
Abstract
Background
A mediastinal aberrant goiter is extremely rare, characterized by independence from the thyroid gland. This tumor most commonly develops in the anterior mediastinum and should be differentiated from a thymoma. Moreover, as mediastinal aberrant goiters frequently have a blood supply arising from the thoracic great vessels, preoperative diagnosis and evaluation of the feeding vessel are vital for safe surgery. Herein, we report a rare case of mediastinal aberrant goiter characterized by high radiodensity on non-enhanced computed tomography (CT).
Case presentation
A 77-year-old woman underwent non-enhanced CT, which showed a 2.2-cm, well-circumscribed, homogeneous anterior mediastinal nodule with high radiodensity. The CT attenuation value of the nodule was as high as 91.9 Hounsfield units. A thymoma or mediastinal goiter was suspected owing to the tumor location and the lack of a cystic component. We performed anterior mediastinal tumor resection using video-assisted thoracoscopic surgery. Pathologically, variably sized follicles, indicative of thyroid tissue, were observed with hemorrhage and hemosiderin deposition. Moreover, papillary projections of small follicles (Sanderson’s polsters) were scattered without atypia of the follicular epithelium, indicative of an adenomatous goiter. The diagnosis of a mediastinal aberrant goiter was supported by the absence of an anatomical connection with the thyroid gland. The postoperative course was uneventful, and the patient was discharged on postoperative day 5.
Conclusion
The thyroid gland has a high radiodensity on non-enhanced CT, which correlates with iodine concentration. This radiological feature may be useful for the preoperative differentiation of mediastinal aberrant goiters containing thyroid tissue.
Similar content being viewed by others


Background
Intrathoracic goiters are a relatively rare type of goiter, and a mediastinal aberrant goiter without continuity with the thyroid gland is extremely rare [1, 2]. Aberrant mediastinal goiters frequently develop in the anterior mediastinum and should be differentiated from thymomas. Herein, we report a case of a mediastinal aberrant goiter in the anterior mediastinum characterized by high radiodensity on preoperative non-enhanced computed tomography (CT).
Case presentation
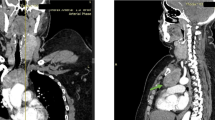
A chest non-enhanced CT scan in a 77-year-old woman with chronic cough revealed a 2.2-cm, well-circumscribed, homogeneous anterior mediastinal nodule with high radiodensity. The CT attenuation value of the nodule was 91.9 Hounsfield units (HU) (Fig. 1). The tumor had no connection to the thyroid gland and did not invade the surrounding organs. The patient’s medical history included second-degree atrioventricular heart block (pacemaker implantation) and diabetes mellitus. Magnetic resonance imaging (MRI) and positron emission tomography (PET)-CT were not performed. As a thymoma or mediastinal goiter was suspected owing to the tumor location and the lack of a cystic component, thoracoscopic anterior mediastinal tumor resection was performed. A lobular tumor was found in the left thymus lobe, but no tumor invasion was detected. The operation time was 1 h 55 min, with 20 g of blood loss. The encapsulated tumor was 2.3 × 2.2 × 1.9 cm in size, with a solid brownish cut surface and scattered hemorrhage deposition. Pathological examination revealed unequal-sized thyroid follicles, Sanderson’s polsters, and papillary projections of small follicles. There was no epithelial atypia and the pathological diagnosis was an adenomatous goiter (Fig. 2). Anatomically, there was no continuity with the thyroid gland, and a mediastinal aberrant goiter was diagnosed. The patient’s postoperative course was uneventful, and she was discharged on postoperative day 5.

Preoperative imaging findings. Non-enhanced computed tomography (CT) scan. A solitary homogeneous anterior mediastinal tumor (2.0 cm in size) showed high radiodensity (CT value: 91.9 Hounsfield units)

Pathological findings. Unequal-sized thyroid follicles and papillary projections of small follicles (Sanderson’s polsters) were present without atypia of the follicular epithelium
Discussion and conclusions
Rives’ classification is a common anatomical classification system used for intrathoracic goiters [3]. Intrathoracic goiters are classified as substernal or mediastinal aberrant, regardless of whether continuity with the thyroid gland is present. Intrathoracic goiters account for 5% of all mediastinal tumors, and mediastinal aberrant goiters account for 2% of intrathoracic goiters (0.1% of all mediastinal tumors) [1, 2].
Aberrant mediastinal goiters are commonly reported in women ≥50 years. The tumor frequently arises from the anterior superior mediastinum, and blood tests often show euthyroidism [1, 3]. CT scans reveal a well-circumscribed tumor that may be accompanied with focal calcification deposition or cystic degeneration; moreover, enhanced CT shows prolonged enhancement [4, 5]. MRI is reliable for evaluating intrathoracic goiter extension but does not provide additional information in diagnostic yield to that from CT [6]. Significant fluorodeoxyglucose accumulation has been reported on PET-CT [1]. Preoperative differentiation between mediastinal aberrant goiters and thymomas, which is frequently made after excision, has been challenging due to the lack of specific radiological findings on both enhanced CT and MRI. Thyroid scintigraphy is a disease-specific examination for goiters, but limited accumulation has been reported for mediastinal aberrant goiters [5]. The use of preoperative endobronchial ultrasound-guided transbronchial needle aspiration has been reported in cases of intrathoracic goiters located in the superior mediastinum (adjacent to the trachea) [7]. However, a biopsy of intrathoracic goiters in the anterior mediastinum (similar to the goiters in our case) is difficult due to anatomical reasons.
In the thyroid gland, the iodine concentration in thyroid tissue is associated with a high radiodensity on non-enhanced CT [8, 9]. This finding may also apply to mediastinal aberrant goiters comprised of thyroid tissue. However, high radiodensity on non-enhanced CT (91.9 HU) was characteristic of the current case; thus, we suspected a mediastinal aberrant goiter. Mediastinal aberrant goiters have a blood supply arising from the thoracic vessels, such as the aorta or subclavian artery [3]; thus, preoperative diagnosis of mediastinal aberrant goiter allows for evaluation of the feeding vessel, which is necessary for safe surgery, especially in recent years with the increasing use of thoracoscopic and robotic surgery. Although we could not detect obvious blood supply from thoracic great vessels in the present case, an additional preoperative enhanced CT should be performed to preventing unforeseen bleeding.
The median CT value of four intrathoracic goiters on non-enhanced CT in our institution (including two cases of substernal goiter and a mediastinal aberrant goiter in the superior mediastinum) was 76.1 HU (interquartile range: 71.7–89.2). Although there are some reports on mediastinal aberrant goiters, only a few of these have presented the CT values for these goiters. A previous report determined the definite CT values of intrathoracic goiters to be 70–85 HU [9]. This is consistent with our findings. On the other hand, the median CT value of a thymoma was reported to be 39.5 HU (interquartile range: 33.7–42.2) [10], which is lower than that of a mediastinal aberrant goiter. However, intrathoracic goiters with a low concentration of iodine per unit volume, for example, owing to cystic degeneration, may have lower CT values [9]. Although further case accumulation is needed, preoperative non-enhanced CT values may be feasible for differentiating mediastinal aberrant goiters from thymomas.
Although mediastinal aberrant goiters are benign entities, 3–6% of these are known to undergo malignant transformation [11]. Therefore, we believe that surgery should be performed even under preoperative suspicion of a mediastinal aberrant goiter.
We encountered a rare surgical case of a mediastinal aberrant goiter characterized by high radiodensity on non-enhanced CT. An anterior mediastinal tumor with a high radiodensity should be considered a mediastinal aberrant goiter.
Availability of data and materials
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
Abbreviations
- CT:
-
Computed tomography
- HU:
-
Hounsfield units
- MRI:
-
Magnetic resonance imaging
- PET:
-
Positron emission tomography
References
Gamblin TC, Jennings GR, Christie DB 3rd, Thompson WM Jr, Dalton ML. Ectopic thyroid. Ann Thorac Surg. 2003;75(6):1952–3.
de Perrot M, Fadel E, Mercier O, Farhamand P, Fabre D, Mussot S, et al. Surgical management of mediastinal goiters: when is a sternotomy required? Thorac Cardiovasc Surg. 2007;55(1):39–43.
Rives JD. Mediastinal Aberrant Goiter. Ann Surg. 1947;126(5):797–810.
Wu CW, Dionigi G, Lee KW, Hsiao PJ, Paul Shin MC, Tsai KB, et al. Calcifications in thyroid nodules identified on preoperative computed tomography: patterns and clinical significance. Surgery. 2012;151(3):464–70.
Kahara T, Ichikawa T, Taniguchi H, Shinnou H, Sumiya H, Uchiyama A, et al. Mediastinal thyroid goiter with no accumulation on scintigraphy. Intern Med. 2013;52(18):2159.
Page C, Strunski V. Cervicothoracic goiter: an anatomical or radiological definition? Report of 223 surgical cases. J Laryngol Otol. 2007;121(11):1083–7.
Ozturk A, Cicek T, Aktas Z, Demirag F, Yilmaz A. Mediastinal ectopic thyroid diagnosed by endobronchial ultrasound-guided transbronchial needle aspiration: report of three cases. J Clin Ultrasound. 2018;46(4):299–301.
Pandey V, Reis M, Zhou Y. Correlation between computed tomography density and functional status of the thyroid gland. J Comput Assist Tomogr. 2016;40(2):316–9.
Glazer GM, Axel L, Moss AA. CT diagnosis of mediastinal thyroid. AJR Am J Roentgenol. 1982;138(3):495–8.
Li X, Han X, Sun W, Wang M, Jing G, Zhang X. Preoperative misdiagnosis analysis and accurate distinguish intrathymic cyst from small thymoma on computed tomography. J Thorac Dis. 2016;8(8):2086–92.
Vadasz P, Kotsis L. Surgical aspects of 175 mediastinal goiters. Eur J Cardiothorac Surg. 1998;14(4):393–7.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
MS contributed towards the conceptualization of the study, project administration, visualization, writing–original draft, writing, reviewing, and editing. HH contributed towards supervision, writing, reviewing, and editing. AN contributed towards data curation. RS contributed towards data curation, writing, reviewing, and editing. TS contributed towards data curation, writing, reviewing, and editing. MH contributed towards writing, review, and editing. TH contributed towards data curation, writing, reviewing, and editing. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All clinical practices were conducted in accordance with the principles of the Declaration of Helsinki.
Consent for publication
Informed consent for publication was obtained from the patient.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Suzuki, M., Horio, H., Nakamura, A. et al. Mediastinal aberrant goiter characterized by high radiodensity on non-enhanced computed tomography: a case report. Gen Thorac Cardiovasc Surg Cases 1, 6 (2022). https://doi.org/10.1186/s44215-022-00004-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s44215-022-00004-3