
Abstract
Background
The independent segment between the superior and basal segments is called the subsuperior segment (S*), which is rarely observed. We report a left S* segmentectomy in a patient with early-stage lung cancer.
Case presentation
A 72-year-old man presented with a history of hilar cholangiocarcinoma. A left lung ground-glass nodule was detected during follow-up examination. The tumor shadow was localized in the left S* according to the findings of the three-dimensional image analysis system (SYNAPSE VINCENT®) with computed tomography-based analysis. S* segmentectomy was successfully performed with a sufficient surgical margin. The operation time was 147 min, and there was a small amount of bleeding. The pathological diagnosis was invasive adenocarcinoma measuring 3 mm. The tumor was successfully removed with a sufficient surgical margin. The patient was discharged from the hospital 8 days after surgery without any complications.
Conclusions
S* segmentectomy is not typically performed in patients with lung cancer due to insufficient surgical margins. However, S* segmentectomy is a viable option for selected patients with pulmonary metastasis or early-stage lung cancer.
Similar content being viewed by others


Background
Previous studies have reported varying frequencies of the lung bronchi and vessel branching types [1,2,3]. The subsuperior segment (S*) is located between the superior (S6) and basal segments. Shimizu et al. reported the first video-assisted thoracic surgery (VATS) for anatomical right S* segmentectomy [4]. They also reviewed the pulmonary bronchovascular pattern variations using three-dimensional computed tomography (CT) angiography and the right lobe bronchography. Right S* was detected in approximately 20% of cases [5]. Other reports have focused on the anatomical thoracic abnormalities detected via three-dimensional CT [6, 7]. Maki et al. described the pulmonary vessels and bronchial anatomy of the left lower lung and found a S* in 24% of patients [8].
We report a case of early-stage lung cancer treated with left S* segmentectomy.
Case presentation
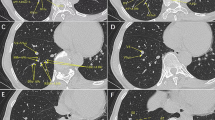
A 72-year-old man presented with a history of hilar cholangiocarcinoma. A left lung ground-glass nodule (GGN) measuring 1.1 cm in diameter was detected in the left lung S* segment during follow-up examination (Fig. 1).

a–f Chest computed tomography images. A subsuperior segmental bronchus (B*) and B7 were detected by thin section computed tomography, and a ground-glass nodule (GGN) was detected in the subsuperior (S*) segment. The subsuperior segmental vein (V*) was included in the S*
Preoperative three-dimensional CT (SYNAPSE VINCENT® analysis) revealed an independent B* bronchus and pulmonary artery (A*) distinct from those of the S6 and basal segment (Fig. 2). In addition, both left B7 and B* were appreciated on CT (Fig. 1). The S* was surrounded by S6, S7, S8, S9, and S10 (Fig. 2). Since performing wedge resection was difficult, independent S* segmentectomy was considered a suitable operation for this case. The distance between the tumor and S8 was the closest, 4.5 mm, and we thought it necessary to be careful when resecting between segments.

a–c A three-dimensional image finding constructed by SYNAPSE VINCENT. Relation to the lower bronchus, pulmonary artery, vein, segments, and tumor shadow. Colors of each segment and tumor: S*, green; S6, light green; S7, red; S8, purple; S9, yellow; S10, blue; tumor, pink. 2a Front view. 2b Between front- and left-side view. 2c Left-side view
First, the interlobar fissure was divided to identify the pulmonary artery. After identifying the superior segmental artery (A6), the peripheral side of the pulmonary artery was dissected. A* was identified between the basal segmental arteries A8 + 9 and A10. Second, after ligating and dissecting A*, the accompanying B* was identified. The tumor was palpable from the pleural surface, and a small-diameter bronchoscope was inserted into the orifice of B*, and selective air injection was performed. The S* segment was expanded until an inflation-deflation line was apparent. Finally, after marking the inflation-deflation line with conventional electrocautery, the central part of the intersegmental plane was dissected with electrocautery, and the peripheral part of the intersegmental plane was dissected along the marking line with automatic sutures (Fig. 3). The shortest margin distance from the tumor was S8/S*; we paid special attention to secure surgical margin dividing between S8 and S* with a sufficient surgical margin > 2 cm.

Thoracoscopic view. Structure of the segmental plane shown after S* segmentectomy in the operative view
The operation time was 147 min, and there was a small amount of bleeding. The pathological diagnosis was invasive adenocarcinoma measuring 3 mm. The tumor was successfully removed with sufficient surgical margins. The patient was discharged from the hospital 8 days after surgery without any complications.
Discussions and conclusions
Recent studies have reported the frequencies of right and left S* to be 20% [5] and 24% [8], respectively. An S* has an independent subsuperior segmental bronchus (B*) and pulmonary artery (A*), which has a small volume. S* is rarely observed, and segmentectomy is not typically performed in patients with primary lung cancer due to insufficient surgical margins. However, S* segmentectomy was deemed appropriate for early-stage lung cancer patients with pure GGN, metastatic lung tumor, and nonmalignant diseases, such as granulomas and congenital bronchial atresia, located in a part unresectable by wedge resection.
Identification of the intersegmental plane is one of the essential techniques for pulmonary segmentectomy [4, 5]. Since this left S* segmentectomy has multiple segmental planes between the S6 and basal segment, selective ventilation via bronchoscopy is effective and useful. We previously reported near-infrared-guided pulmonary segmentectomy after endobronchial indocyanine green (ICG) injection [9]. ICG injection via the bronchus or intravenous technique is useful in S* segmentectomy. We performed a left S* segmentectomy via a small open thoracotomy with a thoracoscope. Less invasive approaches such as VATS or uniportal VATS are technically possible [4, 10]. Even robot-assisted segmentectomy can be considered because firefly fluorescence imaging with the da Vinci Surgical System to utilize ICG is available [11]. In this case, we preoperatively identified an independent B* bronchus and pulmonary artery (A*) distinct from the S6 and basal segment. The left S* segmentectomy was safely performed. Furthermore, left B7, seen in 7.9% of cases [8], was also detected. Failure to note these anatomic variants preoperatively could have led to an inadvertent left S8 segmentectomy. Preoperative three-dimensional multi-dissector CT angiography allows visualization of the pulmonary vasculature and bronchi anatomy to help detect anatomical variants. This was recommended for surgical planning in patients undergoing lung resection, particularly in cases with complicated segmentectomy for lung cancer [4, 11]. For non-small cell lung cancer with a major axis of 2 cm or less and a lesion-filled area ratio of greater than 0.5 to the maximum lesion diameter, segmental resection should be standard surgery [12]. Although the lesions in this case were relatively peripheral, it should be considered that this may not be the case for more centrally located tumors or larger tumors, in which multi-segment resection is preferred. Left S* segmentectomy is technically feasible for selected patients with nodules in the S*. Three-dimensional CT findings are useful for preoperative planning for S* segmentectomy.
Availability of data and materials
All data supporting the conclusions of this article are included within the published article.
Abbreviations
- S*:
-
Subsuperior segment
- VATS:
-
Video-assisted thoracic surgery
- GGN:
-
Ground-glass nodule
- CT:
-
Computed tomography
- ICG:
-
Indocyanine green
References
Boyden EA, Hamle CJ. An analysis of variations in the broncho-vascular patterns of the right middle lobe in fifty dissected and twenty injected lungs. J Thorac Surg. 1951;21:172–88.
Ferry RM, Boyden EA. Variations in the bronchovascular pat terns of the right lower lobe of fifty lungs. J Thorac Surg. 1951;22:188–201.
Yamashita H. Variations in the pulmonary segments and the bronchovascular trees. Roentgenologic anatomy of the lung. Tokyo: Igaku-syoin; 1978.
Shimizu K, Mogi A, Yajima T, Nagashima T, Ohtaki Y, Obayashi K, et al. Thoracoscopic subsuperior segment segmentectomy. Soc Thorac Surg. 2017;104:e407–10.
Nagashima T, Shimizu K, Ohtaki Y, Obayashi K, Nakazawa S, Kuwano H, et al. Analysis of variation in bronchovascular pattern of the right middle and lower lobes of the lung using three-dimensional CT angiography and bronchography. Gen Thorac Cardiovasc Surg. 2017;65:e343–9.
Akiba T, Marushima H, Odaka M, Harada J, Kobayashi S, Morikawa T. Pulmonary vein analysis using three-dimentional computed tomography angiography for thoracic surgery. Gen Thorac Cardiovasc Surg. 2010;58:331–5.
Ishikawa Y, Iwano S, Usami N, Yokoi K. An anomalous segmental vein of the left upper lobe of the lung: preoperative identification by three-dimensional computed tomography pulmonary angiography. Interact Cardiovasc Thorac Surg. 2012;15:512–3.
Maki R, Miyajima M, Ogura K, Tada M, Takahashi Y, Arai W, et al. Pulmonary vessels and bronchial anatomy of the left lower lobe. Surg Today. 2020;50:1081–90.
Wada H, Yamamoto T, Morimoto J, Sakairi Y, Suzuki H, Nakajima T, et al. Near-infrared-guided pulmonary segmentectomy after endobronchial indocyanine green injection. Ann Thorac Surg. 2020;109:396–403.
Liu G, Hu H, Mao Z, Dong P, Zhang S, Mao Z. Modifed left subsuperior segmentectomy via 2-cm uniportal video-assisted thoracoscopic surgery. Surg Today. 2021;51(1):172–5.
Le Moal J, Peillon C, Dacher JN, Baste JM. Three-dimensional computed tomography reconstruction for operative planning in robotic segmentectomy: a pilot study. J Thorac Dis. 2018;10(1):196–201.
Saji H, Okada M, Tsuboi M, Nakajima R, Suzuki K, Aokage K, et al. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG0802/WJOG4607L): a multicentre, open-label, phase 3, randomised, controlled, non-inferiority trialpulmonary vein analysis using three-dimentional computed tomography angiography for thoracic surgery. Lancet. 2022;399:1607–17.
Acknowledgements
The authors thank Editage (www.editage.jp) for the English language review.
Funding
None.
Author information
Authors and Affiliations
Contributions
HO and HS performed the surgery, and HO, HS, TK, AH, KT, and YS followed up with the patient. The manuscript was prepared by HO and HS under the supervision of IY. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Patient privacy was considered, and the manuscript did not include any identifying information.
Consent for publication
The patient provided informed consent for publication of this case report.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Oeda, H., Suzuki, H., Kaiho, T. et al. Left subsuperior segmentectomy for a patient with early-stage lung cancer: a case report. Gen Thorac Cardiovasc Surg Cases 1, 12 (2022). https://doi.org/10.1186/s44215-022-00012-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s44215-022-00012-3