
Abstract
Purpose
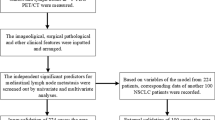
Maximum standardized uptake values (SUVmax) at the primary lesions of non-small-cell lung cancer in 18F-fluorodeoxyglucose positron emission tomography combined with computed tomography (FDG-PET/CT), and the microscopic local extension of tumors were examined to develop reliable criteria to determine candidates for sublobar resection.
Methods
We retrospectively analyzed 209 patients who underwent lobectomy, bilobectomy, or pneumonectomy with systematic lymph node dissection. Preoperative SUVmax at the primary lesion, microscopic lymphatic, venous, and pleural invasion in addition to lymph node metastases in the resected specimens were examined. Receiver operating characteristic analyses were used to predict an optimal cutoff for lymph node metastases.
Results
With receiver operating characteristic analysis, the areas under the curve for SUVmax and tumor size were 0.693 and 0.545, respectively, suggesting SUVmax superiority for prediction of lymph node metastases with a cutoff of 2.9. When a tumor was ≤2.0 cm (n = 41, 19.6 %), the percentages of microscopic lymphatic invasion, venous invasion, pleural invasion, and lymph node metastases were 12.2, 7.3, 4.9, and 17.1 %, respectively. When SUVmax was <3.0 (n = 91, 43.5 %), these percentages were 15.4, 3.3, 7.7, and 8.8 %, showing that SUVmax could efficiently exclude nodal metastases in more cases than tumor size. The postoperative 5-year survival rate was 86.6 % in patients with SUVmax < 3.0 and 58.1 % in patients with SUVmax ≥ 3.0 (p < 0.001).
Conclusions
18F-FDG uptake value was more useful than tumor size for selecting patients with non-small-cell lung cancer suitable for intentional sublobar resection.


Similar content being viewed by others


References
Ginsberg RJ, Rubinstein LV. Randomized trial of lobectomy versus limited resection for T1 N0 non–small cell lung cancer. Lung Cancer Study Group. Ann Thorac Surg. 1995;60:615–22.
Nakamura H, Kawasaki N, Taguchi M, Kabasawa K. Survival following lobectomy vs limited resection for stage I lung cancer: a meta-analysis. Br J Cancer. 2005;92:1033–7.
Asamura H, Nakayama H, Kondo H, Tsuchiya R, Shimosato Y, Naruke T. Lymph node involvement, recurrence, and prognosis in resected small, peripheral, non-small-cell lung carcinomas: are these carcinomas candidates for video-assisted lobectomy? J Thorac Cardiovasc Surg. 1996;111:1125–34.
Whitson BA, Groth SS, Andrade RS, Maddaus MA, Habermann EB, D’Cunha J. Survival after lobectomy versus segmentectomy for stage I non–small cell lung cancer: a population-based analysis. Ann Thorac Surg. 2011;92:1943–50.
Brown RS, Leung JY, Kison PV, Zasadny KR, Flint A, Wahl RL. Glucose transporters and FDG uptake in untreated primary human non–small cell lung cancer. J Nucl Med. 1999;40:556–65.
de Geus-Oei LF, van Krieken JH, Aliredjo RP, et al. Biological correlates of FDG uptake in non–small cell lung cancer. Lung Cancer. 2007;55:79–87.
Vansteenkiste JF, Stroobants SG, Dupont PJ, et al. Prognostic importance of the standardized uptake value on (18)F-fluoro-2-deoxy-glucose-positron emission tomography scan in non-small-cell lung cancer: an analysis of 125 cases. Leuven Lung Cancer Group. J Clin Oncol. 1999;17:3201–6.
Higashi K, Ueda Y, Arisaka Y, et al. 18F-FDG uptake as a biologic prognostic factor for recurrence in patients with surgically resected non–small cell lung cancer. J Nucl Med. 2002;43:39–45.
Ohtsuka T, Nomori H, Watanabe K, et al. Prognostic significance of [(18)F]fluorodeoxyglucose uptake on positron emission tomography in patients with pathologic stage I lung adenocarcinoma. Cancer. 2006;107:2468–73.
Pillot G, Siegel BA, Govindan R. Prognostic value of fluorodeoxyglucose positron emission tomography in non–small cell lung cancer: a review. J Thorac Oncol. 2006;1:152–9.
Nakamura H, Hirata T, Kitamura H, Nishikawa J. Correlation of the standardized uptake value in FDG-PET with the expression level of cell-cycle-related molecular biomarkers in resected non–small cell lung cancers. Ann Thorac Cardiovasc Surg. 2009;15:304–10.
Shiono S, Abiko M, Sato T. Positron emission tomography/computed tomography and lymphovascular invasion predict recurrence in stage I lung cancers. J Thorac Oncol. 2011;6:43–7.
Ueda K, Tanaka T, Hayashi M, Tanaka N, Li TS, Hamano K. What proportion of lung cancers can be operated by segmentectomy? A computed-tomography-based simulation. Eur J Cardiothorac Surg. 2012;41:341–5.
Veronesi G, Maisonneuve P, Pelosi G, et al. Screening-detected lung cancers: is systematic nodal dissection always essential? J Thorac Oncol. 2011;6:525–30.
Nakamura H, Saji H, Shinmyo T, et al. Close association of IASLC/ATS/ERS lung adenocarcinoma subtypes with glucose-uptake in positron emission tomography. Lung Cancer. 2015;87:28–33.
Goldstraw P. International Association for the Study of Lung Cancer. IASLC staging manual in thoracic oncology. Orange Park: Editorial Rx Press;2009.
Gupta NC, Tamim WJ, Graeber GG, Bishop HA, Hobbs GR. Mediastinal lymph node sampling following positron emission tomography with fluorodeoxyglucose imaging in lung cancer staging. Chest. 2001;120:521–7.
Guhlmann A, Storck M, Kotzerke J, Moog F, Sunder-Plassmann L, Reske SN. Lymph node staging in non–small cell lung cancer: evaluation by [18F]FDG positron emission tomography (PET). Thorax. 1997;52:438–41.
Al-Sarraf N, Gately K, Lucey J, Wilson L, McGovern E, Young V. Mediastinal lymph node staging by means of positron emission tomography is less sensitive in elderly patients with non-small-cell lung cancer. Clin Lung Cancer. 2008;9:39–43.
Yoshikawa K, Tsubota N, Kodama K, Ayabe H, Taki T, Mori T. Prospective study of extended segmentectomy for small lung tumors: the final report. Ann Thorac Surg. 2002;73:1055–8.
Koike T, Yamato Y, Yoshiya K, Shimoyama T, Suzuki R. Intentional limited pulmonary resection for peripheral T1 N0 M0 small-sized lung cancer. J Thorac Cardiovasc Surg. 2003;125:924–8.
Swanson SJ. Segmentectomy for lung cancer. Semin Thorac Cardiovasc Surg. 2010;22:244–9.
Okada M, Yoshikawa K, Hatta T, Tsubota N. Is segmentectomy with lymph node assessment an alternative to lobectomy for non–small cell lung cancer of 2 cm or smaller? Ann Thorac Surg. 2001;71:956–60.
Casiraghi M, Travaini LL, Maisonneuve P, et al. Lymph node involvement in T1 non-small-cell lung cancer: could glucose uptake and maximal diameter be predictive criteria? Eur J Cardiothorac Surg. 2011;39:e38–43.
Nakamura H, Saji H, Shinmyo T, et al. Association of IASLC/ATS/ERS histologic subtypes of lung adenocarcinoma with epidermal growth factor receptor mutations in 320 resected cases. Clin Lung Cancer. 2014.
Nakamura K, Saji H, Nakajima R, et al. A phase III randomized trial of lobectomy versus limited resection for small-sized peripheral non–small cell lung cancer (JCOG0802/WJOG4607L). Jpn J Clin Oncol. 2010;40:271–4.
Meng X, Sun X, Mu D, et al. Noninvasive evaluation of microscopic tumor extensions using standardized uptake value and metabolic tumor volume in non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2012;82:960–6.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Nakamura, H., Saji, H., Marushima, H. et al. Standardized Uptake Values in the Primary Lesions of Non-Small-Cell Lung Cancer in FDG-PET/CT Can Predict Regional Lymph Node Metastases. Ann Surg Oncol 22 (Suppl 3), 1388–1393 (2015). https://doi.org/10.1245/s10434-015-4564-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4564-6