
Abstract
Background
For asymptomatic benign papillomas detected at ultrasonography-guided 14-gauge core-needle biopsy (US–CNB), the decision to perform excision versus observation has been a topic of debate. We sought to determine which subgroup of asymptomatic benign papillomas without atypia diagnosed at US–CNB can be safely managed by observation versus immediate excision.
Materials
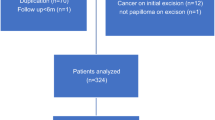
Overall, 230 asymptomatic benign papillomas in 197 women (mean age 46.6 ± 9.5 years; range 22–78), diagnosed at US–CNB using immunohistochemistry staining when needed and then managed by surgery (n = 144) or vacuum-assisted excision (VAE) with at least 12 months of follow-up after benign VAE results (n = 86) were included in this study. The upgrade rate to malignancy was calculated. Clinical and radiological variables, including age, size, Breast Image Reporting and Data System (BI–RADS) category, and imaging–pathology correlation were evaluated to find associations with malignancy using multivariate analysis.
Results
The upgrade rate to malignancy was 2.6 % (6 of 230): four were ductal carcinomas in situ and two were 1.5- and 9-mm-sized invasive ductal carcinomas without lymph node metastasis. The upgrade rates of papillomas with a BI–RADS category 3–4a and imaging–pathology concordance were 1.4 and 1.8 %, respectively. Category 4b–5 and imaging–pathology discordance were independently associated with malignancy, with upgrade rates of 13 and 50 %, respectively. Age and lesion size were not associated with malignancy.
Conclusion
Asymptomatic benign papillomas with probable benign or low suspicious US features or imaging–pathology concordance can be followed-up as opposed to immediate excision.

Similar content being viewed by others


References
Mulligan AM, O’Malley FP. Papillary lesions of the breast: a review. Adv Anat Pathol. 2007;14:108–19.
Ueng S-H, Mezzetti T, Tavassoli FA. Papillary neoplasms of the breast: a review. Arch Pathol Lab Med. 2009;133:893–907.
Jaffer S, Nagi C, Bleiweiss IJ. Excision is indicated for intraductal papilloma of the breast diagnosed on core needle biopsy. Cancer. 2009;115:2837–43.
Mcghan LJ, Pockaj BA, Wasif N, Giurescu ME, Mccullough AE, Gray RJ. Papillary lesions on core breast biopsy: excisional biopsy for all patients? Am Surg. 2013;79:1238–42.
Moritani S, Ichihara S, Hasegawa M, et al. Uniqueness of ductal carcinoma in situ of the breast concurrent with papilloma: implications from a detailed topographical and histopathological study of 50 cases treated by mastectomy and wide local excision. Histopathology. 2013;63:407–17.
Bode M, Rissanen T, Apaja-Sarkkinen M. Ultrasonography-guided core needle biopsy in differential diagnosis of papillary breast tumors. Acta Radiol. 2009;50:722–9.
Ko ES, Cho N, Cha JH, Park JS, Kim SM, Moon WK. Sonographically-guided 14-gauge core needle biopsy for papillary lesions of the breast. Korean J Radiol. 2007;8:206–11.
Tseng H, Chen Y, Chen S, et al. The management of papillary lesion of the breast by core needle biopsy. Eur J Surg Oncol. 2009;35:21–4.
Kil W-H, Cho EY, Kim JH, Nam S-J, Yang J-H. Is surgical excision necessary in benign papillary lesions initially diagnosed at core biopsy? Breast. 2008;17:258–62.
Shin HJ, Kim HH, Kim SM, et al. Papillary lesions of the breast diagnosed at percutaneous sonographically guided biopsy: comparison of sonographic features and biopsy methods. Am J Roentgenol. 2008;190:630–6.
Cheng T-Y, Chen C-M, Lee M-Y, et al. Risk factors associated with conversion from nonmalignant to malignant diagnosis after surgical excision of breast papillary lesions. Ann Surg Oncol. 2009;16:3375–9.
Youk JH, Kim E-K, Kwak JY, Son EJ. Atypical papilloma diagnosed by sonographically guided 14-gauge core needle biopsy of breast mass. Am J Roentgenol. 2010;194:1397–402.
Georgian-Smith D, Lawton TJ. Controversies on the management of high-risk lesions at core biopsy from a radiology/pathology perspective. Radiol Clin North Am. 2010;48:999–1012.
Ivan D, Selinko V, Sahin AA, Sneige N, Middleton LP. Accuracy of core needle biopsy diagnosis in assessing papillary breast lesions: histologic predictors of malignancy. Mod Pathol. 2004;17:165–71.
Youk JH, Kim E-K, Kwak JY, Son EJ, Park B-W, Kim S-I. Benign papilloma without atypia diagnosed at US-guided 14-gauge core-needle biopsy: clinical and US features predictive of upgrade to malignancy. Radiology. 2011;258:81–8.
Swapp RE, Glazebrook KN, Jones KN, et al. Management of benign intraductal solitary papilloma diagnosed on core needle biopsy. Ann Surg Oncol. 2013;20:1900–5.
Nakhlis F, Ahmadiyeh N, Lester S, Raza S, Lotfi P, Golshan M. Papilloma on core biopsy: excision vs. observation. Ann Surg Oncol. 2015;22:1479–82.
Fu C-Y, Chen T-W, Hong Z-J, et al. Papillary breast lesions diagnosed by core biopsy require complete excision. Eur J Surg Oncol. 2012;38:1029–35.
Shouhed D, Amersi FF, Spurrier R, et al. Intraductal papillary lesions of the breast: clinical and pathological correlation. Am Surg. 2012;78:1161–5.
Skandarajah AR, Field L, Mou AYL, et al. Benign papilloma on core biopsy requires surgical excision. Ann Surg Oncol. 2008;15:2272–7.
Rizzo M, Linebarger J, Lowe MC, et al. Management of papillary breast lesions diagnosed on core-needle biopsy: clinical pathologic and radiologic analysis of 276 cases with surgical follow-up. J Am Coll Surg. 2012;214:280–7.
Nakhlis F, Ahmadiyeh N, Lester S, Raza S, Lotfi P, Golshan M. Papilloma on core biopsy: excision vs. observation. Ann Surg Oncol. 2015;22(5):1479–82.
Agoff SN, Lawton TJ. Papillary lesions of the breast with and without atypical ductal hyperplasia can we accurately predict benign behavior from core needle biopsy? Am J Clin Pathol. 2004;122:440–3.
Ahmadiyeh N, Stoleru MA, Raza S, Lester SC, Golshan M. Management of intraductal papillomas of the breast: an analysis of 129 cases and their outcome. Ann Surg Oncol. 2009;16:2264–9.
Sakorafas G. Nipple discharge: current diagnostic and therapeutic approaches. Cancer Treat Rev. 2001;27:275–82.
Nayak A, Carkaci S, Gilcrease MZ, et al. Benign papillomas without atypia diagnosed on core needle biopsy: experience from a single institution and proposed criteria for excision. Clin Breast Cancer. 2013;13:439–49.
Berg WA, Blume JD, Cormack JB, et al. Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer. JAMA. 2008;299:2151–63.
Carder P, Garvican J, Haigh I, Liston J. Needle core biopsy can reliably distinguish between benign and malignant papillary lesions of the breast. Histopathology. 2005;46:320–7.
Furuya C, Kawano H, Yamanouchi T, Oga A, Ueda J, Takahashi M. Combined evaluation of CK5/6, ER, p63, and MUC3 for distinguishing breast intraductal papilloma from ductal carcinoma in situ. Pathol Int. 2012;62:381–90.
Grin A, O’Malley FP, Mulligan AM. Cytokeratin 5 and estrogen receptor immunohistochemistry as a useful adjunct in identifying atypical papillary lesions on breast needle core biopsy. Am J Surg Pathol. 2009;33:1615–23.
Koo JS, Han K, Kim MJ, Moon HJ, Kim E-K, Park B-W. Can additional immunohistochemistry staining replace the surgical excision for the diagnosis of papillary breast lesions classified as benign on 14-gage core needle biopsy? Breast Cancer Res Treat. 2013;137:797–806.
American College of Radiology. Breast imaging reporting and data system (BI-RADS). 4th ed. Reston: American College of Radiology; 2003.
Salkowski LR, Fowler AM, Burnside ES, Sisney GA. Utility of 6-month follow-up imaging after a concordant benign breast biopsy result. Radiology. 2011;258:380–7.
Youk JH, Jung I, Kim E-K, et al. US follow-up protocol in concordant benign result after US-guided 14-gauge core needle breast biopsy. Breast Cancer Research Treat. 2012;132:1089–97.
Moon HJ, Jung I, Youk JH, Kim MJ, Kim E-K. Short-term follow-up in 6 months is unnecessary for asymptomatic breast lesions with benign concordant results obtained at ultrasonography-guided 14-gauge core needle biopsy. Am J Surg. 2016;211:152–8.
Kim MJ, Kim E-K, Kwak JY, et al. Nonmalignant papillary lesions of the breast at US-guided directional vacuum-assisted removal: a preliminary report. Eur Radiol. 2008;18:1774–83.
Youk JH, Kim MJ, Son EJ, Kwak JY, Kim E-K. US-guided vacuum-assisted percutaneous excision for management of benign papilloma without atypia diagnosed at US-guided 14-gauge core needle biopsy. Ann Surg Oncol. 2012;19:922–8.
Kalof A, Tam D, Beatty B, Cooper K. Immunostaining patterns of myoepithelial cells in breast lesions: a comparison of CD10 and smooth muscle myosin heavy chain. J Clin Pathol. 2004;57:625–9.
Youden WJ. Index for rating diagnostic tests. Cancer. 1950;3:32–5.
Youk JH, Kim E-K, Kim MJ, et al. Concordant or discordant? Imaging-pathology correlation in a sonography-guided core needle biopsy of a breast lesion. Korean J Radiol. 2011;12:232–40.
SL Z, KY L. Longitudinal data analysis for discrete and continuous outcomes. Biometrics. 1986;42(1):121–30.
Jung S-Y, Kang H-S, Kwon Y, et al. Risk factors for malignancy in benign papillomas of the breast on core needle biopsy. World J Surg. 2010;34:261–5.
Sakr R, Rouzier R, Salem C, et al. Risk of breast cancer associated with papilloma. Eur J Surg Oncol. 2008;34:1304–8.
Wen X, Cheng W. Nonmalignant breast papillary lesions at core-needle biopsy: a meta-analysis of underestimation and influencing factors. Ann Surg Oncol. 2013;20:94–101.
Hall FM. Screening mammography guidelines: an alternative proactive approach. Radiology. 2014;273:646–51.
Graf O, Helbich TH, Hopf G, Graf C, Sickles EA. Probably benign breast masses at US: is follow-up an acceptable alternative to biopsy? Radiology. 2007;244:87–93.
Sickles EA. Probably benign breast lesions: when should follow-up be recommended and what is the optimal follow-up protocol? Radiology. 1999;213:11–4.
Mercado CL, Hamele-Bena D, Oken SM, Singer CI, Cangiarella J. Papillary Lesions of the breast at percutaneous core-needle biopsy. Radiology. 2006;238:801–8.
Shah V, Flowers C, Douglas‐Jones A, Dallimore N, Rashid M. Immunohistochemistry increases the accuracy of diagnosis of benign papillary lesions in breast core needle biopsy specimens. Histopathology. 2006;48:683–91.
Disclosures
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kim, SY., Kim, EK., Lee, H.S. et al. Asymptomatic Benign Papilloma Without Atypia Diagnosed at Ultrasonography-Guided 14-Gauge Core Needle Biopsy: Which Subgroup can be Managed by Observation?. Ann Surg Oncol 23, 1860–1866 (2016). https://doi.org/10.1245/s10434-016-5144-0
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5144-0