Abstract
Pain scientists and clinicians search for objective measures of altered nociceptive processing to study and stratify chronic pain patients. Nociceptive processing can be studied by observing a combination of nociceptive detection thresholds and evoked potentials. However, it is unknown whether the nociceptive detection threshold measured using a go-/no-go (GN) procedure can be biased by a response criterion. In this study, we compared nociceptive detection thresholds, psychometric slopes, and central evoked potentials obtained during a GN procedure with those obtained during a two-interval forced choice (2IFC) procedure to determine (1) if the nociceptive detection threshold during a GN procedure is biased by a criterion and (2) to determine if nociceptive evoked potentials observed in response to stimuli around the detection threshold are biased by a criterion. We found that the detection threshold was higher when assessed using a GN procedure in comparison with the 2IFC procedure. During a GN procedure, the average P2 component increased proportionally when averaged with respect to detection probability, but showed on-off behavior when averaged with respect to stimulus detection. During a 2IFC procedure, the average P2 component increased nonlinearly when averaged with respect to detection probability. These data suggest that nociceptive detection thresholds estimated using a GN procedure are subject to a response criterion.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pain scientists and clinicians search for objective criteria to identify impaired nociceptive processing for the purpose of stratification and treatment of chronic pain patients (Mouraux & Iannetti, 2018). With this aim, nociceptive processing of patients is usually evaluated using a combination of neurophysiological and psychophysical testing. In this field, there is a recent renewed interest in the assessment of mechanical, thermal, and electric detection thresholds. However, the interpretation of these thresholds could alter depending on the procedure through which these thresholds are measured.
Recently, we developed a method to assess nociceptive processing by quantifying the effect of nociceptive stimulus properties on detection probability and cortical evoked potentials (EPs). In this method, we stimulate nociceptive afferents in the skin by intra-epidermal electric stimulation with a specialized electrode (Steenbergen et al., 2012). This method selectively activates nociceptive afferents in the skin provided that low stimulation currents are used, for which a limit of twice the detection threshold was proposed as a rule of thumb (Mouraux et al., 2010). Stimulus amplitudes are centered around the detection threshold by an adaptive psychophysical method of limits (Doll et al., 2015) and the electroencephalogram (EEG) is recorded in response to each stimulus. This allows us to record the combination of nociceptive detection thresholds and evoked potentials in response to nociceptive stimulation. We recently showed that nociceptive detection thresholds of single-pulse and double-pulse intra-epidermal electric stimuli can be used to observe peripheral and central changes of nociception following deafferentation by capsaicin (Doll, van Amerongen, et al., 2016b). Nociceptive evoked potentials can be used as a marker for altered central nociception, for example, in central sensitization (van den Broeke et al., 2015), attentional modulation (Legrain et al., 2002), or placebo analgesia (Wager et al., 2006). The combination of both methods allowed us to evaluate the effect of temporal stimulus properties on nociceptive detection threshold and evoked potentials in healthy participants (van den Berg et al., 2020; van den Berg & Buitenweg, 2021), and could be used to study impaired nociceptive processing in chronic pain patients in future studies.
Although nociceptive detection thresholds appear sensitive to induced changes in peripheral and central nociceptive processing, it remains unclear how observed detection thresholds are related to the underlying physiological systems. In all of our studies, we used an adaptive method of limits with a go/no-go (GN) procedure to approach and estimate the detection threshold, i.e.: (1) an adaptive series of stimuli is presented, (2) the participant has to indicate when a stimulus was detected, and (3) the stimulus amplitude is increased or decreased depending on stimulus detection. Subsequently, logistic regression was used to estimate the detection threshold and slope based on all available data. Although the obtained detection threshold is used to probe central or peripheral nervous function, most studies appear to disregard the fact that these thresholds could also be modulated by a sensory, perceptual, or decision criterion (Georgeson, 2012), which we will refer to more generally as a “response criterion.” We can describe the role of such a response criterion during a GN procedure using signal detection theory (Kingdom & Prins, 2016), by assuming that the response of a participant is based on the quantity of sensory evidence, defined as any type of sensory neural activity that is available for decision making in the brain. During a GN procedure, the participant will report a stimulus as detected when the sensory evidence exceeds the response criterion (Fig. 1). It remains unknown whether nociceptive detection thresholds estimated using a GN procedure indeed depend on such a response criterion.

Stimulus detection as viewed by signal detection theory. Sensory evidence consists of random noise (e.g., spontaneous neural activity) and sensory information (e.g., stimulus-evoked activity). The total amount of sensory evidence during one time interval can be described by a probability density function. During a go/no-go (GN) procedure, the stimulus is reported as detected when the sensory evidence during one interval exceeds a response criterion. During a two-interval forced choice (2IFC) procedure, the interval is correctly classified when the sensory evidence during the interval with stimulus exceeds sensory evidence of the interval without stimulus
In addition, it remains unexplored how evoked cortical activity, measured in some studies as a more “objective” measure of altered nociceptive or somatosensory processing, is affected by the potential dependence on a response criterion in a GN procedure. The perception of a (change in) visual stimulus results in the generation of the famous P3 (also referred to as P300) peak in the event-related potential (Picton, 1992), which is considered a key marker of conscious access to visual information (Rutiku et al., 2015; Salti et al., 2012). The P2 in response to nociceptive stimulation represents multi-modal brain activity similar to the visual P3, with an important role in the generation of conscious perception (Mouraux & Iannetti, 2009). The P2 in response to nociceptive stimulation is also described as a response to stimulus salience (Legrain et al., 2011). This interpretation of the P2 is closely related to the other (i.e., a marker of conscious access), as a more salient stimulus will have a higher probability of being consciously detected, but is not the same. It therefore remains unknown how the P2 in response to near-threshold stimuli can be interpreted. And if the P2 is a marker of conscious access to information, will there be a P2 when there is sufficient sensory evidence to support decision making (i.e., to correctly classify the interval during the two-interval forced choice (2IFC) procedure) or only when sensory evidence exceeds the response criterion (i.e., when stimulus detection is reported during the GN procedure)?
The potential influence of a response criterion can be omitted by using a 2IFC procedure (Kingdom & Prins, 2016), where participants are asked to choose during which of two observation intervals a stimulus was applied. During the 2IFC procedure, the interval is reported correctly if the sensory evidence during an interval with a stimulus, i.e., with both spontaneous and stimulus-evoked neural activity, is larger than the sensory evidence during an interval without a stimulus, i.e., with only spontaneous neural activity (Fig. 1). In this study, we compared nociceptive detection thresholds, psychometric slopes, and the evoked P2 obtained during a GN procedure with those obtained during a 2IFC procedure with two objectives. Our first objective was to determine if the nociceptive detection threshold during a GN procedure is dependent on a response criterion, i.e., resulting in a different detection threshold with respect to the 2IFC threshold. Our second objective was to explore how the evoked P2 during each procedure is related to the detection probability and to stimulus detection itself.
Methods
The results presented in this work include measurements of the detection threshold using a GN and a 2IFC procedure in randomized order. A total of 25 participants was included and performed both procedures. In the last 15 participants, the EEG was also recorded during task performance. The experiments were performed at the University of Twente, The Netherlands, and were approved by the local Medical Review and Ethics Committee. All experiments were performed in accordance with the Declaration of Helsinki.
Participants
A total of 25 healthy participants (12 males and 13 females, age 19–30 years) were included in this study. The inclusion criterion was age between 18 and 40 years old. Exclusion criteria were skin abnormalities at the site of stimulation, diabetes, implanted stimulation devices, pregnancy, usage of analgesics within 24 h before the experiment, the consumption of alcohol or drugs within 24 h before the experiments, pain complaints at the time of the experiment, a medical history of chronic pain, or any language problems that would impede communication with the participant. All participants provided written informed consent before participation in the experiment.
Stimuli
Each stimulus consisted of cathodic square wave electric pulses generated by a constant current stimulator (NociTRACK AmbuStim, University of Twente, Enschede, The Netherlands). Stimuli were delivered to the epidermis at the back of the right hand via a custom-made electrode consisting of five inter-connected microneedles protruding 0.5 mm from the electrode surface. Intra-epidermal electric stimulation preferentially activates nociceptive afferents in the skin, provided that stimuli remain below twice the detection threshold (Mouraux, 2010; Poulsen et al., 2020). A previous validation study of the electrode used in this study demonstrated that electric pulses resulted in a sharp pricking sensation (Steenbergen et al., 2012).
Previous studies noted that two intra-epidermal electric pulses repeated at a short inter-pulse interval (between 5 and 40 ms) result in a much lower detection threshold than a single intra-epidermal electric pulse (Doll, Maten, et al., 2016a; Mouraux et al., 2014; van den Berg & Buitenweg, 2021), suggesting an effect of temporal summation on detection probability. In this study, we therefore investigated the potential influence of response criterion on both single- and double-pulse stimuli. Two stimulus types were used during the experiment, which were both shown to result in similar latencies of response times and evoked N1, N2, and P2 peaks in comparison with earlier studies using intraepidermal and laser stimulation (van den Berg & Buitenweg, 2021):
-
One square pulse with a pulse width of 210 μs.
-
Two square pulses with a pulse width of 210 μs and an inter-pulse interval of 10 ms.
Familiarization
Participants were instructed to press and hold a button. For familiarization with the sensation of intra-epidermal stimuli, participants were stimulated with a series of pulses with a stepwise (0.025 mA) increasing amplitude and instructed to release the button when a stimulus was clearly perceived for at least two times. For an initial estimate of the detection threshold for each stimulus type, participants were stimulated with a series of pulses with a stepwise (0.025 mA) increasing amplitude and instructed to release the button when any sensation was perceived that they ascribed to stimulation.
Go/no-go procedure
Participants were seated upright in a chair and asked to focus on the site of stimulation. Detection thresholds were estimated and tracked using an adaptive procedure (Doll et al., 2015). Participants were instructed to press and hold a button, and to briefly release the button when any sensation was perceived that they ascribed to stimulation (Fig. 2). For the adaptive procedure, the stimulus amplitude was randomly picked from a vector of five stimulus amplitudes with a step size of 0.025 mA initialized around the initial estimate of the detection threshold. The vector of amplitudes was decreased by 0.025 mA when a stimulus was reported as detected and increased by 0.025 when the participant did not release the response button. This process was repeated independently for every stimulus type, with the order of stimulus type randomized, for a total of 130 stimuli per type.

The go/no-go (GN) and the two-interval forced choice (2IFC) procedure used to measure the nociceptive detection threshold for single and double pulse intra-epidermal electric stimuli (left), and the adaptive procedure used to converge to the detection threshold in both procedures (right). The stimulus is randomly selected from a vector of five equidistant stimulus amplitudes (with a step size of 0.025 mA, indicated by []). When a stimulus is not detected (indicated by open markers), this vector is decreased by 0.025 mA (GN) or 0.075 mA (2IFC). When a stimulus is detected (indicated by closed markers), this vector is increased by 0.025 mA (both procedures)
Two-interval forced choice procedure
Participants were seated upright in a chair and asked to focus on the site of stimulation. Detection thresholds were estimated and tracked using an adapted version of the adaptive procedure in a previous version. Participants were stimulated during one of two time intervals (Fig. 2), marked by an auditory cue. After each set of two time intervals, participants were asked to indicate during which time interval they were stimulated. For the adaptive procedure, the stimulus amplitude was randomly picked from a vector of five stimulus amplitudes with a step size of 0.025 mA initialized around the initial estimate of the detection threshold. The vector of amplitudes was decreased by 0.075 mA when the reported time interval was incorrect and increased by 0.025 when the reported time interval was correct. Note that the decrease after an incorrect answer [dincorrect] is three times larger than the increase after a correct answer [dcorrect], as this ratio is governed by the value of the detection threshold, \( \frac{d_{incorrect}}{d_{correct}+{d}_{incorrect}}={p}_{threshold} \), where pthreshold is equal to 0.5 for a GN procedure and equal to 0.75 for a 2IFC procedure. This process was repeated independently for every stimulus type, with the order of stimulus type randomized, for a total of 130 stimuli per type.
Electroencephalography
The scalp EEG was recorded at 32 channels (international 10/20 system) using a REFA amplifier (TMSi B.V., Oldenzaal, The Netherlands) with a sampling rate of 1,024 Hz. Participants were asked to fix their gaze at a spot on the wall. Electrode impedance was kept below 20 kΩ.
Nociceptive detection threshold
The nociceptive detection probability was estimated by global optimization of the negative log-likelihood using an implementation of the GlobalSearch algorithm (Ugray et al., 2007) in combination with an interior-point algorithm to find local minima (Coleman & Li, 1996) in Matlab. In the case of the GN procedure (Eq. 1), the detection probability was modeled using a cumulative normal distribution as a function of an intercept [β0], additive temporal summation of the first pulse [βA1A] and the second pulse [βA2A], and a linear drift over time [βtt]. In the case of a 2IFC procedure (Eq. 2), this function was adapted to account for a 50% guessing rate at low stimulus amplitudes. Differences between thresholds estimated using a 2IFC and a GN procedure were assessed based on Bland-Altman analysis (Bland & Altman, 1986), using the BlandAltmanPlot function available on the Matlab file exchange.
Detection probability for a go/no-go procedure:
Detection probability for a two-interval forced choice procedure:
Evoked brain activity
The EEG was preprocessed using the FieldTrip toolbox (Oostenveld et al., 2011). Eye-blinks, eye movement, and movement artefacts were corrected using independent component analysis (Delorme et al., 2007). Epochs with excessive EMG activity or remaining movement artefacts were removed by visual inspection. Grand average EP waveforms of detected and non-detected stimuli (GN) and of correct and incorrect stimuli (2IFC) were computed at T7-F4 and CPz-M1M2 and tested for significance with respect to baseline and with respect to the other condition using cluster-based nonparametric permutation tests (Maris & Oostenveld, 2007). In addition, grand average EP waveforms were computed for four levels of detection probability (.00–.25, .25–.50, .50–.75, and .75–1.0) for both procedures. Significance of the effect of detection probability on the EEG was assessed by fitting a linear mixed model (3) to the EEG at each latency, and obtaining the t-value of effect coefficients using Satterthwaite’s approximation of the degrees of freedom. The t-values were corrected for retesting over time using the Benjamini-Hochberg correction (Hochberg & Benjamini, 1995). The average P2 amplitude for each of the four levels of detection probability was determined by averaging over time between 380 ms and 420 ms post-stimulus.
Results
Nociceptive detection threshold
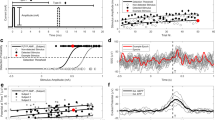
A typical example of an experiment with the GN and the 2IFC procedure is displayed in Fig. 3. During the GN procedure, the detection threshold for single-pulse stimuli was larger than the detection threshold for double-pulse stimuli. Both thresholds showed a small increasing drift over time. During the 2IFC procedure, the thresholds were equal for single-pulse and double-pulse stimuli. Drift over time was small or not present.

Typical example of detection thresholds obtained when performing a go/go-no (GN) procedure (left) and when performing a two-interval forced choice (2IFC) procedure (right). When performing a 2IFC procedure, detection thresholds appeared to equalize for both stimulus types. Detected and non-detected (GN) or correct and incorrect (2IFC) stimuli are depicted by closed and open circles, respectively
Detection thresholds and slopes estimated using a GN procedure were compared to detection thresholds and slopes estimated using a 2IFC procedure. Note that four participants were excluded from comparison, because the optimizer failed to achieve a solution for either the GN or 2IFC procedure, and one participant was excluded because of inadequate task performance, defined as a detection rate lower than 0.2 during the GN procedure. Detection thresholds and slopes for the remaining 20 participants are displayed on the left in Fig. 4. The detection threshold for single-pulse stimuli during a 2IFC procedure was significantly lower than the detection threshold for single-pulse stimuli during a GN procedure. The psychometric slope for single-pulse stimuli during a 2IFC procedure was significantly larger than the psychometric slope for single-pulse stimuli during a GN procedure. Bland-Altmann plots for analysis of the individual differences between threshold and slopes estimated using a GN procedure, and threshold and slopes estimated using a 2IFC procedure, are displayed on the right in Fig. 4. For single-pulse stimuli, detection thresholds are positively biased and slopes are negatively biased when estimated using a GN procedure. This bias of estimated thresholds appears to increase with respect to the estimated value. For double-pulse stimuli, thresholds and slopes were unbiased.

Individual results and boxplots of the detection thresholds and slopes for single-pulse (SP) and double-pulse (DP) stimuli during the go/no-go (GN) and the two-interval forced choice (2IFC) procedure for a total of 20 participants. Significance is indicated with * (p < .05), ** (p <. 01), and *** (p < .001). Detection thresholds for single-pulse stimuli were significantly lower and psychometric slopes were significantly larger when assessed in a 2IFC procedure in comparison with the GN procedure. Bland-Altmann plots are shown on the right, and indicate that single-pulse detection thresholds and slopes are significantly biased and show that the difference between GN and 2IFC threshold estimates increases as the mean value of the estimates increases
Evoked brain activity
Grand average evoked potentials at Cz-M1M2 acquired during both procedures are displayed in Fig. 5. There was a significant contrast between evoked potentials in response to detected and non-detected stimuli in the GN procedure, and correct and incorrect trials in the 2IFC procedure. For the GN procedure, the evoked potential was significantly larger than baseline for detected as well as non-detected stimuli. For the 2IFC procedure, the evoked potential was only significantly larger than baseline for correct trials. Note that the average evoked potential for correct trials (2IFC) was lower than the average evoked potential for detected stimuli (GN), but might be confounded by inclusion of trials that were not consciously perceived but simply guessed correctly.

Grand average evoked potential at Cz-M1M2 for stimuli acquired during both procedures. Significance with respect to baseline (p < .05) is indicated by a solid line, while insignificant parts are indicated by dotted lines. Latencies with a significant contrast (p < .05) between detected and non-detected (in go/go-no (GN) procedure) and between correct and incorrect (in two-interval forced choice (2IFC) procedure) are marked with a black bar
Grand average evoked potentials at Cz-M1M2 for several levels of detection probability are displayed in Fig. 6. There was a significant effect of detection probability on the evoked potential during both procedures and for both stimulus types. While the average evoked potential during a GN procedure appears graded with stimulus intensity, the average evoked potential during a 2IFC procedure remains low until high levels of detection probability are reached, i.e. a detection probability larger than 0.875. Both phenomena are more clearly visible in Fig. 7, where the average amplitude of the major positive peak between 380 and 420 ms, the P2, is displayed. Here, the average P2 appears to increase almost proportional with respect to detection probability during the GN procedure. Note that this proportional increase with detection probability can be attributed to two phenomena: (1) The average P2 for detected stimuli is at almost every point significantly larger than the average P2 amplitude for non-detected stimuli, leading to an increased average P2 over all stimuli when more stimuli are detected, and (2) there is an increasing trend in the average P2 for both detected and non-detected stimuli, leading to a further increase in the average P2 over all stimuli with respect to detection probability. Similar to the previous figure, the average P2 during the 2IFC procedure remains low until a probability larger than 0.875 is reached.

Grand average evoked potential at Cz-M1M2 for stimuli acquired during both procedures at four levels of detection probability. Latencies with a significant effect of detection probability (p < .05) are marked with a black bar

Average amplitude of P2 peak in the evoked potential (and 95% confidence interval) with respect to detection probability. There is an almost proportional relation between the average P2 amplitude and detection probability. Average P2 amplitude is significantly larger for detected stimuli in comparison with non-detected stimuli, and shows an increasing trend with respect to detection probability for both detected and non-detected stimuli. In the two-interval forced choice (2IFC) procedure, the average P2 amplitude remains at very low levels (comparable with or even lower than non-detected stimuli) until a high detection probability (> 0.8 for go/no-go (GN) and > 0.9 for 2IFC) is reached
Discussion
In this study, we observed nociceptive detection thresholds, psychometric slopes, and central evoked potentials obtained during a GN and a 2IFC detection procedure. The differences observed between both procedures in nociceptive detection threshold and in evoked responses include important clues about how nociceptive detection might work, and how the threshold obtained during these procedures can be interpreted.
The first objective of this study was to determine if the nociceptive detection threshold during a GN procedure is biased by a response criterion. We found that the detection threshold for single-pulse intra-epidermal electric stimuli is significantly higher, and the psychometric slope significantly lower, during a GN procedure in comparison with a 2IFC procedure. In addition, this difference between both procedures appears to increase as the value of the estimated threshold or slope increases. In contrast, we found that the threshold for double-pulse stimuli does not differ significantly between procedures. This result implies that for some types of stimuli the nociceptive detection threshold measured during a GN procedure reflects evoked neural activity exceeding a response criterion, rather than the presence of sensory evidence itself. Equal detection thresholds for double pulse stimuli between the GN and the 2IFC procedure indicate that the extent to which the observed detection threshold is influenced by the response criterion also depends on stimulus properties, and that the bias of the detection threshold introduced by a criterion might be lower for high signal-to-noise ratio stimuli such as the double-pulse stimulus in this experiment. In addition, a significant difference was observed between single- and double-pulse stimuli during a GN procedure, while no significant difference was observed between detection thresholds for single- and double-pulse stimuli during a 2IFC procedure. Although a small difference between the single- and double-pulse threshold might go unnoticed due to estimation errors, it is clear that the large difference between both stimulus types in a GN procedure almost completely disappears during 2IFC. The reason for this discrepancy between the two tasks remains unclear without more sophisticated psychophysical modeling, which is out of the scope of this study. However, these results warrant the development of novel psychophysical models that are tailored to the process of nociception in future studies. One of the potential factors that might help to explain such a difference would be the presence of spontaneous neural activity influencing both the response criterion and psychometric slope of the participant. More importantly, formulation of psychophysical models that are connected to neurophysiological mechanisms can lead to more insight in the interpretation of the detection thresholds measured in a clinical or research setting.
The second objective of this study was to determine if the presence of a response criterion is reflected in the nociceptive evoked potentials observed in response to stimuli around the detection threshold. We measured a significant central evoked response at Cz-M1M2 during both procedures for detected stimuli (GN) and correctly reported trials (2IFC). We also measured a significant evoked response to non-detected stimuli (GN), which was absent for incorrectly reported trials (2IFC). We found that the evoked P2 response is proportionally graded with detection probability during a GN procedure. At the same time, we observed that the P2 response during a 2IFC procedure for stimuli with the same detection probability (corrected for guessing rate), remains low until a large detection probability is reached. The P2 response to detected and non-detected stimuli show that we might be looking at a mostly dichotomous response, where the response is much larger for detected stimuli than for non-detected stimuli. The visual evoked P3 response is considered a key marker of conscious access to sensory evidence (Rutiku et al., 2015; Salti et al., 2012), and the high degree of overlap in activated brain regions suggests a similar functional significance of the nociceptive P2 (Iannetti & Mouraux, 2010; Mouraux & Iannetti, 2009). Our observation that the P2 shows an on-off behavior with respect to reported conscious perception is in accordance with this theory.
Assuming that we are looking at an entirely dichotomous response, we can explore how the detection probability in both procedures relates to the stimulus amplitude and the associated probability of evoking a central brain response at Cz-M1M2. Figure 8 shows that the difference between detection probability and evoked response probability determines the observed pattern of the average P2 response in Fig. 7. When there is no difference between the detection threshold and the threshold for evoking a brain response at 0.5 probability, both curves will overlap leading to a proportional relation between the evoked response probability (or average P2) and the detection probability, as we observed for the GN procedure. When the detection threshold is lower than the threshold for evoking a brain response, we expect a bended curve which predicts that the evoked response probability (or average P2) remains low until a high detection probability is reached, as we observed for the 2IFC procedure. As such, our results suggest that the evoked response probability is equal to the detection probability in the GN procedure, but lower than the detection probability in the 2IFC procedure, implying that the probability of evoked a P2 response was approximately equal to the probability of a stimulus being detected in the GN procedure. Our data indicate that the P2 might be modulated by both conscious stimulus detection and detection probability; however, the effect of stimulus detection appeared to be much larger. If we interpret this increase of the P2 with respect to stimulus detection as a marker for conscious access to sensory evidence, the response criterion observed in this experiment could be interpreted as a perceptual criterion, i.e., only stimuli above this criterion are perceived. This also implies that the average P2 responses observed during a GN procedure are affected by a response criterion just like the participant responses themselves, when they are not corrected for stimulus detection.

The difference between detection probability and evoked response probability determines the relation between detection probability and average evoked response
These observations show that when the nociceptive detection threshold is assessed using a GN procedure, one might observe the effect of an adjusted perceptual criterion rather than altered nociceptive processing following an intervention. This has important consequences for studies using nociceptive detection thresholds to assess altered central and peripheral nociceptive processing. The mechanical and thermal detection threshold are increased in patients with neuropathic pain and signs of central sensitization (Maier et al., 2010). Thermal heat and cold detection thresholds show a high sensitivity to potential peripheral nerve damage by diabetes (Courtin et al., 2020) as well as painfulness in diabetic neuropathies (Krämer et al., 2004). Intra-epidermal electric detection thresholds are increased following deafferentiation by capsaicin (Doll, van Amerongen, et al., 2016b) and following diabetic neuropathy (Suzuki et al., 2016). Our current results emphasize that these nociceptive detection thresholds can in some cases reflect a central criterion that determines if the stimulus is consciously perceived, rather than the threshold for activation of the nociceptive system itself. This criterion does not only affect participant report, but also the central P2 response, which appeared to be generated only when the stimulus was reported as consciously perceived, i.e., when the stimulus exceeded a perceptual criterion. The notion that we can measure the potential influence of a perceptual criterion by comparing detection thresholds in GN and 2IFC procedures opens up new avenues of research into the role of perception in nociceptive processing and (chronic) pain.
References
Bland, J. M., & Altman, D. G. (1986). Statistical methods for assessing agreement between two methods of clinical measurement. Lancet, 1(8476), 307–310.
Coleman, T. F., & Li, Y. (1996). An Interior Trust Region Approach for Nonlinear Minimization Subject to Bounds. SIAM Journal on Optimization, 6(2), 418–445. https://doi.org/10.1137/0806023
Courtin, A. S., Maldonado Slootjes, S., Caty, G., Hermans, M. P., Plaghki, L., & Mouraux, A. (2020). Assessing thermal sensitivity using transient heat and cold stimuli combined with a Bayesian adaptive method in a clinical setting: A proof of concept study. European Journal of Pain, 24(9), 1812–1821. https://doi.org/10.1002/ejp.1628
Delorme, A., Sejnowski, T., & Makeig, S. (2007). Enhanced detection of artifacts in EEG data using higher-order statistics and independent component analysis. NeuroImage, 34(4), 1443–1449. https://doi.org/10.1016/j.neuroimage.2006.11.004
Doll, R. J., Maten, A. C. A., Spaan, S. P. G., Veltink, P. H., & Buitenweg, J. R. (2016a). Effect of temporal stimulus properties on the nociceptive detection probability using intra-epidermal electrical stimulation. Experimental Brain Research, 234(1), 219–227. https://doi.org/10.1007/s00221-015-4451-1
Doll, R. J., van Amerongen, G., Hay, J. L., Groeneveld, G. J., Veltink, P. H., & Buitenweg, J. R. (2016b). Responsiveness of electrical nociceptive detection thresholds to capsaicin (8 %)-induced changes in nociceptive processing. Experimental Brain Research, 234(9), 2505–2514. https://doi.org/10.1007/s00221-016-4655-z
Doll, R. J., Veltink, P. H., & Buitenweg, J. R. (2015). Observation of time-dependent psychophysical functions and accounting for threshold drifts. Attention, Perception, and Psychophysics, 77(4), 1440–1447. https://doi.org/10.3758/s13414-015-0865-x
Georgeson, M. (2012). Sensory, perceptual and response biases: the criterion concept in perception. Journal of Vision, 12(9), 1392–1392. https://doi.org/10.1167/12.9.1392
Hochberg, Y., & Benjamini, Y. (1995). Controlling the false discovery rate: A Practical and powerful approach to multiple testing. J.Roy.Statist.Soc., 57, 289–300. https://doi.org/10.1111/j.2517-6161.1995.tb02031.x
Iannetti, G. D., & Mouraux, A. (2010). From the neuromatrix to the pain matrix (and back). Experimental Brain Research, 205(1), 1–12. https://doi.org/10.1007/s00221-010-2340-1
Kingdom, F. A. A., & Prins, N. (2016). Chapter 6 - Signal Detection Measures∗. In F. A. A. Kingdom & N. Prins (Eds.), Psychophysics (Second ed., pp. 149–188). Academic Press.
Krämer, H. H., Rolke, R., Bickel, A., & Birklein, F. (2004). Thermal thresholds predict painfulness of diabetic neuropathies. Diabetes Care, 27(10), 2386–2391. https://doi.org/10.2337/diacare.27.10.2386
Legrain, V., Guérit, J. M., Bruyer, R., & Plaghki, L. (2002). Attentional modulation of the nociceptive processing into the human brain: Selective spatial attention, probability of stimulus occurrence, and target detection effects on laser evoked potentials. Pain, 99(1-2), 21–39. https://doi.org/10.1016/S0304-3959(02)00051-9
Legrain, V., Iannetti, G. D., Plaghki, L., & Mouraux, A. (2011). The pain matrix reloaded: A salience detection system for the body. Progress in Neurobiology, 93(1), 111–124. https://doi.org/10.1016/j.pneurobio.2010.10.005
Maier, C., Baron, R., Tölle, T. R., Binder, A., Birbaumer, N., Birklein, F., . . . Treede, D. R. (2010). Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): somatosensory abnormalities in 1236 patients with different neuropathic pain syndromes. Pain, 150(3), 439-450. https://doi.org/10.1016/j.pain.2010.05.002
Maris, E., & Oostenveld, R. (2007). Nonparametric statistical testing of EEG- and MEG-data. Journal of Neuroscience Methods, 164(1), 177–190. https://doi.org/10.1016/j.jneumeth.2007.03.024
Mouraux, A., & Iannetti, G. D. (2009). Nociceptive Laser-Evoked Brain Potentials Do Not Reflect Nociceptive-Specific Neural Activity. Journal of Neurophysiology, 101(6), 3258–3269. https://doi.org/10.1152/jn.91181.2008
Mouraux, A., & Iannetti, G. D. (2018). The search for pain biomarkers in the human brain. Brain, 141(12), 3290–3307. https://doi.org/10.1093/brain/awy281
Mouraux, A., Iannetti, G. D., & Plaghki, L. (2010). Low intensity intra-epidermal electrical stimulation can activate Aδ-nociceptors selectively. Pain, 150(1), 199–207. https://doi.org/10.1016/j.pain.2010.04.026
Mouraux, A., Marot, E., & Legrain, V. (2014). Short trains of intra-epidermal electrical stimulation to elicit reliable behavioral and electrophysiological responses to the selective activation of nociceptors in humans. Neuroscience Letters, 561(Supplement C), 69–73. https://doi.org/10.1016/j.neulet.2013.12.017
Oostenveld, R., Fries, P., Maris, E., & Schoffelen, J. M. (2011). FieldTrip: Open source software for advanced analysis of MEG, EEG, and invasive electrophysiological data. Computational Intelligence and Neuroscience, 2011. https://doi.org/10.1155/2011/156869
Picton, T. W. (1992). The P300 wave of the human event-related potential. Journal of Clinical Neurophysiology, 9(4), 456–479. https://doi.org/10.1097/00004691-199210000-00002
Poulsen, A. H., Tigerholm, J., Meijs, S., Andersen, O. K., & Mørch, C. D. (2020). Comparison of existing electrode designs for preferential activation of cutaneous nociceptors. Journal of Neural Engineering. https://doi.org/10.1088/1741-2552/ab85b1
Rutiku, R., Martin, M., Bachmann, T., & Aru, J. (2015). Does the P300 reflect conscious perception or its consequences? Neuroscience, 298, 180–189. https://doi.org/10.1016/j.neuroscience.2015.04.029
Salti, M., Bar-Haim, Y., & Lamy, D. (2012). The P3 component of the ERP reflects conscious perception, not confidence. Conscious Cogn, 21(2), 961–968. https://doi.org/10.1016/j.concog.2012.01.012
Steenbergen, P., Buitenweg, J. R., Trojan, J., van der Heide, E. M., van den Heuvel, T., Flor, H., & Veltink, P. H. (2012). A system for inducing concurrent tactile and nociceptive sensations at the same site using electrocutaneous stimulation. Behavior Research Methods, 44(4), 924–933. https://doi.org/10.3758/s13428-012-0216-y
Suzuki, C., Kon, T., Funamizu, Y., Ueno, T., Haga, R., Nishijima, H., . . . Baba, M. (2016). Elevated pain threshold in patients with asymptomatic diabetic neuropathy: an intraepidermal electrical stimulation study. Muscle Nerve, 54(1), 146-149. https://doi.org/10.1002/mus.25158
Ugray, Z., Lasdon, L., Plummer, J., Glover, F., Kelly, J., & Martí, R. (2007). Scatter Search and Local NLP Solvers: A Multistart Framework for Global Optimization. INFORMS Journal on Computing, 19(3), 328–340. https://doi.org/10.1287/ijoc.1060.0175
van den Berg, B., & Buitenweg, J. R. (2021). Observation of Nociceptive Processing: Effect of Intra-Epidermal Electric Stimulus Properties on Detection Probability and Evoked Potentials. Brain Topography. https://doi.org/10.1007/s10548-020-00816-y
van den Berg, B., Doll, R. J., Mentink, A. L. H., Siebenga, P. S., Groeneveld, G. J., & Buitenweg, J. R. (2020). Simultaneous tracking of psychophysical detection thresholds and evoked potentials to study nociceptive processing. Behavior Research Methods. https://doi.org/10.3758/s13428-019-01338-7
van den Broeke, E. N., Mouraux, A., Groneberg, A. H., Pfau, D. B., Treede, R.-D., & Klein, T. (2015). Characterizing pinprick-evoked brain potentials before and after experimentally induced secondary hyperalgesia. Journal of Neurophysiology, 114(5), 2672–2681. https://doi.org/10.1152/jn.00444.2015
Wager, T. D., Matre, D., & Casey, K. L. (2006). Placebo effects in laser-evoked pain potentials. Brain, Behavior, and Immunity, 20(3), 219–230. https://doi.org/10.1016/j.bbi.2006.01.007
Availability of data and materials
Data of the experiments reported here are available on request from the corresponding author.
Code availability
Codes required to perform the analyses reported here are available on request from the corresponding author.
Funding
This study was funded by the Dutch Research Council (NWO) through the NeuroCIMT research program (P14-12, project 2).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethics approval
All experiments were approved by the research ethics committee of the faculty of Electrical Engineering, Mathematics and Computer Science at the University of Twente (nr. RP 2021-05). All experiments were carried out in accordance with the 1964 Declaration of Helsinki and its later amendments.
Consent to participate
All participants provided written informed consent and were rewarded for participation in the experiment.
Consent for publication
All authors approved the final manuscript and agreed with submission to Attention, Perception & Psychophysics.
Additional information
Open practices statement
Data and code are available on request from the corresponding author. None of the experiments was preregistered.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
van den Berg, B., Vanwinsen, L., Pezzali, G. et al. Observation of nociceptive detection thresholds and cortical evoked potentials: Go/no-go versus two-interval forced choice. Atten Percept Psychophys 84, 1359–1369 (2022). https://doi.org/10.3758/s13414-022-02484-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.3758/s13414-022-02484-5