
Abstract
Introduction
We evaluated the impact of travel distance and insurance status on contralateral prophylactic mastectomy (CPM) rates in breast cancer.
Methods
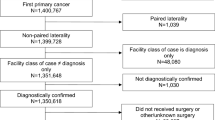
We queried the National Cancer Data Base (NCDB) for women >18 years of age with a nonmetastatic primary breast cancer of ductal, lobular, or mixed histology. Patient- and facility-specific CPM rates were calculated based on insurance, race, and distance to treatment center. Standard univariable and multivariable regression analysis was performed.
Results
Overall, the CPM rate was 6.5% for the 864,105 patients identified. Most patients traveled <20 miles to a treatment center (79.5%) and had private insurance or Medicare (58.3 and 33.4%, respectively). In general, younger, White, non-Hispanic, and privately insured patients residing further from a treatment center was associated with increased rates of CPM. However, distance to the treatment center and insurance type had a greater absolute impact on rates of CPM for Black and Hispanic patients. Absolute CPM rate increases for patients >100 miles from a treatment center compared with those <20 miles from a treatment center were observed to be greater for Black and Hispanic patients (3.5 and 3.9%, respectively) compared with White and non-Hispanic patients (2.5 and 2.6%). Additionally, further patient travel distance was associated with higher treatment center-specific CPM rates.
Conclusion
Increased travel distance is independently associated with increased rates of CPM for all patients and increased facility-specific rates of CPM. Black and Hispanic patients were found to be more vulnerable to the impact of travel distance and insurance status on rates of CPM.

Similar content being viewed by others


References
Elsayegh N, Kuerer HM, Lin H, et al. Predictors that influence contralateral prophylactic mastectomy election among women with ductal carcinoma in situ who were evaluated for BRCA genetic testing. Ann Surg Oncol. 2014;21:3466–72.
Pinell-White XA, Kolegraff K, Carlson GW. Predictors of contralateral prophylactic mastectomy and the impact on breast reconstruction. Ann Plast Surg. 2014;72:S153–7.
Abbott A, Rueth N, Pappas-Varco S, Kuntz K, Kerr E, Tuttle T. Perceptions of contralateral breast cancer: an overestimation of risk. Ann Surg Oncol. 2011;18:3129–36.
Ager B, Butow P, Jansen J, Phillips KA, Porter D, CPM DA Advisory Group. Contralateral prophylactic mastectomy (CPM): a systematic review of patient reported factors and psychological predictors influencing choice and satisfaction. Breast 2016;28:107–20.
Katz SJ, Morrow M. Contralateral prophylactic mastectomy for breast cancer: addressing peace of mind. JAMA 2013;310:793–4.
Pesce C, Liederbach E, Wang C, Lapin B, Winchester DJ, Yao K. Contralateral prophylactic mastectomy provides no survival benefit in young women with estrogen receptor-negative breast cancer. Ann Surg Oncol. 2014;21:3231–9.
Elsayegh N, Profato J, Barrera AM, et al. Predictors that influence election of contralateral prophylactic mastectomy among women with ductal carcinoma in situ who are BRCA-negative. J Cancer 2015;6:610–5.
Albornoz CR, Cohen WA, Razdan SN, et al. The impact of travel distance on breast reconstruction in the United States. Plast Reconstr Surg 2016;137:12-8.
Azzopardi J, Walsh D, Chong C, Taylor C. Surgical treatment for women with breast cancer in relation to socioeconomic and insurance status. Breast J 2014;20:3–8.
Coburn N, Fulton J, Pearlman DN, Law C, DiPaolo B, Cady B. Treatment variation by insurance status for breast cancer patients. Breast J 2008;14:128–34.
Freedman RA, Virgo KS, He Y, et al. The association of race/ethnicity, insurance status, and socioeconomic factors with breast cancer care. Cancer 2011;117:180–9.
Grimmer L, Liederbach E, Velasco J, Pesce C, Wang CH, Yao K. Variation in contralateral prophylactic mastectomy rates according to racial groups in young women with breast cancer, 1998 to 2011: a report from the National Cancer Data Base. J Am Coll Surg. 2015;221:187–96.
Goyal S, Chandwani S, Haffty BG, Demissie K. Effect of travel distance and time to radiotherapy on likelihood of receiving mastectomy. Ann Surg Oncol. 2015;22:1095–101.
Lautner M, Lin H, Shen Y, et al. Disparities in the use of breast-conserving therapy among patients with early-stage breast cancer. JAMA Surg. 2015;150:778–86.
Lin CC, Bruinooge SS, Kirkwood MK, et al. Association between geographic access to cancer care, insurance, and receipt of chemotherapy: geographic distribution of oncologists and travel distance. J Clin Oncol. 2015;33:3177–85.
Leff DR, Ho C, Thomas H, et al. A multidisciplinary team approach minimises prophylactic mastectomy rates. Eur J Surg Oncol. 2015;41:1005–12.
Acharya S, Hsieh S, Michalski JM, Shinohara ET, Perkins SM. Distance to radiation facility and treatment choice in early-stage breast cancer. Int J Radiat Oncol Biol Phys. 2016;94:691–9.
St-Jacques S, Philibert MD, Langlois A, et al. Geographic access to mammography screening centre and participation of women in the Quebec Breast Cancer Screening Programme. J Epidemiol Community Health. 2013;67:861–7.
Loree JM, Javaheri KR, Lefresne SV, et al. Impact of travel distance and urban-rural status on the multidisciplinary management of rectal cancer. J Rural Health. Epub 7 Oct 2016.
Lara PN Jr, Higdon R, Lim N, et al. Prospective evaluation of cancer clinical trial accrual patterns: identifying potential barriers to enrollment. J Clin Oncol. 2001;19:1728–33.
Disclosure
Erin P. Ward, Jonathan T. Unkart, Alex Bryant, James Murphy, and Sarah Blair deny any commercial or financial conflicts.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ward, E.P., Unkart, J.T., Bryant, A. et al. Influence of Distance to Hospital and Insurance Status on the Rates of Contralateral Prophylactic Mastectomy, a National Cancer Data Base study. Ann Surg Oncol 24, 3038–3047 (2017). https://doi.org/10.1245/s10434-017-5985-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-017-5985-1