
Abstract
Background
Demand for nipple-sparing mastectomy (NSM) has increased. The authors’ initial NSM guidelines included risk reduction and cancers 2 cm or smaller located more than 2 cm from the nipple. The relative contraindications included obesity, large and/or ptotic breasts, and prior radiation. This study aimed to evaluate changes over time in NSM indications, surgical approach, and early outcomes.
Methods
After institutional review board approval, the study identified 354 patients scheduled for 588 NSMs, 341 (96 %) of whom underwent 566 NSMs. Changes across time [early (2009–2010), mid (2011–2012), and recent (2013–6/2014)] were assessed using tests for linear trend.
Results
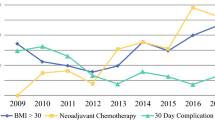
For patients undergoing reconstruction, NSMs increased from 24 % (early) to 40 % (recent) (p = 0.004). Among the NSM patients, average body mass index, proportion with bra cup sizes of C or larger, and prior radiation increased significantly over time. Performance of NSM for tumors 2 cm or less from the nipple increased from 5 to 18 %, and after neoadjuvant therapy, from 8 to 21.5 % (p = 0.02). Use of inframammary, radial, and reduction-type incisions increased over time, together with intraoperative laser angiography (both p < 0.0001). Concomitantly, the overall complication rate, complications requiring treatment, and postoperative nipple loss decreased. During a median follow-up period of 19 months, five locoregional recurrences (LRR) were observed, for an estimated 2-year LRR rate of 1.7 % [95 % confidence interval (CI), 0–3.9 %].
Conclusions
Over time, the indications for NSM expanded in terms of patient characteristics, tumor stage, and prior therapy, whereas the complication rates decreased. Excellent short-term outcomes suggest that NSM is a reasonable approach for many risk-reduction and cancer patients without disease in the nipple–areolar complex. Further study is needed to assess long-term aesthetics, patient satisfaction, and oncologic safety.



Similar content being viewed by others


References
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29.
Tuttle TM, Habermann EB, Grund EH, Morris TJ, Virnig BA. Increasing use of contralateral prophylactic mastectomy for breast cancer patients: a trend toward more aggressive surgical treatment. J Clin Oncol. 2007;25:5203–9.
Habermann EB, Thomsen KM, Hieken TJ, Boughey JC. Impact of availability of immediate breast reconstruction on bilateral mastectomy rates for breast cancer across the United States: data from the nationwide inpatient sample. Ann Surg Oncol. 2014;21:3290–6.
Kummerow KL, Du L, Penson DF, Shyr Y, Hooks MA. Nationwide trends in mastectomy for early-stage breast cancer. JAMA Surg. 2015;150:9–16.
Canavan J, Truong PT, Smith SL, Lu L, et al. Local recurrence in women with stage I breast cancer: declining rates over time in a large, population-based cohort. Int J Radiat Oncol Biol Phys. 2014;88:80–6.
Wapnir I, Dua M, Kieryn A, et al. Intraoperative imaging of nipple perfusion patterns and ischemic complications in nipple-sparing mastectomies. Ann Surg Oncol. 2014;21:100–6.
de Alcantara Filho P, Capko D, Barry JM, Morrow, M, Pusic A, Sacchini, VS. Nipple-sparing mastectomy for breast cancer and risk-reducing surgery: the Memorial Sloan-Kettering Cancer Center experience. Ann Surg Oncol. 2011;18:3117–22.
Burdge EC, Yuen J, Hardee M, et al. Nipple skin-sparing mastectomy is feasible for advanced disease. Ann Surg Oncol. 2013;20:3294–302.
Coopey SB, Tang R, Lei L, et al. Increasing eligibility for nipple-sparing mastectomy. Ann Surg Oncol. 2013;20:3218–22.
Wang F, Peled AW, Garwood E, et al. Total skin-sparing mastectomy and immediate breast reconstruction: an evolution of technique and assessment of outcomes. Ann Surg Oncol. 2014;21:3223–30.
Agarwal JP, Mendenhall SD, Anderson LA, Ying J, Boucher KM, Liu T, Neumayer, LA. The breast reconstruction evaluation of acellular dermal matrix as a sling trial (BREASTrial): design and methods of a prospective randomized trial. Plast Reconstr Surg. 2015;135:20–8e.
Petit JY, Veronesi U, Orecchia R, et al. Risk factors associated with recurrence after nipple-sparing mastectomy for invasive and intraepithelial neoplasia. Ann Oncol. 2012;23:2053–8.
Gabos Z, Thoms J, Ghosh S, Hanson J, Deschenes, J, Sabri, S, Abdulkarim B. The association between biological subtype and locoregional recurrence in newly diagnosed breast cancer. Breast Cancer Res Treat. 2010;124:187–94.
Lin NU, Vanderplas A, Hughes ME, et al. Clinicopathologic features, patterns of recurrence, and survival among women with triple-negative breast cancer in the National Comprehensive Cancer Network. Cancer. 2012;118:5463–72.
Shons AR, Press BH. Subcutaneous mastectomy: indications, technique, and applications. Arch Surg. 1983;118:844–50.
Yugueros P, Bite U. current concepts and techniques in subcutaneous mastectomy. Oper Tech Gen Surg. 2000;2:110–17.
Cense HA, Rutgers EJ, Lopes Cardozo M, Van Lanschot JJ. Nipple-sparing mastectomy in breast cancer: a viable option? Eur J Surg Oncol. 2001;27:521–6.
Simmons RM, Brennan M, Christos P, King V, Osborne M. Analysis of nipple/areolar involvement with mastectomy: can the areola be preserved? Ann Surg Oncol. 2002;9:165–8.
Sakurai T, Zhang N, Suzuma T, Umemura T, Yoshimura G, Sakurai T, Yang Q. Long-term follow-up of nipple-sparing mastectomy without radiotherapy: a single-center study at a Japanese institution. Med Oncol. 2013;30:481.
Stanec Z, Zic R, Budi S, et al. Skin and nipple–areola complex-sparing mastectomy in breast cancer patients: 15-year experience. Ann Plast Surg. 2014;73:485–91.
Regnault P. Breast ptosis: definition and treatment. Clin Plast Surg. 1976;3:193–203.
Kim HJ, Park EH, Lim WS, et al. Nipple–areola skin-sparing mastectomy with immediate transverse rectus abdominis musculocutaneous flap reconstruction is an oncologically safe procedure: a single-center study. Ann Surg. 2010;251:493–8.
Gerber B, Krause A, Reimer T, et al. Skin-sparing mastectomy with conservation of the nipple–areola complex and autologous reconstruction is an oncologically safe procedure. Ann Surg. 2003;238:120–7.
Laronga C, Kemp B, Johnston D, Robb GL, Singletary SE. The incidence of occult nipple–areola complex involvement in breast cancer patients receiving a skin-sparing mastectomy. Ann Surg Oncol. 1999;6:609–13.
Crowe JP, Patrick RJ, Yetman RJ, Djohan R. Nipple-sparing mastectomy update: one hundred forty-nine procedures and clinical outcomes. Arch Surg. 2008;143:1106–10.
Byon W, Kim E, Kwon J, Park YL, Park C. Magnetic resonance imaging and clinicopathological factors for the detection of occult nipple involvement in breast cancer patients. J Breast Cancer. 2014;17:386–92.
Boneti C, Yuen J, Santiago C, et al. Oncologic safety of nipple skin-sparing or total skin-sparing mastectomies with immediate reconstruction. J Am Coll Surg. 2011;212:686–93.
Steen ST, Chung AP, Han SH, Vinstein Al, Yoon JL, Giuliano AE. Predicting nipple–areolar involvement using preoperative breast MRI and primary tumor characteristics. Ann Surg Oncol. 2013;20:633–9.
Brachtel EF, Rusby JE, Michaelson JS, Chen LL, Muzikansky A, Smith BL, Koerner FC. Occult nipple involvement in breast cancer: clinicopathologic findings in 316 consecutive mastectomy specimens. J Clin Oncol. 2009;27:4948–54.
Jensen JA, Orringer JS, Giuliano AE. Nipple-sparing mastectomy in 99 patients with a mean follow-up of 5 years. Ann Surg Oncol. 2011;18:1665–70.
Babiera G, Simmons R. Nipple–areolar complex-sparing mastectomy: feasibility, patient selection, and technique. Ann Surg Oncol. 2010;17(Suppl 3):245–8.
Salibian AH, Harness JK, Mowlds DS. Inframammary approach to nipple–areola-sparing mastectomy. Plast Reconstr Surg. 2013;132:700e–8e.
Petit JY, Veronesi U, Lohsiriwat V, et al. Nipple-sparing mastectomy: is it worth the risk? Nat Rev Clin Oncol. 2011;8:742–7.
Duggal CS, Madni T, Losken A. An outcome analysis of intraoperative angiography for postmastectomy breast reconstruction. Anesthet Surg. 2014;34:61–5.
Gerber B, Krause A, Dieterich M,Kundt G, Reimer T. The oncological safety of skin-sparing mastectomy with conservation of the nipple–areola complex and autologous reconstruction: an extended follow-up study. Ann Surg. 2009;249:461–8.
Disclosure
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Krajewski, A.C., Boughey, J.C., Degnim, A.C. et al. Expanded Indications and Improved Outcomes for Nipple-Sparing Mastectomy Over Time. Ann Surg Oncol 22, 3317–3323 (2015). https://doi.org/10.1245/s10434-015-4737-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4737-3