
Abstract
Background
Recent advances in imaging and the increasing use of neoadjuvant therapy puts the contemporary utility of staging laparoscopy for patients with pancreatic adenocarcinoma (PDAC) into question. This study aimed to develop a prognostic score to optimize prevention of an unnecessary laparotomy and minimize the rate for unnecessary laparoscopy.
Methods
Clinicopathologic data were evaluated for all patients undergoing surgical intervention for PDAC between 2001 and 2015, who were stratified into group 1 (2001–2008) and group 2 (2009–2014).
Results
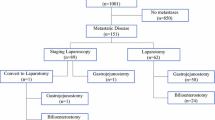
The study identified 1001 patients eligible for analysis, 331 (33%) of whom underwent a staging laparoscopy before exploration. An unnecessary laparotomy was prevented for 44.4% of the patients in period 1 and for 24% of the patients in period 2 (p < 0.001). Male gender [odds ratio (OR), 1.8; p < 0.05], preoperative resectability (borderline resectable OR 2.1; p < 0.019; locally advanced OR 7.6; p < 0.001), CA 19-9 levels higher than 394 U/L (OR 3.1; p < 0.001), no neoadjuvant chemotherapy (OR 2.7; p = 0.012), and pancreatic body or tail lesions (OR 1.8; p = 0.063) were predictive of occult metastatic disease. The developed scoring index demonstrated a c-statistic of 0.729. The observed-to-expected ratio for the index at every score level validated the index’s model. A score cutoff at 4 was able to detect 76.1% of radiographically occult metastatic disease.
Conclusion
The rate for unnecessary laparotomy among patients with PDAC has decreased in contemporary times, but unnecessary laparotomy still occurs for 1 in 4 patients. Using our scoring system, a cutoff of 4 allows 76% of radiographically occult metastases to be predicted, thereby selecting high-risk patients for laparoscopic biopsy and potentially avoiding a non-therapeutic laparotomy.



Similar content being viewed by others

References
Halpern MT, Ward EM, Pavluck AL, et al. Association of insurance status and ethnicity with cancer stage at diagnosis for 12 cancer sites: a retrospective analysis. Lancet Oncol. 2008;9:222–31.
Sener SF, Fremgen A, Menck HR, et al. Pancreatic cancer: a report of treatment and survival trends for 100,313 patients diagnosed from 1985–1995, using the National Cancer Database. J Am Coll Surg. 1999;189:1–7.
De Rosa A, Cameron IC, Gomez D. Indications for staging laparoscopy in pancreatic cancer. HPB Oxford. 2016;18:13–20.
Conlon KC, Dougherty E, Klimstra DS, et al. The value of minimal access surgery in the staging of patients with potentially resectable peripancreatic malignancy. Ann Surg. 1996;223:134–40.
Jimenez RE, Warshaw AL, Rattner DW, et al. Impact of laparoscopic staging in the treatment of pancreatic cancer. Arch Surg. 2000;135:409–14; discussion 414–5.
Warshaw AL, Tepper JE, Shipley WU. Laparoscopy in the staging and planning of therapy for pancreatic cancer. Am J Surg. 1986;151:76–80.
Stefanidis D, Grove KD, Schwesinger WH, et al. The current role of staging laparoscopy for adenocarcinoma of the pancreas: a review. Ann Oncol. 2006;17:189–99.
Liu RC, Traverso LW. Diagnostic laparoscopy improves staging of pancreatic cancer deemed locally unresectable by computed tomography. Surg Endosc. 2005;19:638–42.
Barreiro CJ, Lillemoe KD, Koniaris LG, et al. Diagnostic laparoscopy for periampullary and pancreatic cancer: what is the true benefit? J Gastrointest Surg. 2002;6:75–81.
Maithel SK, Maloney S, Winston C, et al. Preoperative CA 19-9 and the yield of staging laparoscopy in patients with radiographically resectable pancreatic adenocarcinoma. Ann Surg Oncol 2008;15:3512–20.
Pisters PW, Lee JE, Vauthey JN, et al. Laparoscopy in the staging of pancreatic cancer. Br J Surg. 2001;88:325–37.
Zamboni GA, Kruskal JB, Vollmer CM, et al. Pancreatic adenocarcinoma: value of multidetector CT angiography in preoperative evaluation. Radiology. 2007;245:770–8.
Ferrone CR, Marchegiani G, Hong TS, et al. Radiological and surgical implications of neoadjuvant treatment with FOLFIRINOX for locally advanced and borderline resectable pancreatic cancer. Ann Surg. 2015;261:12–7.
Nitsche U, Wenzel P, Siveke JT, et al. Resectability after first-line FOLFIRINOX in initially unresectable locally advanced pancreatic cancer: a single-center experience. Ann Surg Oncol. 2015;22(Suppl 3):S1212–20.
Sadot E, Doussot A, O’Reilly EM, et al. FOLFIRINOX induction therapy for stage 3 pancreatic adenocarcinoma. Ann Surg Oncol. 2015;22:3512–21.
Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–83.
Callery MP, Chang KJ, Fishman EK, et al. Pretreatment assessment of resectable and borderline resectable pancreatic cancer: expert consensus statement. Ann Surg Oncol. 2009;16:1727–33.
Easterlin MC, Chang DC, Wilson SE. A practical index to predict 30-day mortality after major amputation. Ann Vasc Surg. 2013;27:909–17.
Pierre SA, Ferrandino MN, Simmons WN, et al. High-definition laparoscopy: objective assessment of performance characteristics and comparison with standard laparoscopy. J Endourol. 2009;23:523–8.
Qin Y, Hua H, Nguyen M. Characterization and in vivo evaluation of a multi-resolution foveated laparoscope for minimally invasive surgery. Biomed Opt Express. 2014;5:2548–62.
Lemieux S, Prud’homme D, Bouchard C, et al. Sex differences in the relation of visceral adipose tissue accumulation to total body fatness. Am J Clin Nutr. 1993;58:463–7.
Grauer WO, Moss AA, Cann CE, et al. Quantification of body fat distribution in the abdomen using computed tomography. Am J Clin Nutr. 1984;39:631–7.
Meguid RA, Bronsert MR, Juarez-Colunga E, et al. Surgical Risk Preoperative Assessment System (SURPAS): II. Parsimonious risk models for postoperative adverse outcomes addressing need for laboratory variables and surgeon specialty-specific models. Ann Surg. 2016;264:10–22.
Fluss R, Faraggi D, Reiser B. Estimation of the Youden Index and its associated cutoff point. Biom J. 2005;47:458–72.
Hashimoto D, Chikamoto A, Sakata K, et al. Staging laparoscopy leads to rapid induction of chemotherapy for unresectable pancreatobiliary cancers. Asian J Endosc Surg. 2015;8:59–62.
Hoshimoto S, Hishinuma S, Shirakawa H, et al. Prognostic significance of intraoperative peritoneal washing cytology for patients with potentially resectable pancreatic ductal adenocarcinoma. Pancreatology. 2017;17:109–14.
Espat NJ, Brennan MF, Conlon KC. Patients with laparoscopically staged unresectable pancreatic adenocarcinoma do not require subsequent surgical biliary or gastric bypass. J Am Coll Surg. 1999;188:649–55; discussion 655–7.
Disclosure
All authors have no relevant disclosures.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Fong, Z.V., Alvino, D.M.L., Fernández-del Castillo, C. et al. Reappraisal of Staging Laparoscopy for Patients with Pancreatic Adenocarcinoma: A Contemporary Analysis of 1001 Patients. Ann Surg Oncol 24, 3203–3211 (2017). https://doi.org/10.1245/s10434-017-5973-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-017-5973-5