
Abstract
Background
Intraoperative examination of retro-areolar margin (IERM) often is used during nipple-sparing mastectomy (NSM) for cancer, but there is no robust data regarding its real advantage.
Methods
Consecutive patients undergoing NSM for cancer with omission of IERM according to institutional protocols from 2016 to 2021 were retrospectively analyzed. The decision to maintain or remove the Nipple-Areola Complex (NAC) after definitive pathology was taken at the multidisciplinary meeting.
Results
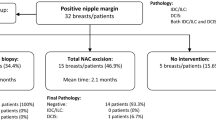
Among 162 women operated in the study period, the presence of neoplastic cells within 2 mm from the inked retroareolar margin (RAM) was detected at permanent pathology in 17 cases (10.5%). Nipple-Areola-Complex (NAC) was removed postoperatively in five patients (3%) for margins <1 mm, the other 12 were observed, whereas postoperative NAC necrosis required surgical removal in additional five cases (3%). The NAC was thus preserved in 152 of 162 patients (94%). At multivariate analysis, RAM ≤2 mm was associated with radiological tumor-to-nipple distance less than or equal to 1 cm (p = 0.04) and Ki67 label index ≥ 20 (p = 0.04), whereas multifocality/multicentricity showed a trend towards significance (p = 0.07). At a median follow-up of 46 months, five locoregional relapses occurred (3%), only one of them involving the NAC (0, 6%). Locoregional relapse and overall survival for patients with RAM > or < 2 mm were not different.
Conclusions
IERM is not routinely necessary during NSM for cancer, because its omission is associated with a very low return to the operating room, it is oncologically safe, and associated pitfalls are avoided. Further studies are necessary to confirm these findings.


Similar content being viewed by others


References
Elmore LC, Dietz JR, Myckatyn TM, Margenthaler JA. The landmark series: mastectomy trials (skin-sparing and nipple-sparing and reconstruction landmark trials). Ann Surg Oncol. 2021;28:273–80.
Benediktsson KP, Perbeck L. Survival in breast cancer after nipple-sparing subcutaneous mastectomy and immediate reconstruction with implants: a prospective trial with 13 years median follow-up in 216 patients. Eur J Surg Oncol. 2008;34(2):143–8.
Sakurai T, Zhang N, Suzuma T, et al. Long-term follow-up of nipple-sparing mastectomy without radiotherapy: a single center study at a Japanese institution. Med Oncol. 2013;30(1):481.
Lanitis S, Tekkis PP, Sgourakis G, et al. Comparison of skin-sparing mastectomy versus non-skin-sparing mastectomy for breast cancer: A meta-analysis of observational studies. Ann Surg Oncol. 2010;251:632–9.
Galimberti V, Morigi C, Bagnardi V, et al. Oncological outcomes of nipple-sparing mastectomy: a single-center experience of 1989 patients. Ann Surg Oncol. 2018;25(13):3849–57.
Weber WP, Haug M, Kurzeder C, et al. Oncoplastic Breast Consortium consensus conference on nipple-sparing mastectomy. Breast Cancer Res Treat. 2018;172(3):523–7.
Gerber B, Krause A, Reimer T, et al. Skin-sparing mastectomy with conservation of the nipple-areola complex and autologous reconstruction is an oncologically safe procedure. Ann Surg. 2003;238:120–7.
Fu M, Chen Q, Zeng L, et al. Prognosis comparison between nipple-sparing mastectomy and total mastectomy in breast cancer: a case-control study after propensity score matching. Ann Surg Oncol. 2022;29(4):2221–30.
Crowe JP, Patrick RJ, Yetman RJ, Djohan R. Nipple sparing mastectomy update: one hundred forty-nine procedures and clinical outcomes. Arch Surg. 2008;143:1106–10.
Sacchini V, Pinotti JA, Barros AC, et al. Nipple sparing mastectomy for breast cancer and risk reduction: Oncologic or technical problem? J Am Coll Surg. 2006;203:704–14.
Dent BL, Chao JW, Eden DJ, et al. Nipple resection and reconstruction after attempted nipple-sparing mastectomy. Ann Plast Surg. 2017;78:28–34.
Cho J, Chung J, Cha ES, Lee JE, Kim JH. Can preoperative 3-T MRI predict nipple-areolar complex involvement in patients with breast cancer? Clin Imag. 2016;40:119–24.
Brachtel EF, Rusby J, Michaelson J, et al. Occult nipple involvement in breast cancer: clinicopathologic findings in 316 consecutive mastectomy specimens. J Clin Oncol. 2009;27(30):4948–54.
Santini D, Taffurelli M, Gelli MC, et al. Neoplastic involvement of nipple-areolar complex in invasive breast cancer. Am J Surg. 1989;158:399–403.
Vyas JJ, Chinoy RF, Vaidya JS. Prediction of nipple and areolar involvement in breast cancer. Eur J Surg Oncol. 1998;24:15–6.
Li W, Wang S, Guo X, et al. Nipple involvement in breast cancer: retrospective analysis of 2323 consecutive mastectomy specimens. Int J Surg Pathol. 2011;19:328–34.
Fregatti P, Gipponi M, Zoppoli G, et al. Tumor-to-nipple distance should not preclude nipple-sparing mastectomy in breast cancer patients. Personal experience and literature review. Anticancer Res. 2020;40:3543–50.
Laronga C, Kemp B, Johnston D, Robb GL, Singletary SE. The incidence of occult nipple-areola complex involvement in breast cancer patients receiving a skin-sparing mastectomy. Ann Surg Oncol. 1999;6:609–13.
Brachtel EF, Rusby JE, Michaelson JS, Muzikansky A, Smith BL, Koerner FC. Occult nipple involvement in breast cancer: clinicopathologic findings in 316 consecutive mastectomy specimens. J Clin Oncol. 2009;27:4948–54.
Headon HL, Kasem A, Mokbel K. The oncological safety of nipple-sparing mastectomy: a systematic review of the literature with a pooled analysis of 12,358 procedures. Arch Plast Surg. 2016;43:328–38.
De la Cruz L, Moody MA, Tappy EE, Blankenship SA, Hecht EM. Overall survival, disease-free survival, local recurrence, and nipple-areolar recurrence in the setting of nipple-sparing mastectomy: a meta-analysis and systematic review. Ann Surg Oncol. 2015;22:3241–9.
Agha RA, Al Omran Y, Wellstead G, et al. Systematic review of therapeutic nipple-sparing versus skin-sparing mastectomy. BJS Open. 2018;3:135–45.
Wu ZY, Kim HJ, Lee JW, et al. Breast cancer recurrence in the nipple-areola complex after nipple-sparing mastectomy with immediate breast reconstruction for invasive breast cancer. JAMA Surg. 2019;154:1030–7.
Heinzen RN, Dornellas de Barros ACS, Carvalho FM, et al. Nipple-sparing mastectomy for early breast cancer: the importance of intraoperative evaluation of retroareolar margins and intra-nipple duct removal. Gland Surg. 2020;9:637–46.
De Alcantara FP, Capko D, Barry JM, et al. Nipple-sparing mastectomy for breast cancer and risk-reducing surgery: the memorial Sloan-Kettering cancer Center experience. Ann Surg Oncol. 2011;18:3117–22.
Luo D, Ha J, Latham B, et al. The accuracy of intraoperative subareolar frozen section in nipple-sparing mastectomies. Ochsner J. 2010;10:188–92.
Morales Piato JR, Aguiar FN, Mota BS, et al. Improved frozen section examination of the retroareolar margin for prediction of nipple involvement in breast cancer. Eur J Surg Oncol. 2015;41:986–90.
Alperovich M, Choi M, Karp NS, et al. Nipple-sparing mastectomy and sub-areolar biopsy: To freeze or not to freeze? Evaluation the role of sub-areolar intraoperative frozen section. Breast J. 2016;22:18–23.
Lucy X, Aya Y, Michaels PS. Ginter: Subareolar tissue biopsy predicts occult nipple involvement in nipple-sparing mastectomies. Am J Clin Pathol. 2022;157:266–72.
Garcia MT, Mota BS, Cardoso N, et al. Accuracy of frozen section in intraoperative margin assessment for breast-conserving surgery: a systematic review and meta-analysis. Plos One. 2021;16:e0248768. https://doi.org/10.1371/journal.pone.0248768.
Rayna C, DeSnyder SM. Intraoperative assessment in breast cancer management. Surg Oncol Clin N Am. 2018;27:155–65.
Margenthaler JA, Gao F, Kimberg VS. Margin index: a new method for prediction of residual disease after breast-conserving surgery. Ann Surg Oncol. 2010;17:2696–701.
Landercasper J, Bogert A, Fayanju O, et al. Factors associated with reoperation in breast-conserving surgery for cancer: a prospective study of American Society of Breast Surgeon members. Ann Surg Oncol. 2019;26:3321–36.
Fortunato L, Loreti A, Andrich A, et al. When mastectomy is needed: Is the nipple-sparing procedure a new standard with very few contraindications? J Surg Oncol. 2013;108:207–12. https://doi.org/10.1002/jso.23390.
https://www.breastcentrescertification.com/breastcentrescert.php.
Zarba Meli E, Cattin F, Curcio A, et al. Surgical delay may extend the indications for nipple-sparing mastectomy: a multicentric study. Eur J Surg Oncol. 2019;45:1373–7.
Jensen JA, Lin JH, Kapoor N, et al. Surgical delay of the nipple-areolar complex: a powerful technique to maximize nipple viability following nipple-sparing mastectomy. Ann Surg Oncol. 2012;19:3171–6.
Zarba Meli E, De Santis A, Cortese G, et al. Nipple-sparing mastectomy after neoadjuvant chemotherapy: definitive results with a long-term follow-up evaluation. Ann Surg Oncol. 2023. https://doi.org/10.1245/s10434-022-13035-5.
Giuliano AE, Edge SB, Hortobagyi GN. Eighth edition of the AJCC cancer staging manual: breast cancer. Ann Surg Oncol. 2018;25:1783–5. https://doi.org/10.1245/s10434-018-6486-6.
Daar DA, Abdou SA, Rosario L, et al. Is there a preferred incision location for nipple-sparing mastectomy? A systematic review and meta-analysis. Plast Reconstr Surg. 2019;143:906e-e919.
Park S, Yoon C, Bae SJ, et al. Comparison of complications according to incision types in nipple-sparing mastectomy and immediate reconstruction. Breast. 2020;53:85–91.
Peled AW, Foster RD, Stover AC, et al. Outcomes after total skin-sparing mastectomy and immediate reconstruction in 657 breasts. Ann Surg Oncol. 2012;19:3402–9.
Amara D, Peled AW, Wang F, et al. Tumor involvement of the nipple in total skin-sparing mastectomy: strategies for management. Ann Surg Oncol. 2015;12:3803–8.
Hogan KO, Lai SM, Wagner JL, Fan F. The utility of intraoperative retroareolar margin frozen section assessment and the management of atypical epithelial proliferative lesions at the retroareolar margin in nipple-sparing mastectomies. Ann Diagn Pathol. 2021;51:151697.
D’Alonzo M, Pecchio S, Campisi P, et al. Nipple-sparing mastectomy: reliability of sub-areolar sampling and frozen section in predicting occult nipple involvement in breast cancer patients. EJSO. 2018;44:1736–42. https://doi.org/10.1016/j.ejso.2018.07.059.
Duarte GM, Tomazini MV, Oliveira A, et al. Accuracy of frozen section, imprint cytology, and permanent histology of sub-nipple tissue for predicting occult nipple involvement in patients with breast carcinoma. Breast Cancer Res Treat. 2015;153:557–63.
Coopey SB, Smith BL. The nipple is just another margin. Ann Surg Oncol. 2015;22:3764–6.
Mitchell SD, Willey SC, Beitsch P, Feldman S. Evidence outcomes of the American society of breast surgeons nipple-sparing mastectomy registry. Gland Surg. 2018;7:247–57.
Haslinger ML, Sosin M, Bartholomew AL, et al. Positive nipple margin after nipple-sparing mastectomy: an alternative and oncologically safe approach to preserving the nipple-areolar complex. Ann Surg Oncol. 2018;25:2303–7.
Eichler C, Stephan S, Thangarajan F, et al. Intraoperative central nipple biopsy in nipple-sparing mastectomy: a retrospective analysis of 211 patients. Breast J. 2021;27:363–8.
Eisenberg REK, Chan JSY, Swistel AJ, Hoda SA. Pathological evaluation of nipple-sparing mastectomies with emphasis on occult nipple involvement: the Weill-Cornell experience with 325 cases. Breast. 2014;20:15–21.
Petit JY, Veronesi U, Orecchia R, et al. Risk factors associated with recurrence after nipple-sparing mastectomy for invasive and intraepithelial neoplasia. Ann Oncol. 2012;23:2053–8.
Kneubil MC, Lohsiriwat V, Curigliano G, et al. Risk of locoregional recurrence in patients with false-negative frozen section or close margins of retroareolar specimen in nipple-sparing mastectomy. Ann Surg Oncol. 2012;19:4117–23.
D’Alonzo M, Martincich L, Biglia N, et al. Clinical and radiological predictors of nipple-areola complex involvement in breast cancer patients. EJC. 2012;48:2311–8.
D’Alonzo M, Martincich L, Fenoglio A, et al. Nipple-sparing mastectomy: external validation of a three-dimensional automated method to predict nipple occult tumor involvement on preoperative breast MRI. Eur Radiol Exp. 2019;3:31.
Ponzone R, Maggiorotto F, Carabalona S, Rivolin A, et al. MRI and intraoperative pathology to predict nipple-areola complex (NAC) involvement in patients undergoing NAC-sparing mastectomy. Eur J Cancer. 2015;51:1882–9.
Acknowledgment
This work was supported by Fondazione Prometeus, ONLUS, for the development of research and training in oncology. The authors thank Marcia Adams for English assistance in the preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
No potential conflict of interest to be reported.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Serio, F., Manna, E., La Pinta, M. et al. Intraoperative Examination of Retro-Areolar Margin is not Routinely Necessary During Nipple-Sparing Mastectomy for Cancer. Ann Surg Oncol 30, 6488–6496 (2023). https://doi.org/10.1245/s10434-023-13726-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-023-13726-7