
Abstract
Background
For the 6% of breast cancer patients with a diagnosis of stage IV disease, systemic therapy is the cornerstone of treatment, with an unclear role for surgery. Limited evidence exists to delineate treatment methods with regard to hormone receptor and human epidermal growth factor receptor 2 (HER2) status.
Methods
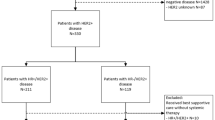
The National Cancer Database was used to identify 12,838 stage IV breast cancer patients with known hormone receptor and HER2 status from 2010 to 2015. Chi square tests examined subgroup differences between the treatment methods received. Using the Kaplan–Meier method, 5-year overall survival (OS) was assessed. Multivariate Cox proportional hazard models examined factors associated with survival.
Results
A survival advantage was noted for patients who received either systemic therapy and surgery (ST + Surg: hazard ratio [HR] 0.723; 95% confidence interval [CI] 0.671–0.779) or systemic therapy, surgery, and radiation (Trimodality: HR 0.640; 95% CI 0.591–0.694) (both p < 0.0001) compared with systemic therapy alone (ST). The HER2+ patients who received Trimodality or ST + Surg had a better 5-year OS rate than those who received ST (Trimodality [48%], ST + Surg [41%], ST [29%]; p < 0.0001). The sequence of chemotherapy in relation to surgery is significant, with the greatest survival advantage noted for recipients of neoadjuvant chemotherapy (NAC) compared with patients who had adjuvant chemotherapy when they had positive hormone receptor and HER2 status (HER2 + NAC: HR 0.477; estrogen receptor-positive [ER+] NAC: HR 0.453; progesterone receptor-positive [PR+] NAC: HR 0.448; all p < 0.0001).
Conclusions
Surgery in addition to ST has a survival benefit for stage IV breast cancer patients with known hormone receptor and HER2 status and should be considered after NAC for patients with ER+, PR+, or HER2+ disease.



Similar content being viewed by others


References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7–34.
Chia SK, Speers CH, D’Yachkova Y, et al. The impact of new chemotherapeutic and hormone agents on survival in a population-based cohort of women with metastatic breast cancer. Cancer. 2007;110:973–9.
Beslija S, Bonneterre J, Burstein HJ, et al. Third consensus on medical treatment of metastatic breast cancer. Ann Oncol. 2009;20:1771–85.
Khan SA, Stewart AK, Morrow M. Does aggressive local therapy improve survival in metastatic breast cancer? Surgery. 2002;132:620–6; discussion 626–7.
Fitzal F, Bjelic-Radisic V, Knauer M, et al. Impact of breast surgery in primary metastasized breast cancer: outcomes of the prospective randomized phase III ABCSG-28 POSYTIVE trial. Ann Surg. 2019;269:1163–9.
Badwe R, Hawaldar R, Nair N, et al. Locoregional treatment versus no treatment of the primary tumour in metastatic breast cancer: an open-label randomised controlled trial. Lancet Oncol. 2015;16:1380–8.
Li X, Huang R, Ma L, Liu S, Zong X. Locoregional surgical treatment improves the prognosis in primary metastatic breast cancer patients with a single distant metastasis except for brain metastasis. Breast. 2019;45:104–12.
Harris E, Barry M, Kell MR. Meta-analysis to determine if surgical resection of the primary tumour in the setting of stage IV breast cancer impacts on survival. Ann Surg Oncol. 2013;20:2828–34.
Headon H, Wazir U, Kasem A, Mokbel K. Surgical treatment of the primary tumour improves the overall survival in patients with metastatic breast cancer: a systematic review and meta-analysis. Mol Clin Oncol. 2016;4:863–7.
Petrelli F, Barni S. Surgery of primary tumors in stage IV breast cancer: an updated meta-analysis of published studies with meta-regression. Med Oncol. 2012;29:3282–90.
Xiao W, Zou Y, Zheng S, et al. Primary tumor resection in stage IV breast cancer: A systematic review and meta-analysis. Eur J Surg Oncol. 2018;44:1504–12.
Neuman HB, Morrogh M, Gonen M, Van Zee KJ, Morrow M, King TA. Stage IV breast cancer in the era of targeted therapy: Does surgery of the primary tumor matter? Cancer. 2010;116:1226–33.
Gnerlich J, Jeffe DB, Deshpande AD, Beers C, Zander C, Margenthaler JA. Surgical removal of the primary tumor increases overall survival in patients with metastatic breast cancer: Analysis of the 1988–2003 SEER data. Ann Surg Oncol. 2007;14:2187–94.
Gradishar WJ, Anderson BO, Balassanian R, et al. Invasive breast cancer version 1. 2016, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2016;14:324–54.
Boffa DJ, Rosen JE, Mallin K, et al. Using the National Cancer Database for outcomes research: A review. JAMA Oncol. 2017;3:1722–8.
Teshome M. Role of operative management in stage IV breast cancer. Surg Clin North Am. 2018;98:859–68.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45:613–9.
Mudgway R, Chavez de Paz Villanueva C, Lin AC, Senthil M, Garberoglio CA, Lum SS. The impact of primary tumor surgery on survival in HER2-positive stage IV breast cancer patients in the current era of targeted therapy. Ann Surg Oncol. 2020;27(8):2711–20.
Dawood S, Broglio K, Buzdar AU, Hortobagyi GN, Giordano SH. Prognosis of women with metastatic breast cancer by HER2 status and trastuzumab treatment: an institutional-based review. J Clin Oncol. 2010;28:92–8.
Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344:783–92.
Swain SM, Miles D, Kim SB, et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): end-of-study results from a double-blind, randomised, placebo-controlled, phase 3 study. Lancet Oncol. 2020;21:519–30.
Babiera GV, Rao R, Feng L, et al. Effect of primary tumor extirpation in breast cancer patients who present with stage IV disease and an intact primary tumor. Ann Surg Oncol. 2006;13:776–82.
Siebenhüner AR, Güller U, Warschkow R. Population-based SEER analysis of survival in colorectal cancer patients with or without resection of lung and liver metastases. BMC Cancer. 2020;20:246.
Demaria S, Golden EB, Formenti SC. Role of local radiation therapy in cancer immunotherapy. JAMA Oncol. 2015;1:1325–32.
Danna EA, Sinha P, Gilbert M, Clements VK, Pulaski BA, Ostrand-Rosenberg S. Surgical removal of primary tumor reverses tumor-induced immunosuppression despite the presence of metastatic disease. Cancer Res. 2004;64:2205–11.
Rao R, Feng L, Kuerer HM, et al. Timing of surgical intervention for the intact primary in stage IV breast cancer patients. Ann Surg Oncol. 2008;15:1696–702.
Lane WO, Thomas SM, Blitzblau RC, et al. Surgical resection of the primary tumor in women with de novo stage IV breast cancer: contemporary practice patterns and survival analysis. Ann Surg. 2019;269:537–44.
Miller KD, Nogueira L, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin. 2019;69:363–85.
Eastern Cooperative Oncology Group. Early surgery or standard palliative therapy in treating patients with stage IV breast cancer. U.S. National Library of Medicine. Published 2019. Updated 2 January 2019. Retrieved 19 August 2020 at https://clinicaltrials.gov/ct2/show/NCT01242800?id=NCT01242800&draw=2&rank=1&load=cart.
ECOG-ACRIN Cancer Research Group. Surgery and radiation do not extend survival in newly diagnosed metastatic breast cancer. Published 2020. Retrieved 10 August 2020 at https://ecog-acrin.org/news-and-info/press-releases/surgery-and-radiation-did-not-extend-survival-in-newly-diagnosed-metastatic-breast-cancer.
King TA, Lyman J, Gonen M, et al. A prospective analysis of surgery and survival in stage IV breast cancer (TBCRC 013). J Clin Oncol. 2016;34(15 Suppl):1006.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1
Breast cancer histology, international classification of disease for oncology manual 3 specific codes.
Appendix 2
Inclusion and exclusion criteria.

Rights and permissions
About this article

Cite this article
Stahl, K., Wong, W., Dodge, D. et al. Benefits of Surgical Treatment of Stage IV Breast Cancer for Patients With Known Hormone Receptor and HER2 Status. Ann Surg Oncol 28, 2646–2658 (2021). https://doi.org/10.1245/s10434-020-09244-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-020-09244-5