic Society (ATS). ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med 2002; 166:111–117.
Harris RS, GiovannettiM, Kim BK. Normal ventilatorymovement of the right hemidiaphragm studied by ultrasonography and pneumotachography. Radiology 1983; 146:141–144.
Boussuges A, Gole Y, Blanc P. Diaphragmatic motion studied by M-mode ultrasonography: methods, reproducibility, and normal values. Chest 2009; 135:391–400.
Testa A, Soldati G, Giannuzzi R, Berardi S, Portale G, Gentiloni Silveri N. Ultrasound M-mode assessment of diaphragmatic kinetics by anterior transverse scanning in healthy subjects. Ultrasound Med Biol 2011; 37:44–52.
Paulin E, Yamaguti WP, Chammas MC, Shibao S, Stelmach R, Cukier A, et al. Influence of diaphragmatic mobility on exercise tolerance and dyspnea in patients with COPD. Respir Med 2007; 101:2113–2118.
Aka Aktürk U, çaglayan BN, Fidan A, Salepçi B, Turan D, Sener Cömert S, et al. The evaluation of diaphragmatic motion by M-mode ultrasonography in chronic obstructive lung diseases. Eur Respir J 2013; 42(Suppl 57):P1922.
Takazakura R, Takahashi M, Nitta N, Murata K. Diaphragmatic motion in the sitting and supine positions: healthy subject study using a vertically open magnetic resonance system. J Magn Reson Imaging 2004; 19: 605–609.
De Troyer A. Effect of hyperinflation on the diaphragm. Eur Respir J 1997; 10:708–713.
Kang HW, Kim TO, Lee BR, Yu JY, Chi SY, Ban HJ, et al. Influence of diaphragmatic mobility on hypercapnia in patients with chronic obstructive pulmonary disease. J Korean Med Sci 2011; 26:1209–1213.
Scheibe N, Sosnowski N, Pinkhasik A, Vonderbank S, Bastian A. Sonographic evaluation of diaphragmatic dysfunction in COPD patients. Int J Chron Obstruct Pulmon Dis 2015; 10:1925–1930.
American Thoracic Society; European Respiratory Society. ATS/ERS statement on respiratory muscle testing. Am J Respir Crit Care Med 2002; 166:518–624.
Author information
Authors and Affiliations
Corresponding author
Additional information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work noncommercially, as long as the author is credited and the new creations are licensed under the identical terms.
Rights and permissions
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Amin, A., Zedan, M. Transthoracic ultrasonographic evaluation of diaphragmatic excursion in patients with chronic obstructive pulmonary disease. Egypt J Bronchol 12, 27–32 (2018). https://doi.org/10.4103/1687-8426.217411
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.4103/1687-8426.217411