
Abstract
Background
The reported reexcision rates vary significantly for patients with invasive breast cancer undergoing breast-conserving surgery (BCS). This variability is a function of both the positive pathologic margin rate and the interpretation of an adequate pathologic margin. The influence of the SSO/ASTRO margin guidelines on reexcision rates and the potential cost savings is of interest from both quality and health economics perspectives.
Methods
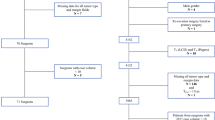
A retrospective analysis of all patients undergoing BCS during a 3-year period (January 1, 2010–December 31, 2012) was performed. The reexcision rate and the pathologic margin status were assessed to determine the number of patients with pathologic negative margins who underwent reexcision. A decision analysis using previously published case costing information was used to determine the potential savings associated with avoidance of reoperation for patients meeting guidelines criteria.
Results
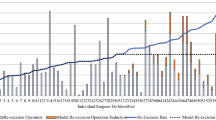
The analysis included 512 patients who underwent attempted BCS for invasive breast cancer. Reoperations occurred for 25% (126/512) of the BCS cohort, but this rate could potentially be decreased to 16% (44/512) if these guidelines were applied. Based on our cost model, application of the guidelines would provide a potential cost savings of $698 (95% confidence interval $523–$893) per patient undergoing attempted BCS in our population.
Conclusions
Adherence to the SSO-ASTRO guidelines could prevent one-third of reoperations among patients undergoing BCS. This would result in significant cost savings to the health care system while avoiding unnecessary operations. Use of guidelines has the potential to improve the quality of care provided to patients.

Similar content being viewed by others

References
Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233–41. doi:10.1056/NEJMoa022152 .
Xue DQ, Qian C, Yang L, Wang XF. Risk factors for surgical-site infections after breast surgery: a systematic review and meta-analysis. Eur J Surg Oncol. 2012;38:375–81. doi:10.1016/j.ejso.2012.02.179.
Olsen MA, Nickel KB, Margenthaler JA, et al. Increased risk of surgical-site infection among breast-conserving surgery re-excisions. Ann Surg Oncol. 2015;22:2003–9. doi:10.1245/s10434-014-4200-x.
Pataky R, Baliski C. Reoperation costs in attempted breast-conserving surgery: a decision analysis. Curr Oncol. 2016;23(5): 314–321.
Esbona K, Li Z, Wilke LG. Intraoperative imprint cytology and frozen section pathology for margin assessment in breast conservation surgery: a systematic review. Ann Surg Oncol. 2012;19:3236–45. doi:10.1245/s10434-012-2492-2.
Azu M, Abrahamse P, Katz SJ, Jagsi R, Morrow M. What is an adequate margin for breast-conserving surgery? Surgeon attitudes and correlates. Ann Surg Oncol. 2010;17:558–63. doi:10.1245/s10434-009-0765-1.
DeSnyder SM, Hunt KK, Smith BD, Moran MS, Klimberg S, Lucci A. Assessment of practice patterns following publication of the SSO-ASTRO consensus guideline on margins for breast-conserving therapy in stage I and II invasive breast cancer. Ann Surg Oncol. 2015;22:3250–6. doi:10.1245/s10434-015-4666-1.
Houssami N, Macaskill P, Marinovich ML, Morrow M. The association of surgical margins and local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy: a meta-analysis. Ann Surg Oncol. 2014;21:717–30. doi:10.1245/s10434-014-3480-5.
Moran MS, Schnitt SJ, Giuliano AE, et al. Society of surgical oncology–American society for radiation oncology consensus guideline on margins for breast-conserving surgery with whole-breast irradiation in stages I and II invasive breast cancer. J Clin Oncol. 2014;32:1507–15. doi:10.1200/JCO.2013.53.3935.
Hunt KK, Sahin AA. Too much, too little, or just right? Tumor margins in women undergoing breast-conserving surgery. J Clin Oncol. 2014;32:1401–6. doi:10.1200/JCO.2013.54.8388.
Patten CR. Changes in margin re-excision rates: a single-institution study. Ann Surg Oncol. 2016;23:49.
Pink GH, Bolley HB. Physicians in health care management: 3. Case mix groups and resource intensity weights: an overview for physicians. CMAJ Can Med Assoc J. 1994;150:889–94.
Statistics Canada. CANSIM Table 326-0021: Consumer Price Index (CPI), Annual, Health Care. Statistics Canada, Ottawa, 2013.
Hughes L, Hamm J, McGahan C, Baliski C. Surgeon volume, patient age, and tumor-related factors influence the need for re-excision after breast-conserving surgery. Ann Surg Oncol. 2016. doi:10.1245/s10434-016-5602-8.
de Camargo Cancela M, Comber H, Sharp L. Hospital and surgeon caseload are associated with risk of reoperation following breast-conserving surgery. Breast Cancer Res Treat. 2013;140:535–44. doi:10.1007/s10549-013-2652-5.
Wilke LG, Czechura T, Wang C, et al. Repeat surgery after breast conservation for the treatment of stage 0 to II breast carcinoma: a report from the national cancer data base, 2004–2010. JAMA Surg. 2014;149(12):1296–1305. doi:10.1001/jamasurg.2014.926 .
Spilsbury K, Semmens JB, Saunders CM, Hall SE, Holman CD. Subsequent surgery after initial breast-conserving surgery: a population-based study. ANZ J Surg. 2005;75:260–4. doi:10.1111/j.1445-2197.2005.03352.x .
Jeevan R, Cromwell DA, Trivella M, et al. Reoperation rates after breast-conserving surgery for breast cancer among women in England: retrospective study of hospital episode statistics. BMJ. 2012;345:e4505. doi:10.1136/bmj.e4505.
Canadian Institute for Health Information. Breast Cancer Surgery in Canada, 2007–2008 to 2009–2010. Ottawa, ON, Canada: CIHI; 2012. p. 47. Retrieved 30 August 2015 at https://secure.cihi.ca/estore/productbrowse.htm.
Abedi N, Ho AL, Knox A, et al. Predictors of mastectomy flap necrosis in patients undergoing immediate breast reconstruction: a review of 718 patients. Ann Plast Surg. 2014. doi:10.1097/SAP.0000000000000262.
Landercasper J, Attai D, Atisha D, et al. Toolbox to reduce lumpectomy reoperations and improve cosmetic outcome in breast cancer patients: the American society of breast surgeons consensus conference. Ann Surg Oncol. 2015;22:3174–83. doi:10.1245/s10434-015-4759-x.
Birkmeyer JD, Reames BN, McCulloch P, Carr AJ, Campbell WB, Wennberg JE. Understanding of regional variation in the use of surgery. Lancet. 2013;382:1121–9. doi:10.1016/S0140-6736(13)61215-5.
Reames BN, Shubeck SP, Birkmeyer JD. Strategies for reducing regional variation in the use of surgery: a systematic review. Ann Surg. 2014;259:616–27. doi:10.1097/SLA.0000000000000248.
Schwartz T, Degnim AC, Landercasper J. Should re-excision lumpectomy rates be a quality measure in breast-conserving surgery? Ann Surg Oncol. 2013;20:3180–3. doi:10.1245/s10434-013-3206-0.
McCahill LE, Single RM, Aiello Bowles EJ, et al. Variability in reexcision following breast conservation surgery. JAMA. 2012;307:467–75. doi:10.1001/jama.2012.43.
McCahill LE, Privette A, James T, et al. Quality measures for breast cancer surgery: initial validation of feasibility and assessment of variation among surgeons. Arch Surg. 2009;144:455–62; discussion 462–3. doi:10.1001/archsurg.2009.56.
Landercasper J, Whitacre E, Degnim AC, Al-Hamadani M. Reasons for re-excision after lumpectomy for breast cancer: insight from the American society of breast surgeons mastery (SM) database. Ann Surg Oncol. 2014;21:3185–91. doi:10.1245/s10434-014-3905-1.
Thavorn K, Wang Z, Fergusson D, van Katwyk S, Arnaout A, Clemons M. Cost implications of unwarranted imaging for distant metastasis in women with early-stage breast cancer in Ontario. Curr Oncol. 2016;23(Suppl 1):S52–5. doi:10.3747/co.23.2977.
Camp MS, Greenup RA, Taghian A, et al. Application of ACOSOG Z0011 criteria reduces perioperative costs. Ann Surg Oncol. 2013;20:836–41. doi:10.1245/s10434-012-2664-0.
Abe SE, Hill JS, Han Y, et al. Margin re-excision and local recurrence in invasive breast cancer: a cost analysis using a decision tree model. J Surg Oncol. 2015;112:443–8. doi:10.1002/jso.23990.
The 6 Domains of Health Care Quality. Retrieved 27 March 2016 at https://cahps.ahrq.gov/consumer-reporting/talkingquality/create/sixdomains.html.
Roberts A, Baxter N, Camacho X, Lau C, Zhong T. Once is rarely enough: a population-based study of reoperations after postmastectomy breast reconstruction. Ann Surg Oncol. 2015;22:3302–7. doi:10.1245/s10434-015-4716-8.
Acknowledgement
The authors thank Ms. Lauren Hughes, Student Intern-PREDICT at the BC Cancer Agency’s Sindi Ahluwalia Hawkins Centre for the Southern Interior, for her statistical support. Funding for her work has been provided through the BC Cancer Foundation. The Canadian Centre for Applied Research in Cancer Control is Funded by the Canadian Cancer Society Research Institute (Grant #2015-703549).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Baliski, C.R., Pataky, R.E. Influence of the SSO/ASTRO Margin Reexcision Guidelines on Costs Associated with Breast-Conserving Surgery. Ann Surg Oncol 24, 632–637 (2017). https://doi.org/10.1245/s10434-016-5678-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5678-1