
Abstract
Background
Controversy continues regarding the use of adjuvant radiation therapy (RT) and hormonal therapy (HT) for patients undergoing breast-conserving therapy (BCT) for ductal carcinoma in situ (DCIS).
Methods
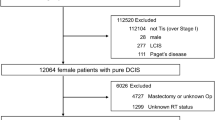
A prospective database was queried to identify women 18 years of age or older treated for DCIS from 2002 to 2013.
Results
BCT was completed for 300 patients with a median age of 66 years. The median DCIS size was 0.7 cm (range 0.1–6.0 cm). The DCIS grades were high (44 %), intermediate (37 %), and low (19 %). The closest margin was wider than 3 mm in 80 % and wider than 5 mm in 63 % of the cases. Adjuvant RT was administered to 183 patients (61 %), and the RT status of 9 patients (3 %) was unknown. RT was associated with age, DCIS size, comedo necrosis, grade, and treatment in 2002–2007 versus 2008–2013. Adjuvant HT was administered to 86 estrogen receptor-positive patients (39 %), and the HT status of 4 patients (2 %) was unknown. The median follow-up period was 63 months (range 4–151 months). The 5-year overall local recurrence (LR) rate was 4 % (95 % confidence interval [CI] 2.1–7.4 %). The 5-year LR rate was 3.9 % (95 % CI 1.8–8.6 %) for the RT patients and 4.1 % (95 % CI 1.6–10.7 %) for the patients not receiving RT. Of 13 LRs, 10 (77 %) were DCIS, and 3 (23 %) were invasive including one node-positive recurrence.
Conclusions
Multidisciplinary and joint decision making in the treatment of DCIS results in a substantial and increasing number of patients forgoing adjuvant RT, adjuvant HT, or both. Reasonable 5-year LR rates suggest that such decision making can appropriately allocate patients to adjuvant therapies.


Similar content being viewed by others


References
Ernster VL, et al. Mortality among women with ductal carcinoma in situ of the breast in the population-based surveillance, epidemiology, and end results program. Arch Intern Med. 2000;160:953–8.
Early Breast Cancer Trialists’ Collaborative G. Overview of the randomized trials of radiotherapy in ductal carcinoma in situ of the breast. J Natl Cancer Inst Monogr. 2010;2010:162–77.
Fisher B, et al. Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol. 1998;16:441–52.
Holmberg L, et al. Absolute risk reductions for local recurrence after postoperative radiotherapy after sector resection for ductal carcinoma in situ of the breast. J Clin Oncol. 2008;26:1247–52.
Cuzick J, et al. Effect of tamoxifen and radiotherapy in women with locally excised ductal carcinoma in situ: long-term results from the UK/ANZ DCIS trial. Lancet Oncol. 2011;12:21–9.
Donker M, et al. Breast-conserving treatment with or without radiotherapy in ductal carcinoma in situ: 15-year recurrence rates and outcome after a recurrence, from the EORTC 10853 randomized phase III trial. J Clin Oncol. 2013;31:4054–9.
Fisher B, et al. Tamoxifen in treatment of intraductal breast cancer: National Surgical Adjuvant Breast and Bowel Project B-24 randomised controlled trial. Lancet. 1999;353:1993–2000.
Kim T, et al. Is radiotherapy necessary for intermediate risk ductal carcinoma in situ after breast-conserving surgery? Springerplus. 2014;3:405.
Wapnir IL, et al. Long-term outcomes of invasive ipsilateral breast tumor recurrences after lumpectomy in NSABP B-17 and B-24 randomized clinical trials for DCIS. J Natl Cancer Inst. 2011;103:478–88.
Baxter NN, et al. Trends in the treatment of ductal carcinoma in situ of the breast. J Natl Cancer Inst. 2004;96:443–8.
Smith GL, Smith BD, Haffty BG. Rationalization and regionalization of treatment for ductal carcinoma in situ of the breast. Int J Radiat Oncol Biol Phys. 2006;65:1397–403.
Silverstein MJ, et al. The influence of margin width on local control of ductal carcinoma in situ of the breast. N Engl J Med. 1999;340:1455–61.
Wong JS, et al. Prospective study of wide excision alone for ductal carcinoma in situ of the breast. J Clin Oncol. 2006;24:1031–6.
Hughes LL, et al. Local excision alone without irradiation for ductal carcinoma in situ of the breast: a trial of the Eastern Cooperative Oncology Group. J Clin Oncol. 2009;27:5319–24.
McCormick B, et al. RTOG 9804: a prospective randomized trial for good-risk ductal carcinoma in situ comparing radiotherapy with observation. J Clin Oncol. 2015;33:709–15.
Silverstein MJ. The University of Southern California/Van Nuys prognostic index for ductal carcinoma in situ of the breast. Am J Surg. 2003;186:337–43.
Motwani SB, et al. Ductal carcinoma in situ treated with breast-conserving surgery and radiotherapy: a comparison with ECOG study 5194. Cancer. 2011;117:1156–62.
Solin LG, Gray R, Baehner FL, et al. A multigene expression assay to predict local recurrence risk for ductal carcinoma in situ of the breast. J Natl Cancer Inst. 2013;105:701–10.
Rudloff U, Jacks LM, Goldberg JI, et al. Nomogram for predicting the risk of local recurrence after breast-conserving surgery for ductal carcinoma in situ. J Clinic Oncol. 2010;28:3762–9.
MacDonald HR, et al. Local control in ductal carcinoma in situ treated by excision alone: incremental benefit of larger margins. Am J Surg. 2005;190:521–5.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Parikh, P., Pockaj, B., Wasif, N. et al. Multidisciplinary Shared Decision Making in the Management of Ductal Carcinoma In Situ of the Breast. Ann Surg Oncol 22 (Suppl 3), 516–521 (2015). https://doi.org/10.1245/s10434-015-4607-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4607-z