
Abstract
Background
We carry out a retrospective observational analysis of clinical records of patients with major placenta praevia who underwent cesarean section surgery over a period of 20 months in our hospital. Out of a total of 40 patients, 20 were subjected to Goal-Directed Therapy (GDT) implemented with non-invasive hemodynamic monitoring using the EV1000 ClearSight system (Group I) and 20 to standard hemodynamic monitoring (Group II). Given the risk of conspicuous blood loss, this study evaluate the impact on maternal and fetal health of GDT relative to standard hemodynamic monitoring.
Results
Average total infusion of fluids was 1600 +/− 350 ml. Use of blood products occurred in 29 patients (72,5%), of which 11 had a hysterectomy and 8 were treated with Bakri Balloons. For 2 patients > 1000 mL of concentrated red blood cells were used. When stroke volume index SVI dropped below 35 mL/m2/beat, it responded well to the infusion of at least 2 crystalloid boluses (5 ml/kg) in 7 patients. Cardiac index (CI) increased in 8 patients in concomitance with a reduction in medium arterial pressure (MAP), but the use of ephedrine (10 mg iv) re-established acceptable baseline values. Group I means are higher than Group II means for MAP, lower for RBC usage, end-of-surgery maternal lactates and fetal pH, and for LOS. Statistical analysis determines that the null hypotheses of equalities between Groups I and II can be rejected for all measures apart from MAP at baseline and induction. Proportions of serious complications in Groups I and II are respectively 10% and 32% and Boschloo’s test rejects the null of equality of proportions against the alternative hypothesis of lower proportion of occurrence in Group I than in Group II.
Conclusions
Hypovolemia can lead to vasoconstriction and inadequate perfusion with decreased oxygen delivery to organs and peripheral tissues and ultimately cause organ dysfunction. Despite the small sample size due to the rarity of the pathology, our statistical analysis finds evidence in favor of more favorable clinical outcomes for patients who received GDT implemented with non-invasive hemodynamic monitoring infusion relative to patients who received standard hemodynamic monitoring.
Similar content being viewed by others

Background
According to the Royal College of Obstetricians and Gynecologists (RCOG) classification, [1] Placenta Praevia (PP) is classified as major if it completely covers the Internal Uterine Orifice (IUO). Placenta Accreta (PA) describes situations in which the placenta is pathologically adherent to the uterus due to a lack of decidual layer, leading to an invasion of the myometrium by the chorionic villi [1]. The PA is classified according to the depth of myometrial invasion. Placenta Increta describes cases in which chorionic villi invade the full thickness of the myometrium; Placenta Percreta describes instead cases in which chorionic villi’s invasion reaches the serosa and may involve adjacent organs such as the bladder. Incidence is challenging to determine because diagnosis depends in part on the prevalence of cesarean sections, but it is currently estimated at 2/1000 of pregnancies [1,2,3].
In patients suffering from this type of pathology, which makes delivery by cesarean section essential, massive blood losses (i.e., greater than 1000 ml) are not unusual, and patients frequently require intra- and sometimes perioperative blood transfusions. This makes fast, reliable and easy to use hemodynamic monitoring potentially valuable [4].
Improvement in patient outcomes has become a significant concern in surgical settings and the use of Goal-Directed Fluid Therapy (GDT) is gaining acceptance for appropriate perioperative fluid/volume management because it is essential for the success of Early Recovery After Surgery (ERAS) protocols. While rarely used in obstetrician surgery, GDT monitoring may be valuable with abnormal placenta implantation. GDT relies on hemodynamic optimization, as fluid titration, inotropes administration, or blood transfusions, to achieve optimal oxygen delivery to tissues. Perioperative fluid overload may cause acidosis, coagulopathy, tissue, and pulmonary edema, while hypovolemia may lead to hypoperfusion, tissue hypoxia, and oxygen debt. It is well known that Mean Artery Pressure (MAP) and Heart Rate (HR) remain stable even with variations of up to 30% of total blood volume and therefore they cannot provide reliable guidelines for fluid therapy. But fluid GDT based on different parameters may improve perioperative outcomes [4,5,6,7].
In early 2018, in our hospital a multi-specialist team of gynecologists, radiologists, neonatologists, and anesthesiologists initiated discussion of the development of a standardized diagnostic and therapeutic pathway. This led to a quality of care improvement initiative evaluating the efficacy of a GDT protocol for eligible patients.
The EV1000 ClearSight system enables fundamental advanced hemodynamic parameters combined with continuous non-invasive blood pressure monitoring thanks to a non-invasive finger cuff. Continuous monitoring of advanced hemodynamic parameters like cardiac index (CI), stroke volume (SV), stroke volume variation (SVV), systemic vascular resistance (SVR), and medium blood pressure (MBP) was performed. The non-invasive hemodynamic monitoring made possible by the EV1000 ClearSight system provides data that allow to proactively make clinical decisions throughout the care process, from moderate to high-risk surgical patients, and can also be used in the perioperative phase to manage clinical situations of patients in constant evolution [8,9,10,11,12].
Aims
The main objective of our study is to assess the benefits of the implementation of a perioperative emo-component utilization and the utility of Goal-Directed Therapy in terms of length of hospital stay, end-of-surgery lactate values and fetal pH, and postoperative complications.
This article contains new scientific contributions compared to any previously published articles on a similar topic as this is the first time that the benefit of non-invasive hemodynamic monitoring in pregnant women with obstetric pathology has been analyzed.
Materials and methods
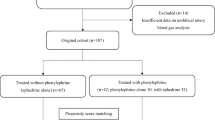
A retrospective observational study was carried out collecting and examining the medical records of patients affected by abnormal placental implantation treated between April 2019 and December 2020 in the Obstetrics and Gynecology Unit of the Hospital “A. Cardarelli” (Naples, Italy).
This study was conducted following the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for reporting observational studies [13].
This study was approved by the local ethics committee (approval number 174 – February 2, 2022) and it was in accordance with the Declaration of Helsinki [14]. An informed consent was signed for each patient.
Inclusion criteria
-
1.
Abnormal placental implantation with signs of placental accretism major;
-
2.
Planned cesarean section procedure;
-
3.
Age of patients between 28 and 42 years old;
-
4.
American Society of Anesthesiology (ASA) Class I or II;
-
5.
Hemoglobin > 11 g/dl.
Exclusion criteria
-
1.
Pathologies or comorbidities that could interfere with the coagulation structure.
A total of 40 medical records were examined. At the time of cesarean section surgery, patients were subjected to either standard hemodynamic monitoring or to GDT implemented with non-invasive hemodynamic monitoring using the EV1000 ClearSight system. Out of the total of 40 patients, 20 had been subjected to additional monitoring with the EV1000 ClearSight system. This occurred when the anesthesiologist on duty had adequate experience with the system and when the appropriate size (Small, Medium or Large) of the disposable sensor with dedicated cuff suitable was available.
Depending on the hemodynamic monitoring system employed during the procedure we label patients as follows:
-
Group I: Patients subjected to standard hemodynamic monitoring together with non-invasive hemodynamic monitoring with the EV1000 ClearSight system;
-
Group II: Patients subjected to standard hemodynamic monitoring.
Procedure
The protocol for procedure and data collection that was followed is outlined below:
-
Entry of the patient into the operating room.
-
Cannulation of 2 large-caliber peripheral vessels.
-
Monitoring of basic vital parameters: consciousness, continuous ECG (electrocardiographic trace in DII), HR (heart rate), oximetry, respiratory rate, temperature, diuresis, and metabolic structure: blood gas analysis (BGA) with the determination of maternal lactate at least at the end of the surgery, fetal pH, intraoperative fluids, transfusion of blood components.
-
Hemodynamic monitoring. Either of the following:
-
Non-invasive hemodynamic monitoring by EV1000 ClearSight system of:
-
Direct parameters: cardiac index (CI), mean arterial pressure (MAP), stroke volume index (SVI) (or stroke volume variation (SVV) in patients submitted to general anesthesia);
-
Indirect parameters: O2 demand (DO2) and RSVI.
-
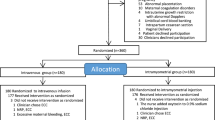
Figure 1 describes the proactive protocol that was followed to correct alterations that occurred during surgery.
-
-
Standard hemodynamic monitoring: continuous ECG, heart rate and systolic/diastolic blood pressure. In this group, hypotension was corrected with fluid bolus therapy until blood pressure normalization.
-
-
Anesthesia:
-
Continuous peridural anesthesia (CPE): For patients with no known contraindications.
-
Blended anesthesia (CPE followed by general anesthesia): For patients when the duration of surgery resulted in poor compliance to CPE alone.
-
General anesthesia: For patients with known absolute or relative contra-indications to loco-regional anesthesia and for some other patients.
-
-
Data collection:
-
Hemodynamic data measurements (CI, SVI, MAP, DO2) and lactates were logged at baseline (T0), induction (T1), post-extraction (T2), intermediate (T3), and end-of-surgery (T4).
-
Body temperatures, diuresis, fluid and blood products administration, fetal pH, complications (such as persistent fever, delayed channeling, mild to severe respiratory failure, wound infection or dehiscence, thrombotic event, etc.), length of hospital stay (LOS) and 30-day hospital readmission.
-

Proactive protocol
Statistical analysis
Statistical analysis was conducted using different statistical tests based on the need to determine the meaning of a value obtained in the whole population or to compare data obtained between treated and untreated patients (Software used R version 4.0.3–2020-10-10; Packages: dplyr, car, one waytests, exact). The outcomes showing departures from normal values were evaluated by Shapiro-Wilk normality test, F-test, Levene’s test, two-sample t-test, Welch two-sample t-test, and Wilcoxon sum test.
The t-test was used to determine the means of two sets of data significantly different from each other. The independent samples t-test is used when two separate sets of independent and identically distributed samples are obtained, one from each of the two populations being compared.
Results
The clinical characteristics of the patients in the two groups are similar: all ASA class I and II patients with placenta previa accreta.
Descriptive statistics for all 40 patients are reported in Table 1. This table reportsm the clinical data recorded during the intervention: the number of bags of concentrated red blood cells used, the fetal pH at birth, the maternal lactates at the end of the intervention, the days of hospitalization. In addition, some events were recorded during the operation or in the postoperative period indicated in the table with appropriate abbreviations: B: bakri balloon, C: coagulation disorder, D: delayed channeling, E: embolization F: fever H: histerectomy M: mild respiratory failure S: severe respiratory failure V: vascular access thrombosis W: wound dehiscence. Of these events, only those that caused complications in the postoperative period were considered and indicated with a score of 1.
The patients treated with continuous epidural anesthesia were 32. Only one patient received general anesthesia (being in treatment with high doses of heparin and being operated in an emergency regime). Seven patients received blended anesthesia (continuous epidural anesthesia and subsequent general anesthesia) when the duration of surgery resulted in poor compliance to continued epidural anesthesia alone. Average duration of procedures was 115 ± 35 minutes.
The MAP remained > 50 mmHg in most patients, in fact only two patients in group I and two patients in group 2 had a MAP < 50 mmHg after placental extraction. Total infusion of fluids was on average 1600 ± 350 ml.
For 3 patients (7.5%), bleeding was quickly controlled after the extraction of the placenta, and no containment maneuvers were necessary. For 8 patients (20%) placing a Bakri Balloon was necessary to control uterine bleeding. For 11 patients (27.5%) hysterectomy was practiced to stop bleeding. Finally, for 7 patients (17.5%), an interventional radiologist was required for selective embolization of uterine arteries. In all patients, blood losses were greater than 1500 ml.
Use of blood products occurred in 28 patients (72.5%): 12 in Group I and 16 in Group II. Ten patients received more than 2 units of blood units (25%), 3 in Group I (15%) and 7 in Group II (35%). Only 2 patients (5%) received > 1000 mL of concentrated red blood cells. Hysterectomy was necessary for a total of 11 patients, of which 5 in Group I (25%) and 6 in Group II (30%).
Fetal pH was 7.31 ± 0.04 in Group I and 7.30 ± 0.03 in Group II. At the end of surgery patients had 0.96 ± 0.41 lactates, while maternal lactates were 1.23 ± 0.33 in Group II.
72.5% of patients were discharged within 7 days. Postoperative length of hospital stay was between 7 and 9 days for 11 patients (4 in Group I versus 7 in Group II): 3 patients with thrombocytopenia or other coagulation factors defects, 1 patient with thrombotic complication after femoral artery cannulation, and 7 patients who required intensive postoperative care. Serious perioperative complications occurred 9 times, of which 7 in Group II.
The clearsight hemodynamic monitoring data recorded in the patients of Group I were collected in Tables 2, 3, 4 and represented in Figs. 2, 3, 4. The hemodynamic values were promptly corrected by recording alterations of the parameters for short periods of time with consequent maintenance of an adequate perfusion during all phases of the surgery, even the most critical.

Group I Patients Cardiac Indices (CI), T0-T4

Group I Patients Stroke Volume Indices (SVI), T0-T4

Group I Patients Oxygen Delivery (O2D), T0-T4
The SVI dropped below 35 mL/m2/beat in 7 patients (35%), but it responded well to the infusion of at least two crystalloid boluses (5 ml/kg); and the CI in 8 patients (40%) increased with a reduction in MBP, but the use of ephedrine (10 mg iv) re-established acceptable baseline levels.
All recorded data were subjected to statistical analysis to assess their significance. The statistical analysis of the results (through two simple t-tests at the usual confidence intervals) gave significant results as regards the maintenance of adequate blood pressure values in the times T3 (p-value 0.002), T4 (p-value 0.002) and T5 (p-value 0.001) and also of the lactate value at the end of surgery (p-value 0.025).
One side test where the null is rejected at the usual confidence level (0.05) for blood unit (p-value = 0.0318). Through Boschloo’s test, the data examined the association of two Bernoulli distributed random variables, which is a uniformly more powerful alternative to Fisher’s exact test for postoperative complications. Indeed true differences in proportions of occurrence of treated versus untreated are less than 0 for postoperative complications (p-value 0.04) and consequently of the length of hospital stay (p-value 0.026) in the group of patients undergoing non-invasive monitoring with the EV1000 ClearSight system.
Discussion
The comparison of outcome markers showed a statistically significant reduction between the two groups. The clinical outcome was favorable in patients who received an infusion of goal-directed fluids and were subjected to a proactive protocol with non-invasive hemodynamic monitoring EV1000 ClearSight system. Hypovolemia can lead to vasoconstriction and inadequate perfusion, with decreased oxygen delivery to organs and peripheral tissues, causing organ dysfunction. On the other hand, fluid overload can lead to interstitial edema, local inflammation and likely impair the regeneration of collagen, thus negatively affecting tissue healing while increasing the risk of wound dehiscence, wound infections, and anastomotic leakage. Therefore, maintenance of intravascular good volume throughout the perioperative period is ideal. The principle behind GDT is to maximize tissue oxygen delivery without fluid overload by achieving measurable optimal hemodynamic indices. Surprisingly, the total quantity of infused liquids was not significantly different between the two groups, as it is strongly influenced by the experience of the anesthetist present for this type of intervention.
The difference in the amount of red blood cells used is statistically significant. Periods of intraoperative hypotension were reduced, as was the use of blood products which occurred in less than 50% of patients.
The comparison of outcome markers such as maternal lactates to end-surgery and perioperative complications showed a statistically significant reduction between the two groups.
Only a minimum number of patients had an extension of hospitalization times, and none of the patients had complications or 30-day readmission, splanchnic, hepatological, and renal microcirculation failure.
Hemodynamic stability guarantees adequate tissue generation and a metabolic balance to reduce postoperative complications, whereas the prolongation of the days of hospitalization due to insufficient microcirculation consequents the onset of suture infections, fever, and renal insufficiency [15,16,17,18,19,20,21,22,23]. The presence of statistically significant data regarding the results not affected by the method makes this study interesting. However, only its application in a more substantial number of patients can provide direct results in choosing the most appropriate monitoring.
Perioperative fluid management have received increased interest in recent years [24]. The validity of ClearSight System may depend on the clinical situation such as the type of surgery or the patient’s clinical condition. Several studies have investigated the effectiveness of non-invasive hemodynamic monitoring in various fields, such as vascular surgery [25], cardiac surgery [26], bariatric surgery [27] and neuroendovascular interventions [28]. All concluded that non-invasive hemodynamic monitoring is
a good option for hemodynamic monitoring during induction of anesthesia. The ClearSight system provided accurate measurements of arterial blood pressure compared with invasive methods. In accordance to these studies, it is a safe and reliable alternative for invasive blood pressure monitoring during different surgical procedures. On the other hand, it is not reliable in critically ill patients [29] and patients undergoing neurosurgery in a sitting position [30].
Limitations
The study has a series of limitations related to the small sample in which it was conducted. However, the obstetric pathology of the abnormal placental implant represents a low percentage of obstetric patients. We managed to reach this number of patients by being the reference hospital for the treatment that can be performed by a multidisciplinary team of specialists with various therapeutic options (for example, embolization of the uterine branches with the interventional radiologist, assistance to the premature newborn with the Neonatological Intensive Care, dedicated anesthetist, etc.). Another limitation was represented by the fact that the study was not conducted in a blind matter. However, we only selected patients with similar inclusion criteria precisely to avoid being influenced by the type of monitoring to be used, and the use of the monitoring provided for a one-to-one random selection. The statistical analysis various tests were used in order to have a more reliable confirmation of the data obtained.
Conclusions
Perioperative hemodynamic management based on the evaluation of advanced hemodynamic variables aims at optimizing cardiovascular dynamics to improve the patient’s postoperative outcome.
In our study we had encouraging results in terms of intraoperative hemodynamic management and maternal-fetal outcome. Due to the small study size, further research is needed to evaluate and establish non-invasive hemodynamic monitoring for hemodynamic management during placenta praevia accreta cesarean delivery.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ASA:
-
American Society of Anesthesiology
- BGA:
-
Blood gas analysis
- CI:
-
Cardiac index
- CPE:
-
Continuous peridural anesthesia
- DO2:
-
O2 demand
- ERAS:
-
Early Recovery After Surgery
- GDT:
-
Goal-Directed Fluid Therapy
- HR:
-
Heart Rate
- LOS:
-
Length of hospital stay
- MAP:
-
Mean Artery Pressure
- MBP:
-
Medium blood pressure
- PA:
-
Placenta Accreta
- PP:
-
Placenta Praevia
- RCOG:
-
Royal College of Obstetricians and Gynecologists
- SV:
-
Stroke volume
- SVR:
-
Systemic vascular resistance
- SVV:
-
Stroke volume variation
References
Royal College of Obstetricians and Gynaecologists. Placenta praevia, placenta praevia accrete and vasa previa: diagnosis and management Green-Top Guideline no.27, 2011
Calì G, Giambanco L, Puccio G, Forlani F (2013 Apr) Morbidly adherent placenta: evaluation of ultrasound diagnostic criteria and differentiation of placenta accrete from Percreta. Ultrasound Obstet Gynecol 41(4):406–412
Lilker S, Meyer R, Downey K et al (2011) Considerazioni anestetiche per la placenta accreta. Int J Obstet Anesth 20(4):288–292
Chachula K, Lieb F, Hess F, Welter J, Graf N, Dullenkopf A (2020) Non-invasive continuous blood pressure monitoring (ClearSight system) during shoulder surgery in the beach chair position: a prospective self-controlled study. BMC Anesthesiol 24(1):271
Joosten A, Desebbe O, Suehiro K, Murphy LS, Essiet M, Alexander B, Fischer MO, Barvais L, Van Obbergh L, Maucort-Boulch D, Cannesson M (2017) Accuracy and precision of non-invasive cardiac output monitoring devices in perioperative medicine: a systematic review and meta-analysis. Br J Anaesth 118(3):298–310
Scott MJ, Baldini G, Fearon KC, Feldheiser A, Feldman LS, Gan TJ, Ljungqvist O, Lobo DN, Rockall TA, Schricker T, Carli F (2015) Enhanced recovery after surgery (ERAS) for gastrointestinal surgery; part 1: pathophysiological considerations. Acta Anaesthesiol Scand 59(10):1212–1231
Ramsingh D, Alexander B, Cannesson M (2013) Clinical review: does it matter which hemodynamic monitoring system is used? Crit Care 17(2):208
Chen G, Zuo Y, Yang L, Chung E, Cannesson M (2014) Hemodynamic monitoring and management of patients undergoing high-risk surgery: a survey among Chinese anesthesiologists. J Biomed Res 28(5):376–382
Hendy A, Bubenek-Turconi Ş-I (2016) The diagnosis and hemodynamic monitoring of circulatory shock: current and future trends. J Crit Care Med (Targu Mures) 2(3):115–123
Nicklas JY, Saugel B (2017) Non-invasive hemodynamic monitoring for hemodynamic Management in Perioperative Medicine. Front Med (Lausanne) 4:209
Jackevičiūtė J, Kraujalytė G, Jaremko I, Stremaitytė V, Gudaitytė J (2019) Confronto di due tecniche di monitoraggio emodinamico continuo non invasivo in ambito perioperatorio. Acta Med Litu 26(1):31–37
Pour-Ghaz I, Manolukas T, Foray N, Raja J, Rawal A, Ibebuogu UN, Khouzam RN (2019) Accuracy of non-invasive and minimally invasive hemodynamic monitoring: where do we stand? Ann Transl Med 7(17):421
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, STROBE Initiative (2007) The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med 147(8):573–577
World Medical Association (2013) World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 310(20):2191–2194
Nelson G, Bakkum-Gamez J, Kalogera E, Glaser G, Altman A, Meyer LA, Taylor JS, Iniesta M, Lasala J, Mena G, Scott M, Gillis C, Elias K, Wijk L, Huang J, Nygren J, Ljungqvist O, Ramirez PT, Dowdy SC (2019) Guidelines for perioperative care in gynecologic/oncology: enhanced recovery after surgery (ERAS) society recommendations-2019 update. Int J Gynecol Cancer 29(4):651–668
Arora A, Jain K (2021) Enhanced recovery after surgery society recommendations for scheduled cesarean deliveries: is the developing world ready? Am J Obstet Gynecol 224(5):553–554
Peahl AF, Kountanis JA, Smith RD (2002) Postoperative urinary catheter removal for enhanced recovery after cesarean protocols. Am J Obstet Gynecol 222(6):634
Macones GA, Caughey AB, Wood SL et al (2019) Guidelines for postoperative care in cesarean delivery: enhanced recovery after surgery (ERAS) society recommendations (part 1, 2, 3). Gynecology 221(3):247–247
Kendrick JB, Kaye AD, Tong Y, Belani K, Urman RD, Hoffman C (2019) Liu H.J goal-directed fluid therapy in the perioperative setting. Anaesthesiol Clin Pharmacol 35(Suppl 1):S29–S34
Jackevičiūtė J, Kraujalytė G, Jaremko I, Stremaitytė V (2019) Comparison of two continuous non-invasive haemodynamic monitoring techniques in the perioperative setting. JActa Med Litu 26(1):31–37
Ghisi D, Garroni M, Giannone S, De Grandis G, Fanelli A, Sorella MC, Bonarelli S (2020) Melotti non-invasive haemodynamic monitoring with Clearsight in patients undergoing spinal anaesthesia for total hip replacement. A prospective observational cohort study.RM. Acta Biomed 91(4):e2020182
Ackland GL, Brudney CS, Cecconi M, Ince C, Irwin MG, Lacey J, Pinsky MR, Grocott MP, Mythen MG, Edwards MR, Miller TE (2019) Perioperative quality Initiative-3 workgroup; POQI chairs; physiology group; preoperative blood pressure group; intraoperative blood pressure group; postoperative blood pressure group. Br J Anaesth 122(5):542–551
Nelson G, Altman AD, Nick A, Meyer LA, Ramirez PT, Achtari C, Antrobus J, Huang J, Scott M, Wijk L, Acheson N, Ljungqvist O, Dowdy SC (2016) Guidelines for pre- and intra-operative care in gynecologic/oncology surgery: enhanced recovery after surgery (ERAS®) society recommendations—part I. Gynecol Oncol 140(2):313–322
Kehlet H, Bundgaard-Nielsen M (2009) Goal-directed perioperative fluid management: why, when, and how? Anesthesiology. 110(3):453–455
Noto A, Sanfilippo F, De Salvo G, Crimi C, Benedetto F, Watson X, Cecconi M, David A (2019) Noninvasive continuous arterial pressure monitoring with Clearsight during awake carotid endarterectomy: a prospective observational study. Eur J Anaesthesiol 36(2):144–152
Frank P, Logemann F, Gras C, Palmaers T (2021) Noninvasive continuous arterial pressure monitoring during anesthesia induction in patients undergoing cardiac surgery. Ann Card Anaesth 24(3):281–287
Rogge DE, Nicklas JY, Schön G, Grothe O, Haas SA, Reuter DA, Saugel B (2019) Continuous noninvasive arterial pressure monitoring in obese patients during bariatric surgery: an evaluation of the vascular unloading technique (Clearsight system). Anesth Analg 128(3):477–483
Bugarini A, Young AJ, Griessenauer CJ, Dalal SS, Schirmer CM, Vaughan S, Goren O (2021) Perioperative continuous noninvasive arterial pressure monitoring for Neuroendovascular interventions: prospective study for evaluation of the vascular unloading technique. World Neurosurg 153:e195–e203
Ameloot K, Van De Vijver K, Van Regenmortel N, De Laet I, Schoonheydt K, Dits H, Broch O, Bein B, Malbrain ML (2014) Validation study of Nexfin® continuous non-invasive blood pressure monitoring in critically ill adult patients. Minerva Anestesiol 80:1294–1301
Schramm P, Tzanova I, Gööck T, Hagen F, Schmidtmann I, Engelhard K, Pestel G (2017) Noninvasive hemodynamic measurements during neurosurgical procedures in sitting position. J Neurosurg Anesthesiol 29:251–257
Acknowledgements
None.
Funding
No funding or sponsorship was received for this study or publication of this article.
Author information
Authors and Affiliations
Contributions
ML, MP, CS and RV helped design the study, conduct the study, analyze the data, and write the manuscript. MC performed the statistical analysis. GP, AE, LGG and PS helped design the study and analyze the data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of our hospital (approval number 174 – February 2, 2022) and it was in accordance with the Declaration of Helsinki. The requirement for informed consent was waived because of the retrospective case–control nature of the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Loreto, M., Pisanti, M., Celentani, M. et al. Non invasive hemodynamic monitoring for fluids and blood resuscitation during placenta praevia accreta cesarean delivery: a retrospective observational study. J Anesth Analg Crit Care 2, 54 (2022). https://doi.org/10.1186/s44158-022-00083-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s44158-022-00083-2