
Abstract
Purpose
A meta-analysis of 22 randomized trials accrued from 1964 to 1986 demonstrated significantly higher rates of locoregional failure (LRF) and breast-cancer mortality in women with 1–3 positive nodes without postmastectomy radiotherapy (PMRT) after mastectomy (mast.). Recent data demonstrate that PMRT reduces distant metastases (DM) in women with pN1 disease. The challenge today is whether all patients with pathologic T1-2pN1 disease have similar substantial LRF/DM risk that routinely warrants PMRT.
Methods
We reviewed patients with pT1-2N1 breast cancer treated with mast. ± adjuvant systemic therapy without PMRT from 2000 to 2013. The endpoints were LRF and DM rates, estimated by cumulative incidence method.
Results
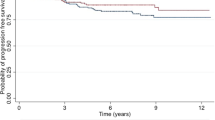
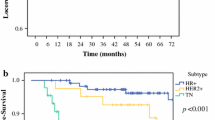
We identified 468 patients with median follow-up of 6.3 years. Most (71%) were estrogen receptor/progesterone receptor + human epidermal growth factor receptor 2 (HER2). There were 269 patients with 1+ node, 140 patients with 2+ nodes, and 59 patients with 3+ nodes. The 6-year LRF/DM rates were 4.1%/8.4%. Patients with 1+, 2+, and 3+ nodes had 6-year LRF of 2.3, 5.1 and 8.9%, respectively (p = 0.13). The 6-year DM rate was higher in patients with 3+ nodes versus 1–2+ nodes: 15.7% versus 7.4% (p = 0.02). Several subgroups had low 6-year LRF and DM rates, including T1/1+ node (0.8%/4.1% LRF/DM) and micrometastases (0%/5.8% LRF/DM).
Conclusions
Patients with pT1-2pN1 represent a heterogeneous group with a wide range of LRF/DM rates. In particular, patients with pT1 tumors and 1 + LN, and patients with micrometastases, had low event rates. These groups would derive small absolute reductions in LRF and DM with addition of PMRT, underscoring the importance of patient selection for PMRT in pT1-2pN1 breast cancer.


Similar content being viewed by others

References
McGale P, Taylor C, Correa C, et al. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet. 2014;383(9935):2127–2135.
McBride A, Allen P, Woodward W, et al. Locoregional recurrence risk for patients with T1,2 breast cancer with 1–3 positive lymph nodes treated with mastectomy and systemic treatment. Int J Radiat Oncol Biol Phys. 2014;89(2):392–398.
Miyashita M, Tada H, Suzuki A, et al. Minimal impact of postmastectomy radiation therapy on locoregional recurrence for breast cancer patients with 1 to 3 positive lymph nodes in the modern treatment era. Surg Oncol. 2017;26(2):163–170.
Moo TA, McMillan R, Lee M, et al. Selection criteria for postmastectomy radiotherapy in T1–T2 tumors with 1 to 3 positive lymph nodes. Ann Surg Oncol. 2013;20(10):3169–3174.
Poortmans PM, Collette S, Kirkove C, et al. Internal mammary and medial supraclavicular irradiation in breast cancer. N Engl J Med. 2015;373(4):317–327.
Whelan TJ, Olivotto IA, Parulekar WR, et al. Regional nodal irradiation in early-stage breast cancer. N Engl J Med. 2015;373(4):307–316.
Recht A, Comen EA, Fine RE, et al. Postmastectomy radiotherapy: an American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology focused guideline update. J Clin Oncol. 2016;34(36):4431–4442.
Clarke M, Collins R, Darby S, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;366(9503):2087–2106.
Zeidan YH, Habib JG, Ameye L, et al. Postmastectomy radiation therapy in women with T1–T2 tumors and 1 to 3 positive lymph nodes: analysis of the Breast International Group 02-98 Trial. Int J Radiat Oncol Biol Phys. 2018;101(2):316–324.
He ZY, Wu SG, Zhou J, et al. Postmastectomy radiotherapy improves disease-free survival of high risk of locoregional recurrence breast cancer patients with T1–2 and 1 to 3 positive nodes. PLoS ONE. 2015;10(3):e0119105.
Tendulkar RD, Rehman S, Shukla ME, et al. Impact of postmastectomy radiation on locoregional recurrence in breast cancer patients with 1–3 positive lymph nodes treated with modern systemic therapy. Int J Radiat Oncol Biol Phys. 2012;83(5):e577–e581.
Pan H, Gray R, Braybrooke J, et al. 20-Year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years. N Engl J Med. 2017;377(19):1836–1846.
Albain KS, Barlow WE, Shak S, et al. Prognostic and predictive value of the 21-gene recurrence score assay in postmenopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: a retrospective analysis of a randomised trial. Lancet Oncol. 2010;11(1):55–65.
Dowsett M, Cuzick J, Wale C, et al. Prediction of risk of distant recurrence using the 21-gene recurrence score in node-negative and node-positive postmenopausal patients with breast cancer treated with anastrozole or tamoxifen: a TransATAC study. J Clin Oncol. 2010;28(11):1829–1834.
Gluz O, Nitz UA, Christgen M, et al. West German Study Group Phase III PlanB Trial: first prospective outcome data for the 21-gene recurrence score assay and concordance of prognostic markers by central and local pathology assessment. J Clin Oncol. 2016;34(20):2341–2349.
Goldstein LJ, Gray R, Badve S, et al. Prognostic utility of the 21-gene assay in hormone receptor-positive operable breast cancer compared with classical clinicopathologic features. J Clin Oncol. 2008;26(25):4063–4071.
Woodward WA, Barlow WE, Jagsi R, et al. The 21-gene recurrence score and locoregional recurrence rates in patients with node-positive breast cancer treated on SWOG S8814. Int J Radiat Oncol Biol Phys. 2016;96(2):146.
Mamounas EP, Liu Q, Paik S, et al. 21-Gene recurrence score and locoregional recurrence in node-positive/ER-positive breast cancer treated with chemo-endocrine therapy. J Natl Cancer Inst. 2017. https://doi.org/10.1093/jnci/djw259.
Canadian Cancer Trials Group. 2018. https://www.ctg.queensu.ca/public/breast/breast-disease-site. Accessed 6 March 2018.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
None.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Bazan, J.G., Majithia, L., Quick, A.M. et al. Heterogeneity in Outcomes of Pathologic T1-2N1 Breast Cancer After Mastectomy: Looking Beyond Locoregional Failure Rates. Ann Surg Oncol 25, 2288–2295 (2018). https://doi.org/10.1245/s10434-018-6565-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-018-6565-8