
Abstract
Background
Sepsis-3 emphasizes the recognition of sepsis-induced cellular metabolic abnormalities, and utilizes serum lactate level as a biomarker of cellular metabolic abnormalities. Magnesium plays an important role as a cofactor in glucose metabolism, although it is not well known that magnesium deficiency causes elevated serum lactate levels. Additionally, it remains unclear how magnesium status affects the role of serum lactate levels as a marker of metabolic abnormalities in sepsis. Thus, this study aimed to investigate the association between serum magnesium and lactate levels in patients with sepsis and explore this relationship from the perspectives of time course and circulatory abnormalities.
Methods
This retrospective observational study of adult patients with sepsis was performed at the 16-bed intensive care unit of Jichi Medical University Hospital between June 2011 and December 2017. The relationship between serum magnesium and lactate levels for 5 days from intensive care unit admission was investigated along the time course. Multivariate logistic regression analysis was performed to evaluate the association between serum magnesium and lactate levels during intensive care unit admission.
Results
Among 759 patients included, 105 had hypomagnesemia (magnesium level < 1.6 mg/dL), 558 had normal serum magnesium levels (1.6–2.4 mg/dL), and 96 had hypermagnesemia (magnesium level > 2.4 mg/dL) at intensive care unit admission. From intensive care unit admission to day 5, the hypomagnesemia group had higher serum lactate levels and a higher frequency of lactic acidosis than the normal magnesium level and hypermagnesemia groups (70% vs. 51.6% vs. 50%; P < 0.001). Hypomagnesemia at intensive care unit admission was independently associated with lactic acidosis, i.e., lactic acid level > 2 mmol/L (odds ratio, 2.76; 95% confidence interval, 1.60–4.76; P < 0.001).
Conclusions
Hypomagnesemia was associated with serum lactate levels in the early and post-resuscitation phases of sepsis. Further studies are needed to elucidate whether the magnesium status is associated with sepsis-induced cellular and metabolic abnormalities.
Similar content being viewed by others


Background
Lactate is not just a metabolic product of anaerobic glycolysis, but also has important functions as an oxidative and gluconeogenic substrate and a signaling molecule [1, 2]. Lactate production is accelerated by hypermetabolic states such as sepsis [3]. When glycolysis causes an increase in pyruvate levels beyond the body’s capacity to metabolize it, the serum lactate level increases even in the absence of impaired oxygen transport [3, 4]. Additionally, lactate levels can provide prognostic information about patients with sepsis with and without hypotension [5] or impaired oxygen transport [6]. The European Society of Intensive Care Medicine and Society of Critical Care Medicine defined septic shock in the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) as a subset of sepsis that includes cellular and metabolic abnormalities with a serum lactate level of > 2 mmol/L in addition to circulatory abnormalities with persisting hypotension [7]. Thus, an elevated lactate level has significance as a marker of metabolic abnormalities in sepsis.
Magnesium (Mg) acts as a cofactor in several essential biochemical enzymatic reactions (such as nucleic acid and protein synthesis) and has a role in immune modulation [8, 9]. Mg is also associated with glycolysis and the tricarboxylic acid (TCA) cycle in intracellular glucose metabolism [10, 11]. Mg plays a role as a cofactor in the conversion of thiamine to thiamine pyrophosphate (TPP), which binds pyruvate dehydrogenase and converts pyruvate to acetyl coenzyme A [12]. Thus, Mg deficiency alters the metabolism of pyruvate to acetyl coenzyme A, resulting in increased lactate production [11,12,13,14] (eFigure 1, Additional file 1).
Hypomagnesemia (HypoMg) has been frequently identified [15, 16] and is associated with increased mortality in critically ill patients [17]. In our previous study on the association between HypoMg and disseminated intravascular coagulation in patients with sepsis, we found that patients with HypoMg upon intensive care unit (ICU) admission had higher serum lactate levels and frequency of septic shock than those with normomagnesemia (NormoMg) [18]. Additionally, HypoMg on admission was associated with lactic acidosis [15] and septic shock [19] in critically ill patients, and Mg supplementation improved serum lactate clearance in patients with sepsis presenting with NormoMg and without hypotension [20]. If the Mg status is associated with serum lactate as a biomarker of sepsis-induced cellular metabolic abnormalities, then the unknown association between Mg status and serum lactate levels could mislead physicians in the diagnosis and treatment of sepsis. However, no previous study has examined the relationship between serum magnesium and lactate levels in sepsis after the day of ICU admission. Thus, the manner in which serum Mg levels affect the pathophysiology of lactic acidosis in sepsis, including time phase and patient population, remains unclear.
To analyze in detail the findings of our previous study [18] in detail, the present was designed to retrospectively investigate the relationship between serum Mg and lactate levels from ICU admission to day 5 in patients with sepsis and additionally explore these relationships from the perspectives of time course, lactate clearance, and circulatory abnormalities.
Methods
Study design and data collection
This was a single-center, retrospective, and observational study of adult patients with sepsis in the 16-bed ICU of Jichi Medical University Hospital, Tochigi, Japan, between June 2011 and December 2017. In our previous study, we retrospectively assembled data from electronic medical records of adult patients (≥ 20 years) who met the Sepsis-3 definition [7] and were admitted to the ICU and created a dataset to analyze the association between HypoMg and coagulopathy [18]. The same dataset was used in this study. We excluded patients who were readmitted to the ICU and those whose data on serum Mg or lactate levels on the day of ICU admission were unavailable for analysis. This study was approved by the Jichi Medical University Hospital Bioethics Committee for Clinical Research (approval number: 21–034, date of approval: October 1, 2021). The procedures followed were in accordance with the ethical standards of the committee on human experimentation and Helsinki Declaration of 1975. The institutional ethics committee waived the need for informed consent due to the retrospective nature of the study.
Lactic acidosis, lactate clearance, septic shock, and serum Mg level
Lactic acidosis was defined according to the criteria for septic shock in Sepsis-3 and in previous studies as follows: lactic acidosis (serum lactate level > 2 mmol/L) and severe lactic acidosis (serum lactate level > 4 mmol/L) [15, 21, 22]. Lactate clearance is the percentage reduction in lactate levels from ICU admission to the time of measurement. Lactate clearance on measurement was calculated using the following formula: (lactate level at ICU admission-lactate on measurement) × 100/lactate level at ICU admission (%) [22]. According to Sepsis-3, septic shock was clinically defined as sepsis with persisting hypotension, requiring vasopressors to maintain an MAP of ≥ 65 mmHg and a serum lactate level > 2 mmol/L (18 mg/dL) despite adequate volume resuscitation [7].
The frequency of lactic acidosis according to the deciles of the serum Mg level at ICU admission demonstrated a J-shaped curve (eFigure 2, Additional file 1). Thus, we categorized the serum Mg level into three groups using the definition in other studies on Mg [15, 23, 24]: HypoMg (Mg level < 1.6 mg/dL), NormoMg (1.6–2.4 mg/dL), and HyperMg (Mg level > 2.4 mg/dL). Similar to our previous study [18], based on the presence of HypoMg on days 2 and 3, we categorized patients with HypoMg on the day of ICU admission into two groups: persistent HypoMg (Mg level < 1.6 mg/dL) and resolved HypoMg (Mg level ≥ 1.6 mg/dL). Additionally, patients without HypoMg at ICU admission were divided into two groups: developed HypoMg (Mg level < 1.6 mg/dL) and non-HypoMg (Mg level ≥ 1.6 mg/dL).
Statistical analyses
We present the data as medians with interquartile ranges for continuous variables and as counts with percentages for categorical variables. We compared the data in two or three groups according to serum Mg levels using the Mann–Whitney U and Kruskal–Wallis tests for continuous variables and the chi-square and Fisher’s exact test for categorical variables. When there were statistically significant differences among the three groups according to serum Mg levels, the Steel–Dwass test, chi-square test, or Fisher’s exact test with the Bonferroni correction was performed to determine significance in the setting of multiple comparisons. To examine the association between serum Mg and lactate levels with and without hypotension, subgroup analyses were performed according to the presence or absence of the need for vasopressors to maintain an MAP of ≥ 65 mmHg. Univariate and multivariate logistic regression analyses were performed to determine independent associations between serum Mg levels and lactic acidosis in complete case analyses. From amongst the variables extracted from our previous study [18], age, chronic comorbidities such as chronic live disease, blood pressure, vasopressor use, respiratory dysfunction, serum creatinine, platelet count, prothrombin time, and severity were considered to be potentially related to lactic acidosis in previous studies [15, 25,26,27]. We included age, chronic comorbidities, blood pressure, respiratory dysfunction, and serum creatinine as a single summary score, viz. the Acute Physiology and Chronic Health Evaluation (APACHE) II score rather than individual variables. Moreover, we added sex; an inflammatory biomarker, viz. C-reactive protein level; and an electrolyte, viz. ionized calcium level as covariates in the multivariate logistic regression models. In model 1, no adjustments were made. Model 2 was adjusted for sex and the APACHE II score. Model 3 was additionally adjusted for the need for vasopressors to maintain an MAP of ≥ 65 mmHg, C-reactive protein level, ionized calcium level, platelet count, and prothrombin time-international normalized ratio. All data were analyzed using JMP pro (version 16. 1. 0) software (SAS Institute Inc., Cary, NC, USA) and R package (version 4.0.4, R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at P < 0.05.
Results
Patient characteristics
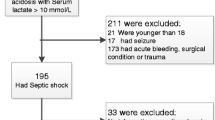
During the study period, 830 patients with sepsis were admitted to the ICU. In total, 71 patients were excluded from this study—60 with missing data at the time of ICU admission and 11 who were readmitted to the ICU. Therefore, based on serum Mg levels on ICU admission, i.e., day 1, 759 patients were eligible for data analysis, with 105, 558, and 96 patients having HypoMg, NormoMg, and hypermagnesemia (HyperMg), respectively (Fig. 1). Table 1 shows the baseline characteristics of the 759 patients categorized into the HypoMg, NormoMg, and HyperMg groups. Compared with the NormoMg and HyperMg groups, the HypoMg group had higher serum lactate levels (median: 3.9 vs. 2.1, P < 0.01; 3.9 vs. 2.1, P < 0.01, respectively) and more patients with septic shock (70.5% vs. 40.1%., P < 0.01; 70.5% vs. 42.7%., P < 0.01, respectively). However, there were no differences in the frequency of the need for vasopressors to maintain a mean arterial pressure (MAP) of ≥ 65 mmHg on the ICU admission day among the three groups. The HypoMg group had a higher disease severity (median Acute Physiology and Chronic Health Evaluation [APACHE] II score: 25 vs. 23; P < 0.01) and hospital mortality (25.7% vs. 14.3%; P < 0.05) than the NormoMg group. However, there were no differences in disease severity and hospital mortality between the HypoMg and HyperMg groups.

Flow chart of participant enrollment
Comparison of serum lactate levels according to serum Mg levels from ICU admission to day 5
Although 759 patients were included in the study, the serum lactate and Mg levels until day 5 were not available for 215 patients, among whom 32 died, 159 were discharged from the ICU, and 24 had missing data. The serum lactate level and frequency of lactic acidosis decreased gradually from admission to day 4. The HypoMg group had higher serum lactate levels and more patients with lactic acidosis than the NormoMg group from admission to day 5 and HyperMg group from admission to day 2 (Table 2).
Comparison of serum lactate parameters between the persistent and resolved HypoMg groups
In total, 105 patients with HypoMg at ICU admission were divided into the persistent HypoMg group (on day 2, N = 68; on day 3, N = 35) and resolved HypoMg group (on day 2, N = 33; on day 3, N = 64) according to their serum Mg levels on days 2 and 3. There was no difference in the serum lactate level or frequency of lactic acidosis between the groups on days 2 and 3. The resolved HypoMg group had higher lactic clearance than the persistent HypoMg group on day 3 (51.9% vs. 34.6%, P = 0.027) (Table 3).
Comparison of serum lactate parameters between the developed and non- HypoMg groups
In total, 654 patients without HypoMg at ICU admission were divided into the developed HypoMg group (on day 2, N = 37; on day 3, N = 28) and non-HypoMg group (on day 2, N = 586; on day 3, N = 553) according to their serum Mg levels on days 2 and 3. The group that developed HypoMg on day 2 or 3 had higher serum lactate levels, frequency of lactic acidosis, and serum lactate levels at ICU admission before developing HypoMg than the non-HypoMg group (Table 4).
Subgroup analysis
The group that required vasopressors to maintain an MAP of ≥ 65 mmHg had higher lactate levels, disease severity, and mortality (eTable 1, Additional file 1) than the group that did not. Patients with HypoMg had higher lactate levels and more frequent lactic acidosis than those with NormoMg and HyperMg in the subgroup that required vasopressors to maintain an MAP of ≥ 65 mmHg but not in the subgroup that did not require vasopressors (eTables 2 and 3, Additional files 1).
Logistic regression analysis of factors associated with lactic acidosis
In the unadjusted analysis (model 1), the HypoMg group had increased odds of developing lactic acidosis (odds ratio [OR], 3.75; 95% confidence interval [CI], 2.26–6.22; P < 0.001) compared with the NormoMg group. This relationship remained highly significant after adjusting for disease severity and the need for vasopressors to maintain an MAP of ≥ 65 mmHg in models 2 and 3 (Table 5).
Discussion
Our retrospective observational study aimed to determine whether serum Mg levels were associated with serum lactate levels in patients with sepsis and if so, in which phase and in which specific population. The HypoMg group had high serum lactate levels and included many patients with lactic acidosis from ICU admission to day 5, and the patients who newly developed HypoMg on days 2 and 3 had high serum lactate levels. Subgroup analysis showed that HypoMg was associated with increased serum lactate levels in patients who required vasopressors to maintain an MAP of ≥ 65 mmHg but not in those who did not. These findings indicate that HypoMg is associated with lactic acid metabolism from the early resuscitation to the post-resuscitation phase of sepsis and in hemodynamically unstable patients with sepsis.
Serum lactate levels indicate the balance between the production and consumption of lactate [4]. The former involves glycolysis, and the latter involves the TCA cycle [2]. Accelerated glycolysis produces lactate according to the energy demands of various organs for biological reactions, and this phenomenon is known as sepsis; subsequently, lactate is used as an energy substrate via the TCA cycle for oxidative phosphorylation or gluconeogenesis [1]. As a cofactor, Mg is principally related to various enzymatic activities of glucose metabolism in both glycolysis and the citric acid cycle [11]. Among the various enzymatic reactions, Mg is essential for the activation of pyruvate dehydrogenase, which converts pyruvate to acetyl coenzyme A, via TPP [3, 11, 12]. Although some studies have reported that thiamine may improve the prognosis of sepsis in patients with thiamine deficiency [28], it has not been clearly shown to improve prognosis in sepsis [29]. However, studies have reported that thiamine deficiency is potentially involved in lactic acidosis in patients with sepsis with thiamine deficiency [30, 31]. If pyruvate dehydrogenase activity is impaired, increased glycolysis, especially during sepsis, can easily exceed the capacity of mitochondrial respiration to metabolize pyruvate [3, 4]. Thus, Mg deficiency could impair pyruvate dehydrogenase activity, resulting in elevated lactate levels.
When investigating the association between Mg and lactate, it is important to distinguish between increased lactate levels in the early resuscitation and post-resuscitation phases because hyperlactatemia has different clinical implications in the two phases [3]. Inadequate tissue oxygenation is one of the factors contributing to elevated serum lactate levels, and hemodynamic resuscitation reduces lactate levels in the early resuscitation phase of sepsis. Magnesium has also been implicated in the cardiac conduction as an essential cofactor of the Na–K-ATP pump, and Mg status therefore influences myocardial excitability [10, 32]. Magnesium deficiency is a risk for arrhythmias such as atrial fibrillation [9, 10, 32], which may result in hemodynamical instability and elevated serum lactate levels. However, persistently elevated serum lactate levels in the post-resuscitation phase often occur independently of whole-body oxygen delivery; therefore, causes of hyperlactatemia other than inadequate whole-body oxygen delivery must be considered [3, 4]. Our findings demonstrated that HypoMg was associated more strongly with high lactate levels than NormoMg even in the post-resuscitation phase when the lactate levels decreased (days 2–5). This result may support the hypothesis that the theoretical mechanism underlying the association between HypoMg and increased lactate level is impaired pyruvate dehydrogenase and not inadequate oxygen delivery.
Mild hyperlactatemia in hemodynamically stable patients with sepsis is due to impaired lactate clearance rather than lactate overproduction [33]. We also showed that hypomagnesemia was associated with serum lactate levels in the subgroup that required vasopressors to maintain an MAP of ≥ 65 mmHg but not in the subgroup that did not require vasopressors. However, the sample size of the subgroup that did not require vasopressors might be too small for evaluation. The subgroup that did not require vasopressors to maintain an MAP of ≥ 65 mmHg had lower serum lactate levels (median: 1.6 mmol/L) and less frequent lactic acidosis (31.3%) than the subgroup that required vasopressors. These findings suggest that Mg is relevant to lactate production rather than lactate clearance. Thus, in situations of increased glycolytic flux during sepsis, HypoMg may reduce mitochondrial oxidative capacity, causing hyperlactatemia.
Intracellular Mg is associated with glucose metabolism but not with serum Mg levels. Although hypomagnesemia is not a good indicator of Mg deficiency [34], Mg deficiency is usually detected due to refractory HypoMg because there is no simple or rapid test to measure intracellular and total body Mg levels [8]. Our study demonstrated that HypoMg and its development are associated with increased serum lactate levels. Interestingly, the developed HypoMg group already had significantly higher serum lactate levels before onset than the non- HypoMg group. Compared with the persistent HypoMg group, the resolved HypoMg group did not show significant improvements in lactic acidosis, even with improvement in HypoMg. These findings indicate that the developed or resolved HypoMg group may have occult intracellular Mg deficiency. To assess the relationship between Mg deficiency and various metabolic reactions, a simple method for measuring intracellular or total body Mg levels must be established. Further studies are required to clarify the mechanism underlying the relationship between Mg and lactate levels and whether treatment of HypoMg may be a potential therapeutic strategy for hyperlactatemia.
Our study had some limitations. First, this was a single-center, retrospective, and observational study. Because of the retrospective nature of this study, data on serum lactate and Mg levels from admission to day 5 in approximately 30% of the included patients were not available due to death or ICU discharge; the number of patients with missing data among the 759 patients included in this study was as follows: 36 (4.7%) on day 2, 80 (10.5%) on day 3, 147 (19.4%) on day 4, and 213 (28.0%) on day 5. Hence, selection bias could have occurred. Due to the large number of patients with missing data on days 4 and 5, we investigated serum lactate only for each change in serum Mg status from ICU admission to days 2 and 3. Second, we did not investigate the baseline Mg profile before sepsis (Mg deficiency or HypoMg), nutritional status (reduced intake or Mg supplementation), cause of Mg deficiency or HypoMg such as comorbidities (gastrointestinal and renal loss) and drug usage (diuretics and proton-pump inhibitor) [32]. Third, there was a lack of information on factors that may affect serum Mg levels during ICU stay, such as Mg administration, diuretics, and dialysis. Fourth, we did not evaluate the mechanism underlying the association between Mg and lactate because we did not investigate glycolysis and oxidative phosphorylation of intracellular metabolic processes through thiamine-dependent reactions.
Conclusion
We demonstrated that HypoMg was associated with lactic acidosis during the early and post-resuscitation phases of sepsis, especially in hemodynamically unstable patients with sepsis. However, it is unknown whether Mg status is associated with the pathophysiology of sepsis-induced cellular and metabolic abnormalities. Further studies are needed to elucidate the mechanism underlying the relationship between Mg status and lactate levels in sepsis and whether Mg is associated with sepsis-induced cellular and metabolic abnormalities.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available because of patient-related confidentiality.
Abbreviations
- ICU:
-
Intensive care unit
- Mg:
-
Magnesium
- TCA:
-
Tricarboxylic acid cycle
- TPP:
-
Thiamine pyrophosphate
- MAP:
-
Mean arterial pressure
- APACHE:
-
Acute Physiology and Chronic Health Evaluation
- HypoMg:
-
Hypomagnesemia
- NormoMg:
-
Normomagnesemia
- HyperMg:
-
Hypermagnesemia
References
Brooks GA (2018) The science and translation of lactate shuttle theory. Cell Metab 27:757–785
Li X, Yang Y, Zhang B et al (2022) Lactate metabolism in human health and disease. Signal Transduct Target Ther 7:305
Suetrong B, Walley KR (2016) Lactic acidosis in sepsis: it’s not all anaerobic: implications for diagnosis and management. Chest 149:252–261
Vincent JL, Bakker J (2021) Blood lactate levels in sepsis: in 8 questions. Curr Opin Crit Care 27:298–302
Howell MD, Donnino M, Clardy P et al (2007) Occult hypoperfusion and mortality in patients with suspected infection. Intensive Care Med 33:1892–1899
Gattinoni L, Vasques F, Camporota L et al (2019) Understanding lactatemia in human sepsis. potential impact for early management. Am J Respir Crit Care Med 200:582–589
Singer M, Deutschman CS, Seymour CW et al (2016) The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 315:801–810
de Baaij JHF, Hoenderop JGJ, Bindels RJM (2015) Magnesium in man: implications for health and disease. Physiol Rev 95:1–46
Jahnen-Dechent W, Ketteler M (2012) Magnesium basics Clin Kidney J 5:i3–i14
Gröber U, Schmidt J, Kisters K (2015) Magnesium in prevention and therapy. Nutrients 7:8199–8226
Pilchova I, Klacanova K, Tatarkova Z et al (2017) The involvement of Mg2+ in regulation of cellular and mitochondrial functions. Oxid Med Cell Longev 2017:6797460
Attaluri P, Castillo A, Edriss H et al (2018) Thiamine deficiency: an important consideration in critically ill patients. Am J Med Sci 356:382–390
Maguire D, Catchpole A, Sheerins O et al (2021) The relation between acute changes in the systemic inflammatory response and circulating thiamine and magnesium concentrations after elective knee arthroplasty. Sci Rep 11:11271
Maguire D, Burns A, Talwar D et al (2022) Randomised trial of intravenous thiamine and/or magnesium sulphate administration on erythrocyte transketolase activity, lactate concentrations and alcohol withdrawal scores. Sci Rep 12:6941
Moskowitz A, Lee J, Donnino MW et al (2016) The association between admission magnesium concentrations and lactic acidosis in critical illness. J Intensive Care Med 31:187–192
Escuela MP, Guerra M, Añón JM et al (2005) Total and ionized serum magnesium in critically ill patients. Intensive Care Med 31:151–156
Jiang P, Lv Q, Lai T et al (2017) Does hypomagnesemia impact on the outcome of patients admitted to the intensive care unit? A systematic review and meta-analysis. Shock 47:288–295
Tonai K, Katayama S, Koyama K et al (2022) Association between hypomagnesemia and coagulopathy in sepsis: a retrospective observational study. BMC Anesthesiol 22:359
Thongprayoon C, Cheungpasitporn W, Erickson SB (2015) Admission hypomagnesemia linked to septic shock in patients with systemic inflammatory response syndrome. Ren Fail 37:1518–1521
Noormandi A, Khalili H, Mohammadi M et al (2020) Effect of magnesium supplementation on lactate clearance in critically ill patients with severe sepsis: a randomized clinical trial. Eur J Clin Pharmacol 76:175–184
Silva CM, Baptista JP, Mergulhão P et al (2022) Prognostic value of hyperlactatemia in infected patients admitted to intensive care units: a multicenter study. Rev Bras Ter Intensiva 34:154–162
Ryoo SM, Lee J, Lee YS et al (2018) Lactate level versus lactate clearance for predicting mortality in patients with septic shock defined by Sepsis-3. Crit Care Med 46:e489–e495
Kraft MD, Btaiche IF, Sacks GS et al (2005) Treatment of electrolyte disorders in adult patients in the intensive care unit. Am J Health Syst Pharm 62:1663–1682
Tazmini K, Nymo SH, Louch WE et al (2019) Electrolyte imbalances in an unselected population in an emergency department: a retrospective cohort study. PLoS ONE 14:e0215673
Green JP, Berger T, Garg N et al (2012) Hyperlactatemia affects the association of hyperglycemia with mortality in nondiabetic adults with sepsis. Acad Emerg Med 19:1268–1275
Pattharanitima P, Thongprayoon C, Kaewput W et al (2021) Machine learning prediction models for mortality in intensive care unit patients with lactic acidosis. J Clin Med 10:5021
Filho RR, Rocha LL, Corrêa TD et al (2016) Blood lactate levels cutoff and mortality prediction in sepsis-time for a reappraisal? A retrospective cohort study. Shock 46:480–485
Vine J, Lee JH, Kravitz MS, Grossestreuer AV et al (2024) Thiamine administration in septic shock: a post hoc analysis of two randomized trials. Crit Care 28(1):41
Fujii T, Salanti G, Belletti A, Bellomo R, Carr A, Furukawa TA et al (2022) Effect of adjunctive vitamin C, glucocorticoids, and vitamin B1 on longer-term mortality in adults with sepsis or septic shock: a systematic review and a component network meta-analysis. Intensive Care Med 48(1):16–24
Donnino MW, Carney E, Cocchi MN et al (2010) Thiamine deficiency in critically ill patients with sepsis. Journal Crit Care 25(4):576–581
Ricci Z, Romagnoli S (2018) The 11th pitfall: thiamine deficiency. Intensive Care Med 44(9):1597
Hansen BA, Bruserud Ø (2018) Hypomagnesemia in critically ill patients. J Intensive Care 6:21
Levraut J, Ciebiera JP, Chave S et al (1998) Mild hyperlactatemia in stable septic patients is due to impaired lactate clearance rather than overproduction. Am J Respir Crit Care Med 157:1021–1026
Huijgen HJ, Soesan M, Sanders R et al (2000) Magnesium levels in critically ill patients. What should we measure? Am J Clin Pathol 114:688–695
Acknowledgements
Not applicable.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Contributions
KT and SK conceptualized and designed the study and acquired, analyzed, and interpreted the data. KT drafted and revised the manuscript. SK, KK, HI, and SN critically reviewed the manuscript. SN supervised the study and revised the manuscript. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Jichi Medical University Hospital Bioethics Committee for Clinical Research (approval number: 21–034, date of approval: October 1, 2021). The procedures followed were in accordance with the ethical standards of the committee on human experimentation and Helsinki Declaration of 1975. The institutional ethics committee waived the need for informed consent due to the retrospective nature of the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tonai, K., Katayama, S., Koyama, K. et al. Association between hypomagnesemia and serum lactate levels in patients with sepsis: a retrospective observational study. J Anesth Analg Crit Care 4, 23 (2024). https://doi.org/10.1186/s44158-024-00158-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s44158-024-00158-2